
Abstract
Background: The purpose of this study is to characterize the distribution and radiographic features of vertebral hemangiomas (VH).
Methods: A retrospective Institutional Review Board- approved radiographic review of all vertebral hemangiomas diagnosed over a 2-year period was conducted at a singleinstitution academic medical center. Patient demographics and lesion-specific features were recorded. A novel system for mapping VH within the vertebra was utilized.
Results: Seven hundred twenty-six patients (age range: 12 to 97 years; mean: 59.1 years; ratio: 508:218 female-to-male) were found to have a total of 998 vertebral hemangiomas. VH were frequently multifocal (297 patients, 40.9%). VH were found to occur more frequently in the lumbar spine compared to the cervical and thoracic spines and sacrum (p < 0.001). VH more commonly occur in the superior aspects of the vertebral body (p = 0.048). Symptomatic cases were rare (2 cases, 0.2%).
Conclusions: VH are a frequent incidental finding on spinal imaging studies. Recognizing characteristic features and understanding their usual asymptomatic course may help prevent unnecessary clinical investigation.
Hemangiomas of bone are vascular lesions that frequently develop spontaneously in osseous structures and are widely recognized as behaving in a clinically benign manner. They are hamartomas consisting of an irregular overgrowth of capillaries, as opposed to true neoplasms. 1 Vertebral hemangiomas (VH) are among the most common primary lesions of the spine; most VH are incidentally discovered on spinal imaging. 2 Characteristic magnetic resonance imaging (MRI) findings are high signal intensity on both T1 and T2 sequences due to high fat and water content, respectively. 3 Computed tomography (CT) scan will reveal a polka-dotted vertebra due to the thickened trabeculae. Due to their benign nature, intervention is rarely required. Rarely VH can become symptomatic if they extend into the epidural space, cause a compression fracture, or cause osseous expansion leading to nerve root compression. 3 However, because less than 1% of lesions are symptomatic, 4 further workup is seldom required. The purpose of this study is to further characterize the radiographic features and geographic distribution of VH to help prevent unnecessary testing or referral for these benign lesions.
Materials and Methods
An institutional review board-approved retrospective review of spinal imaging was conducted at an academic medical center. All radiological reports of spinal MRIs and CT scans from January 1, 2009, to December 31, 2010, were searched for diagnosis of vertebral hemangioma using a Radiology Information System (RIS) query. Previously reported diagnostic criteria were applied to 683 MRIs and 43 CT scans, which were retrospectively reviewed to confirm the diagnosis of vertebral hemangioma. The criteria for diagnosis of VH were the presence of a lesion with moderate to markedly increased signal on T1-weighted images and moderate to markedly increased signal on T2-weighted images. 3 , 5 Patient demographics, VH location, and the involved spinal level were recorded for each lesion.
Lesion volume was calculated using measurements obtained on sagittal and axial images. If a corresponding axial image was not available, the lesion width was estimated by multiplying number of consecutive sagittal images demonstrating the lesion by slice thickness. Volume was estimated in mm 3 by multiplying these values. Volume analysis only included MR images due to the greater precision in measurement available compared to CT images.
Chi-square analysis was performed to compare the frequency of VH occurrence between vertebral level groups. The frequency of occurrence was obtained by dividing the number of lesions in a group by the number of vertebra in the group multiplied by the patient population. ANOVA testing was used to compare volumes between vertebral level groups.
Locations of VH within a vertebra were recorded using a novel geographic map (Fig. 1). The vertebral body was hemi- sected in the sagittal, axial, and coronal planes to create an 8-section grid within the body. Numbering began at the left superoanterior aspect of the body (“area 1”) and continued in a left-to-right and anterior-to-posterior manner. Posterior elements, including pedicles, transverse processes, and spinous processes, were similarly assigned numbers.

The vertebra is divided into 13 geographic areas. Area 8 (the right inferoposterior area) is not shown.
Results
The review revealed 726 unique patients and 998 total VH. There were 508 women (70%) and 218 men (30%), an approximate 3:1 female to male ratio. The average patient age was 59.1 years with a range of 12 to 97 years. VH most commonly occurred in patients between the ages of 51 to 60 years (Fig. 2).

The overall age range is 12 to 97 years. Vertebral hemangiomas were most frequently seen in the patients ranging in age from 51 to 60 years
Vertebral hemangiomas were frequently multifocal. Of 726 patients, 297 (40.9%) had VH involving multiple levels. Forty-five patients (6.6%) had VH involving three or more vertebral levels, with one patient demonstrating them in six contiguous levels (T11-L4).
Hemangiomas were found at every spinal level but appeared most frequently in the lumbar spine (Fig. 3). VH distribution included 81 in the cervical spine (8.1%), 392 in the thoracic spine (39.3%), 479 in the lumbar spine (48%), and 46 in the sacral spine (4.6%). VH occurred significantly more frequently in the lumbar spine (13.2% of lumbar vertebra) compared to the cervical spine (1.6%, p < 0.001), the thoracic spine (4.5%, p < 0.001), and the sacrum (1.3%, p < 0.001).
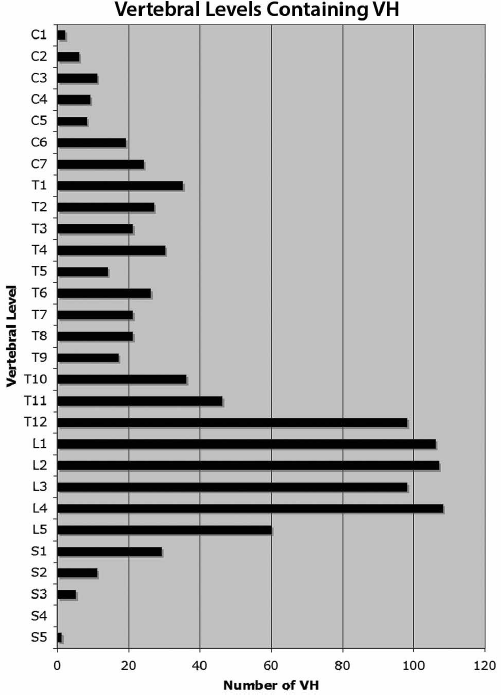
The overall number of vertebral hemangiomas at each level is demonstrated. There is a marked increase in presence of lesions beginning at T12 and tapering off at L5.
Average volume increased with caudal descent in the spine, demonstrating the largest volume in the lumbar spine (cervical spine: 739 mm3; thoracic spine: 1,509 mm3; lumbar spine: 2,385 mm3; sacral spine: 1,229 mm3). VH volume was significantly greater in the lumbar spine compared with other groups (p < 0.001).
Most lesions were contained within the vertebral body and did not involve the pedicles or other posterior elements (Fig. 4). The majority of VH, 52.4%, were contained within a single geographic area within the vertebral body as opposed to multiple areas (p = 0.49). Of those contained in a single zone, VH were more likely to be contained in the superior aspect of the vertebra: zones 1 to 4 contained 338 (64.9%) of VH restricted to one zone (areas 1 to 4 versus areas 5 to 8, p < 0.001). Thirteen lesions extended into a single pedicle (areas 9 and 10). Two were contained entirely within the spinous process, and one was involved in a transverse process.

Vertebral hemangiomas were present in all geographic areas and frequently occupied adjacent areas, both laterally and vertically. They were more likely to be confined to a single area (p = 0.048). Of those confined to single areas, they were more likely to occur in the superior areas (1 to 4) than the inferior areas of the body (5 to 8, p < 0.001). This figure does not demonstrate the posterior elements due to the relative infrequence of their presence in area 9 to 13.
All lesions fit the described imaging criteria, and 793 lesions (83.6%) lost signal intensity on short tau inversion recovery (STIR). The vast majority of lesions reviewed were found incidentally and were not sampled. Two hemangiomas were clinically symptomatic. One patient with a clinical complaint of back pain demonstrated lesion extension into the posterior elements, producing intervertebral foraminal stenosis. One hemangioma resulted in significant osseous destruction for which resection and vertebral fusion were necessary.
Discussion
Vertebral hemangiomas are common, generally asymptomatic entities that are well-recognized within the orthopaedic literature. Nevertheless, they are frequently confused for more ominous lesions, and patients are frequently referred to subspecialists, such as orthopaedic oncologists or spine specialists for evaluation, underscoring a lack of appreciation for their benign nature. While simple VH have a characteristic appearance, compressive VH often display a mottled high-intensity signal on T1-weighted imaging. Compressive VH should, thus, be distinguished from other lesions that demonstrate a coarse reticular pattern with epidural extension such as hemangioblastoma, lymphangioma, and Ewing’s sarcoma. Of these lesions, however, only VH will show high intensity on both T1- and T2-weighted MRI.
Vertebral hemangiomas are usually slow-growing lesions that histologically demonstrate an overgrowth of blood vessels within bone trabecula and frequently contain adipose tissue. 2 Histological correlation of VH with lesions found on MRI has previously demonstrated that T1-hyperintensity corresponds to an increased proportion of adipocytes in the lesion, whereas marked T2-hyperintensity corresponds with a vascular predominance. 3 , 6 , 7 The majority of lesions reviewed (83.6%) lost signal intensity on STIR, suggesting that overgrowth of adipose tissue is more frequently associated with hemangiomas than a vascular predominance. This increase in adiposity is considered a reactive rather than a neoplastic process. 8
A novel mapping system was utilized to clearly and accurately localize a given lesion’s position within the bone. Previously reported spinal tumor mapping systems include the Weinstein-Boriani-Biagini classification 9 ; however, this system is largely designed to describe extraosseous tumor expansion, an event that is extremely rare with VH. The currently described mapping system demonstrated that while VH occur in every area of the vertebral body, they are more commonly confined to the superior aspect of the vertebral body, with no predilection for laterality.
Incidence of VH have been variously reported. Two relatively recent radiographic reviews of consecutive spinal MR images reported widely different incidences. One study of 782 consecutive images found an incidence of 26.9%. 10 A similar retrospective study reviewing incidental findings confined to lumbar spine in 1,268 patients found a VH incidence of only 1.5%. 11 Although the present study does not comment on incidence, it does support previous reports of common multilevel involvement and a female predominance. Barzin and coworkers found multilevel VH in 33% of cases, consistent with the present finding of multifocal involvement in 36.8% of patients. 11 The same study found VH to occur more frequently in females than males (30% compared to 23%). Studies with smaller patient populations also found VH more commonly in females. 12 , 13 The 3:1 female to male ratio we found, while consistent with the general notion of female predominance, is more pronounced than previously reported.
The present study found that 0.2% of reviewed cases demonstrated symptomatic lesions, consistent with previous reports supporting that symptomatic VH are rare. Furthermore, only one case required operative intervention. A previous study assessing 35 asymptomatic VH found that two lesions progressed to eventually cause neurological deficits. Pain preceded neurological deficit in both cases and the investigators recommended long-term follow-up for only those patients in which the VH caused pain. 13 In the same study, 9 of 11 VH causing neurological deficits requiring intervention extended beyond the vertebral body into the posterior elements or involved the entire vertebra, suggesting a need for increased vigilance in lesions extending beyond the body. Posterior element extension was found in 1.6% of VH in the present study, and of these, 1 of 16 produced symptomatic stenosis. This suggests that while posterior element extension is uncommon, a relatively higher proportion of lesions extending into the pedicles may be symptomatic compared to those contained within the vertebral body. Symptomatic VH has been shown to more frequently occur in the thoracic spine, as was the case with both symptomatic lesions observed in the current study. 12 , 14
There are several limitations to this study. It was a retrospective observational imaging study, which did not consider subsequent clinical encounters. Therefore, progression from asymptomatic to symptomatic findings could not be evaluated. Furthermore, histological correlation of all but the two lesions that required surgical intervention was not feasible; the diagnoses were made purely on imaging criteria.
In conclusion, this study represents a large retrospective characterization of VH using a novel geographic mapping system. The current findings underscore the overwhelmingly benign and incidental nature of VH, and reinforce that in the absence of symptoms, further clinical evaluation is rarely necessary.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.