
Abstract
Background
Early determination of hospital discharge destination is critical for adult patients hospitalized with pathologic fractures as they require attentive postoperative multidisciplinary care. There is a paucity of studies that investigate risk factors for non-home discharge in this vulnerable patient population. This study aimed to examined the impact of health insurance type and New York State region on hospital discharge disposition for adult patients admitted with pathologic fractures.
Methods
The New York Statewide Planning and Research Cooperative System (SPARCS) database identified 1133 patients aged 18 years and older admitted to a public or private hospital in New York state between January 1st of 2020 and December 31st of 2022 with pathologic fractures. Multinomial logistic regression analysis was used to examine the relationship between insurance type or New York State region and discharge disposition (inpatient/skilled nursing facility, hospice, compared home or home with home health services). The model accounted for potential confounders, including age, sex, race, severity of illness, and risk of mortality.
Results
Compared to patients with commercial insurance, patients with Medicare were 2.7 (95% CI, 1.4-5.2) more likely to be discharged to inpatient rehabilitation or skilled nursing facility than home. Compared to patients with commercial insurance, patients with Medicare were 2.7 (95% CI, 1.2-6.1) and patients with Medicaid were 2.5 (95% CI, 1.0-6.2) more likely to be discharged to hospice than home. Compared to patients in New York City, patients in the Hudson Valley region were 2.3 (95% CI, 1.3-4.1) more likely to be discharged to in-patient rehabilitation or a skilled nursing facility than home. Patients in Long Island were 1.9 (95% CI, 1.1-3.2) and Hudson Valley were 4.2 (95% CI, 2.0-8.6) more likely than those in New York City to be discharged to hospice. Patients in Central New York (RRR 2.7, 95% CI 1.3-5.5) were more likely to expire during the hospitalization than patients in New York City.
Conclusions
Our study found Medicare or Medicaid payor status were significant predictors of hospital discharge disposition for adult patients hospitalized with pathologic fractures. Regional variance exists across New York State which may reflect access to care and historical patterns of care. High-quality care coordination is critically important for cancer patients whose care extends longitudinally from hospital acute care to ambulatory care and involves multiple medical specialties.
Level of Evidence
Level III, Diagnostic Study.
Introduction
The prevalence of patients living with metastatic carcinoma affecting the musculoskeletal system is increasing. Pathologic fractures occur in approximately 10% of patients with metastatic carcinoma to bone and many will require surgical intervention by orthopedic surgeons. 1 The medical and surgical complexity of caring for these patients requires a multidisciplinary approach. 2 There is a growing body of evidence regarding differences in perioperative and postoperative morbidity and mortality for this patient population compared with the traumatic injuries.3-6 Some of these analyses have included discharge disposition as secondary outcomes but there is a paucity of data on determinants of discharge type for this vulnerable patient population. For example, a NSQIP study of 30 866 patients who underwent surgical treatment for pathologic or native humerus fractures reported patients with pathologic fractures were more likely to be discharged to facilities (22.3% compared to 13.5%). 4 A propensity-score matched analysis of 29 541 geriatric patients with hip fractures from the Registry for Geriatric Trauma of the German Trauma Society did not find differences in non-home discharge between surgically managed osteoporotic and pathologic hip fracture patients. 7 The ability to predict discharge disposition following hospitalization for pathologic fractures may aid in improving efficiency in care coordination for admitted patients as well as post-acute care monitoring efforts and therapies. These data may also provide more accurate preoperative counseling for patients and their families. The decision to discharge patients to a non-home destination is multifaceted and involves assessment of disease progression, functional status, anticipated postoperative interventions, and support systems. For example, patients with progressive, disseminated cancer may require hospice care, whereas patients pursuing radiation may benefit more from discharge home to minimize treatment delays. Inpatient costs associated with skeletal related events, which include pathologic fractures, are significant.8,9 A study of admitted patients with multiple myeloma and metastatic breast and prostate carcinoma using MarketScan commercial and Medicare databases reported a mean length of stay of 5.9 to 11.6 days and mean payments per admission from $22,390 to $59,854 in June 2009 dollars. 10 Examining 2011-2015 Medicare data, Li et al analyzed 7988 patients with bone metastases and 4277 patients with multiple myeloma discharged after a skeletal related event hospitalization and reported 40.3% and 45.5% patients were discharged to institutional post-acute care facilities; these percentages are higher than the general Medicare population which was 26.3% in 2015.11,12 There are discrepancies in the literature, however, in the rates of non-home discharge disposition for this patient population.3,13
The purpose of this study was to examine determinants of discharge disposition of admitted adult patients with pathologic fractures. The New York Statewide Planning and Research Cooperative System (SPARCS) database offers a unique opportunity to examine acute-care patient disposition. We hypothesized that SPARCS data would demonstrate variation in discharge disposition based on insurance payor and New York state region following hospital admission for adult patients with pathologic fractures.
Methods
Study Design and Setting
This study used the SPARCS database to identify 1,133 patients aged 18 years and older admitted to a public or private hospital in New York state between January 1st of 2020 and December 31st of 2022 with pathologic fractures. SPARCS is an all-payor administrative database that collects patient data from all non-federal acute care facilities in the state (100 hospitals in the dataset queried). Patients were identified by the diagnosis related group “Initial encounter for pathologic fracture” (APR-DRG 343), which includes appendicular and axial pathologic fractures.
Variables, Outcome Measures, and Data Sources
The primary outcome was patient discharge disposition, which collapsed into 5 categories: discharge to home or home with home health services (HHS), discharge to facility, discharge to inpatient rehabilitation or skilled nursing facilities (SNF), hospice discharges, and in-hospital deaths. “Discharge to facility” included cancer center, Medicaid certified nursing facility, Medicare certified long term care hospital, psychiatric hospital, short-term hospital, facility with custodial support, and hospital-based swing bed.
Demographics, Description of Study Population
Baseline patient information collected included age, sex, race (White, Black, Other), severity of illness (low/high), risk of mortality (low/high), New York State region, and primary payor (commercial, Medicare, Medicaid). Severity of illness and risk of mortality were classified into 4 categories (minor, moderate, major, extreme) using APR-DRG classifications. Due to low frequencies in the minor and extreme groups, they were collapsed into 2 levels: low (minor/moderate) and high (major/extreme) for improved estimation. Commercial payor included private insurances, Blue Cross/Blue Shield, and Managed Care. Other payor included federal, state, local Veteran’s Health Insurance, miscellaneous/other, and self-pay. Median total charges, costs, and lengths of stay were examined and stratified by insurance provider and hospital location.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics. Categorical variables were reported as frequencies and percentages. Due to the skewed distribution of total charges and total costs, these variables were summarized using the median and interquartile range (IQR). Multinomial logistic regression was used to assess the association between insurance type and patient discharge disposition with home or HHS as the base outcome category. All predictors were first assessed for multicollinearity and interaction with (1) insurance type and (2) New York State region. A forward stepwise selection method was used to add predictors into the full model to account for confounding. The final model included age group, sex, insurance type, New York State region, severity of illness, and risk of mortality and was expressed as Relative Risk Reductions (RRRs) with 95% confidence intervals. To examine the potential impact of the COVID-19 pandemic, a variable reflecting year, 2020 compared to 2021-2022 was also included in the full model and had no effect. All statistical analyses were conducted using Stata SE 18.5 (College Station, Texas, 2023). Statistical significance was determined using a two-tailed alpha level of 0.05. To ensure compliance with data use regulations, small cell counts (<10) are not reported in the analyses. Ethical approval for this study was obtained from the institutional review board (IRB Protocol #23772) at New York Medical College, Valhalla, NY.
Results
Descriptive Characteristics of the Study Population, SPARCS-New York 2020-2022

*“Commercial” category in primary payer includes Blue Cross/Blue Shield, Managed Care, and Private Health Insurance.
*“Missing/Other” category in primary payer includes Federal/State/Local/VA, Miscellaneous/Other, and Self-Pay.
*“Western NY” category includes Finger Lakes, Western NY, and Southern Tier.
*“Facility” under patient disposition includes Cancer Center, Medicaid Cert Nursing Facility, Medicare Cert Long Term Care Hospital, Psychiatric Hospital, Short-term Hospital, Facility w/Custodial/Supportive Care, and Hospital-based Medicare Swing Bed.
*“Missing/Unknown” under patient disposition includes Another Type Not Listed and Left Against Medical Advice.
*“Low” category under severity of illness and risk of mortality includes minor and moderate severity/risk.
*“High” category under severity of illness and risk of mortality includes major and extreme severity/risk.
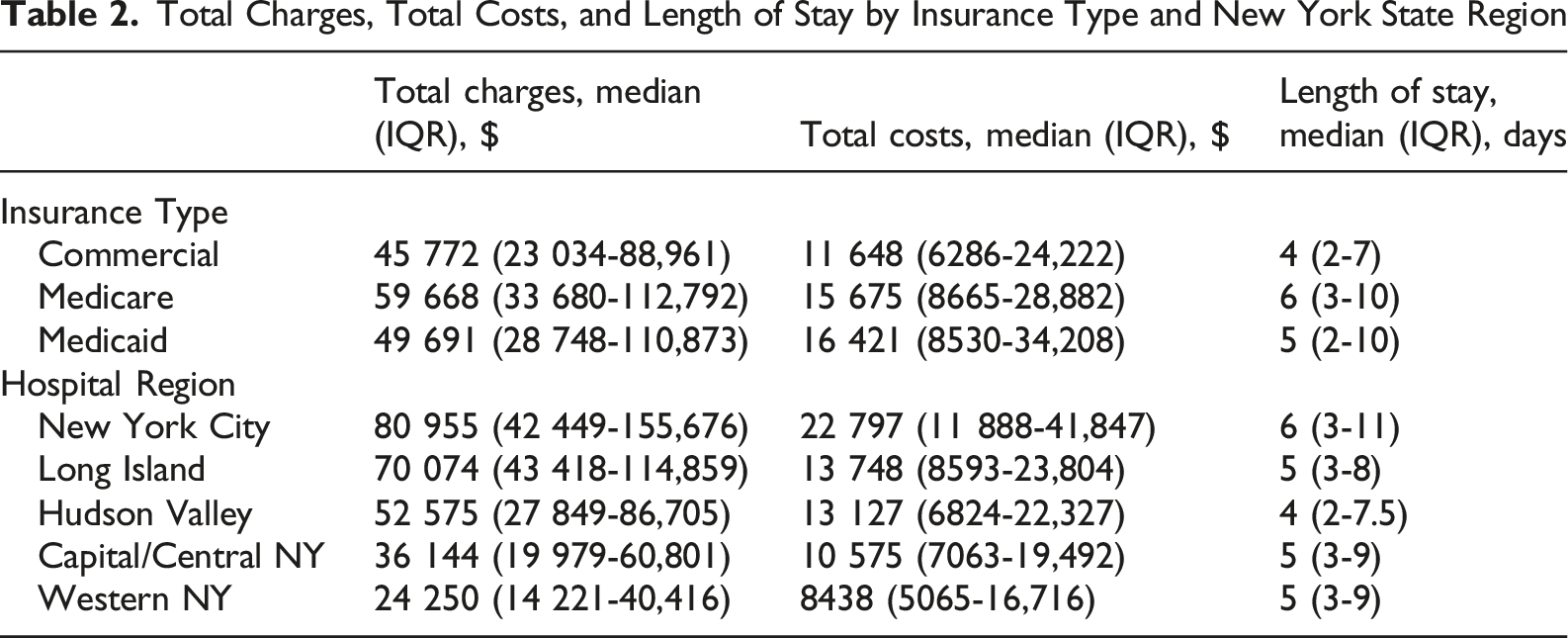
Total Charges, Total Costs, and Length of Stay by Insurance Type and New York State Region
Multinomial Model for Patient Disposition

Data Source: SPARCS-New York 2020-2022.
Regional differences in discharge disposition were detected for inpatient rehabilitation or SNF, hospice, and mortality during hospitalization. No differences were detected for discharge to facility as compared to home or HHS across the 5 state regions. With New York City as the comparison group, patients treated in the Hudson Valley region were more likely (RRR 2.6, 95% CI 1.2-4.1, P < 0.01) to be discharged to inpatient rehabilitation or SNF than home or HHS. Patients treated in Long Island (RRR 1.9, 95% CI 1.1-3.2, P < 0.05) and the Hudson Valley (RRR 4.1, 95% CI 2.0-8.6, P < 0.01) were more likely than those treated in New York City to be discharged to hospice than home or HHS. Relative to New York City, patients treated in Central New York were more likely (RRR 2.7, 95% CI 1.3-5.5, P < 0.01) to expire during the hospitalization rather than be discharged home or HHS.
Patient age further contributed to the multinomial model when comparing home or HHS with in-patient rehabilitation and SNF disposition. Compared to patients 18 to 49 years old, those 70 year or older were 4.7 (95% CI 1.5-14.7, P < 0.01) times more likely to be discharged to a rehabilitation facility rather than home. The SPARCS indexed variables of severity of illness and risk of mortality also contributed the model. For both variables, minor and moderate levels were classified as low; major and extreme were classified as high. Compared to the low reference group, patients with high severity of illness were more likely to be discharged to hospice (RRR 2.2, 95% CI 1.2-4.1, P < 0.05) and expire during the hospitalization (RRR 3.7, 95% CI 1.2-11.4, P < 0.05) than home or HHS. Compared to the low reference group, patients with high risk of mortality were more likely discharged to inpatient rehabilitation or SNF (RRR 1.7, 95% CI 1.2-2.5, P < 0.01), hospice (RRR 4.0, 95% CI 2.4-6.8, P < 0.01), and expire (RRR 12.3, 95% CI 4.6-33.1, P < 0.01) than home or HHS.
Discussion
Post-acute care disposition is a complex undertaking in the management of pathologic fractures. These patients may present with poor prognoses and require coordinated ambulatory care across many medical specialties. Moreover, non-home discharge disposition is layered in patient and community factors. This study identified adult patients admitted with pathologic fractures from the SPARCS database to investigate risk factors for specific discharge destinations. The findings of this study were: (1) compared to patients with commercial payors, Medicare patients were more likely to be discharged to inpatient rehabilitation or SNF than home; Medicare and Medicaid patients were more likely to be discharged to hospice than home; (2) regional differences in discharge disposition were detected for inpatient rehabilitation or SNF, hospice, and death during the acute care hospitalization; (3) higher severity of illness or risk of mortality patients were more likely to be discharged to hospice or expire during the hospital encounter compared to a home disposition.
This study found that patients with Medicare were more likely to undergo discharge to a non-home facility such as inpatient rehabilitation center or skilled nursing facility than patients with commercial insurance. Patients with Medicare and Medicaid were more likely to be discharged to hospice than home as compared to patients with commercial payors. Although Medicaid coverage of inpatient rehabilitation for trauma patients varies by state, discharge destination often depends on the type of care needed during the post-discharge period. 14 The needs of patients with pathologic fractures differ from that of the typical post-fracture fixation patient and therefore inpatient rehabilitation may not be the most feasible discharge option. For example, patients requiring chemotherapy may not always be candidates for inpatient rehabilitation.15,16 Current guidelines recommend immediate assessment of candidacy for radiotherapy either pre or post pathologic fracture fixation. 17 A 2011 to 2017 NSQIP analysis of 67 548 patients with hip fractures reported those with pathologic fractures had significantly longer length of stay greater than 5 days, higher rates of venous thromboembolic disease, 30-day readmission, 30-day mortality, but were less likely to be discharged to a non-home location. 13 This study was unable to capture data regarding 30-day readmission or mortality rates but found insurance payor to be predictive of a non-home discharge destination. This finding may reflect a decreased illness severity profile in patients with commercial insurance as compared to those with Medicare or Medicaid. Whereas Medicare patients are older and may have widespread or progressive metastatic bone disease, perhaps declining further treatments, as evidenced by higher likelihood of discharge to hospice.18,19 Additionally, patients with Medicare may have less social support or transportation access which may limit the ability to transition to home discharge immediately following acute care.
We also identified differences in discharge destinations based on geographic location within New York State. Previous studies have demonstrated variations in resource utilization and outcomes following orthopedic surgery. One study found that the utilization of rotator cuff repair was decreased in the Northeast, compared with the South, Southwest, and Southeast. 20 An analysis of a national Medicare database demonstrated that the rate of total knee arthroplasty utilization was increased in states where patients had fewer outpatient visits such as the upper Midwest, Great Plains, and Mountain West regions. 21 Another study analyzing a Pennsylvania state database demonstrated that Black patients were more likely to be discharged to non-home destination following total joint arthroplasty. 22 A 2018 study using Medicare data showed that patients from the South and Northeast had a higher likelihood of being discharged to non-home destinations following orthopedic surgery. 23 Our study is the first to demonstrate differences in discharge destination based on geographic location following admission for pathologic fractures. Specifically, patients admitted to hospitals in the Hudson Valley region were more likely to be discharged to inpatient rehabilitation and hospice care compared to patients cared for in New York City. These regional practice variations may reflect differences in access to care or discharge planning practices among hospitals. New York City represents an urban environment with a high concentration of tertiary referral centers, cancer hospitals, and post-acute care facilities. Long Island and the Hudson Valley are suburban regions with mixed community hospitals, and moderate SNF availability. In contrast, Central and Western New York include more rural areas with lower hospital density, fewer specialty centers, and a greater reliance on regional referral networks. These structural differences may contribute to variation in discharge practices, resource availability, and access to hospice or rehabilitation services across the state. 24 Moreover, patients with sufficient social support may be discharged home rather than to facility.25,26 Several additional patient factors were influential in discharge disposition including age, illness severity, and mortality risk score. Increasing age is well-known to predispose patients to discharge to non-home destinations.27,28 The current analysis found age older than 70 was associated with increased risk of discharge to inpatient rehabilitation or SNF. This finding may reflect common age-related physiologic impacts on functional status, such as a decreased functional reserve capacity, reduced cardiopulmonary function, and age-related sarcopenia.29,30 In the subset of patients who are admitted with pathologic fractures, this illness-induced frailty may be exacerbated and contribute to an increased need for rehabilitation following discharge.
Our study also found that patients insured by Medicare and Medicaid had greater median total charges, costs, and longer lengths of stay. This is likely a reflection of a higher complexity of care associated with an older or more socially vulnerable patient population. We also observed regional differences, with hospitals in New York City and Long Island demonstrating higher charges, costs, and lengths of stay. Similarly, this may be attributed to the high concentration of referral centers in these areas with a greater utilization of specialized services in oncology. 31
This study has several limitations. First, due to the nature of the SPARCS dataset, we were unable to distinguish between axial and appendicular, articular and extraarticular, lower and upper extremity fractures, or presence of multiple fractures. This analysis was based on the diagnosis code as pathologic fracture but the SPARCS dataset does not include histopathology, whether there was a primary cancer diagnosis, staging, prior oncologic management, or treatment data; therefore, this study includes patients treated with and without surgery. There are no prior studies that compare appendicular and axial pathologic fracture discharge disposition after admission; therefore, the impact of the heterogenicity of this cohort is unknown. We feel there is value, however, in assessing the aggregate experience of this patient population as many of the treatment paradigms are similar between diagnoses. It is, however, important to consider these data as heterogeneous in diagnosis and treatment.
Second, the SPARCS dataset does not include information about social support, baseline functional status, or patient preference; all which might influence discharge destination. Specifically, because socioeconomic measures such as the Area Deprivation Index are not captured in SPARCS, we were unable to account for neighborhood-level disadvantage, which may meaningfully influence discharge disposition. These are areas for future research.
Third, the current study used the SPARCS dataset as cross-sectional data. It would be valuable to examine the determinants of discharge from the acute care setting and the impact of the ambulatory care. For example, do these patients experience a delay in radiation treatment if discharged to inpatient rehabilitation or SNF as compared to home or HHS? Further, we were unable to capture 30-day readmissions or 30-day mortality in this analysis. This analysis was limited to New York State and discharge practices differ among various hospital systems around the country. 32 We also lacked detailed information about patients’ specific insurance plans, including New York Medicaid, Medicare Advantage, and dual-eligible Medicare-Medicaid, all of which differ in coverage of medical services. We also could not stratify by Medicare patients with kidney disease, and Medicare recipients due to disability. This study was performed over a limited number of years which may be useful to minimize the contributions of changing practice patterns but also resulted in a smaller number of subjects. Finally, there may be additional variables unavailable in the SPARCS dataset that contribute to discharge distribution, including data on whether patients were transferred to another hospital for further specialized care.
Conclusions
Early discharge planning for patients presenting with pathologic fractures is critical, as they require multidisciplinary care following discharge. This study analyzed risk factors for discharge disposition following admission for pathologic fractures using a statewide database. We found that insurance payor, New York state region, age, disease severity, and mortality risk were significant predictors of discharge. Medicare payor and older age were risk factors for discharge to a non-home facility as compared to commercial payor. Analyses of this patient population are important as the complexity of their care differs significantly from non-oncologic fractures. Such nuances are important for clinicians, patients and families, hospital administrators, insurance companies, and state and federal agencies. Future studies should aim to incorporate clinical data such as histopathologic diagnosis, stage, preinjury functional status, fracture location, and treatment modality, into identifying predictors of discharge; furthermore, it would be interesting to evaluate the impact of discharge disposition on mortality, future skeletal related events, and patient reported outcomes.
Footnotes
Ethical Considerations
The protocol Discharge Destination of Pathologic Fractures: A State Database Analysis, Westchester Medical Center, 23772 has been verified by the New York Medical College General Medical and Behavioral IRB as Exempt according to 45CFR46.101(b) (4): (4) Secondary Research Uses of Data or Specimens on 11/13/2024. The following items associated with this protocol have been approved: Protocol 10/14/2024 SPARCS_IRB_10.14.2024.docx (10.14.2024) Pre-Application Questionnaire 09/27/2024 Pre-Protocol Questionnaire.pdf Approved Application 11/14/2024 SPARCS_IRB_10.14.2024.docx (10.14.2024) This email constitutes New York Medical College’s permission to initiate the referenced study.
Author Contributions
ARC: Conceptualization of the study, supervision of the research process, manuscript editing, and manuscript preparation. JA: Data analysis, and manuscript writing. ED: Data analysis, manuscript editing, and manuscript preparation. VK: Data retrieval, study conceptualization, manuscript preparation, and manuscript editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study is publicly available and deidentified.