
Abstract
Background: There is a limited amount of data on the long-term function and quality of life of children who sustain gunshot injuries to the extremity. Many complications, such as physeal arrest and limb-length discrepancy, take months or years to manifest. The purpose of this study is to characterize clinical features and long-term outcomes of pediatric patients with firearm injuries to the extremities.
Methods: A retrospective review of the trauma registry at an urban Level 1 trauma center was performed in which 27 patients ranging in age from 14 to 18 years old who were admitted between January 2011 and March 2014 for management of extremity firearm injuries were identified. Demographic data, injuries, Injury Severity Score (ISS), and hospital course were obtained through chart review. Patients who were followed up after the review commenced completed the 36-Item Short Form Health Survey (SF-36) and Childhood Trauma Screening Questionnaire (CTSQ).
Results: Twenty-seven pediatric patients with an average age of 17 years (SD ± 0.94 years) were identified with 33 gunshot wounds (GSWs): 7 upper extremity and 26 lower extremity. Seventeen patients sustained at least one fracture, with a total of 20 fractures. Six (30%) of the fractures were treated operatively. Peripheral nerve injury (N = 4) was the most common complication. There were no cases of infection, compartment syndrome, vascular injury, physeal fracture, growth disturbance, or angular deformities. The mean length of follow-up was 132 days (N = 18, range: 2 days to 2.95 years). The mean SF-36 Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were 48.7 (N = 3, range: 44.0 to 56.2) and 58.2 (N = 3, range: 51.3 to 62.2), respectively. The mean CTSQ score was 4.67 (N = 3, range: 4 to 5).
Conclusion: Pediatric patients with extremity GSWs reported below-average physical health and above average mental health relative to SF-36 age and gender-controlled national norms. CTSQ scores were not predictive of future post-traumatic stress disorder. Outpatient follow-up for pediatric GSW is a concern because most complications, including deformity and limb-length discrepancy, occur months to years after the injury.
Firearm injuries for adolescents and children result in approximately 21,000 Emergency Department (ED) visits and over 3,000 deaths annually. 1 As a result, in 2012 an American Academy of Pediatrics policy cited firearm injuries as one of the top three causes of death among children and the cause of one in four deaths among adolescents ages 15 to 19 years. 2 , 3 Firearm injuries cause significant morbidity and mortality to children and adolescents annually.
In regards to firearm injuries to the extremities, there is a paucity of literature describing the long-term effects of osseous injury and the resulting functional limitations in the pediatric population. For adolescents between 14 and 17 years old, 183 of 2,066 ED visits at an urban Level 1 trauma center were due to firearm injuries to the extremities. 4 It is known that firearm injuries to the extremity in pediatric patients are associated with fractures and frequently require surgery. 5 , 6 Additionally, it is not uncommon to have associated abdominal, neurologic, or vascular injuries. 7 Several studies have characterized the epidemiology, social circumstances, and hospital course of these patients, but also cited poor follow-up and did not describe long-term function. 8 - 10
At this time, the long-term complications from firearm injuries to the extremities in the pediatric population are not well described. These complications may take months to years to manifest. The purpose of this study is to characterize clinical features and long-term outcomes of pediatric firearm extremity injuries. The investigators aimed to qualify the osseous injuries through retrospective review of treatment records and radiographic imaging as well as quantify the functional status of the patient after firearm injury using a functional assessment questionnaire. The investigators hypothesized that firearm injuries to the extremities among pediatric patients would be associated with long-term effects on patient functional status.
Materials and Methods
Study Setting
The study was conducted at a 477-bed, Level 1 trauma center in an urban setting. It is a university-affiliated teaching hospital with approximately 2,000 trauma admissions per year serving a population of 424,148 in its primary service area, with an additional 469,309 people within secondary service areas. Primary service area is defined as zip codes that provide 50% of the institute’s patients, while secondary service area is defined as the zip codes that provide the next 25% of the institute’s patients. The population served has an average annual income of $37,684 with 30.6% below the national poverty line. 11 , 12
Study Design and Chart Review
After Institutional Review Board approval was obtained, a retrospective review of the hospital trauma registry was performed. The Institutional Review Board approved a review for patients aged 14 years or older. Inclusion criteria included patients ranging in age from 14 to 18 years old who were admitted following a firearm injury to one or more extremities with ICD9 codes E922, 922.0, 922.1, and 922.9 in the 39-month study period from January 2011 through March 2014. Exclusion criteria included all patients discharged directly from or who died in the ED. Data obtained from the electronic medical record included age, sex, ethnicity, Injury Severity Score (ISS), total hospital length of stay (LOS), Surgical Intensive Care Unit length of stay (SLOS), procedures performed, associated complications as defined by the National Trauma Data Bank (NTDB), 13 and length of follow-up. Study outcomes included the time to follow-up, the 36-Item Short Form Health Survey (SF-36), and Childhood Trauma Screening Questionnaire (CTSQ). Analysis was performed using descriptive statistics because there was no control or comparative study cohort.
Results
Demographics
Twenty-seven pediatric patients with an average age of 17 years (SD ± 0.94 years) were identified with 33 gunshot wounds (GSWs). There was a total of 7 upper extremity and 26 lower extremity GSWs. The study population included 21 males and 6 females (3.5:1 ratio) of whom 21 identified as African American and 5 as Other (one patient’s race was unknown), (Table 1).
Study Population Demographics

Fracture Patterns

Outcome Score Data

The mean hospital length of stay (LOS) was 3.5 days (SD ± 4.1 days). Six patients required intensive care unit (ICU) level care, for whom the mean ICU LOS was 4.1 days (SD ± 3.0). The mean ISS was 5.8 (SD ± 5.4).
Clinical Features
Seventeen patients sustained at least one fracture (63%), accounting for a total of 20 fractures in the study population altogether. Fracture locations included fibula (5), tibia (4), femur (3), ulna (2), metacarpal (2), humerus (1), radius (1), metatarsal (1), and calcaneus (1), (Table 2).
Operative treatment was required for six (30%) of the fractures, all of which were isolated to the lower extremities. The remainder of the fractures were treated non-operatively. Peripheral nerve injury (N = 4) was the most common complication. There were no cases of infection, compartment syndrome, or vascular injury. Figures 1 through 4 display representative radiographs of a case of a 17-year-old male with a gunshot wound to the right thigh resulting in a right midshaft femur fracture.

Postoperative radiographs status post anterograde intramedullary nailing showing a comminuted, displaced right midshaft femur fracture with a bullet retained in the thigh. A right tibial traction pin was placed under sedation, and 13 pounds of traction was applied.
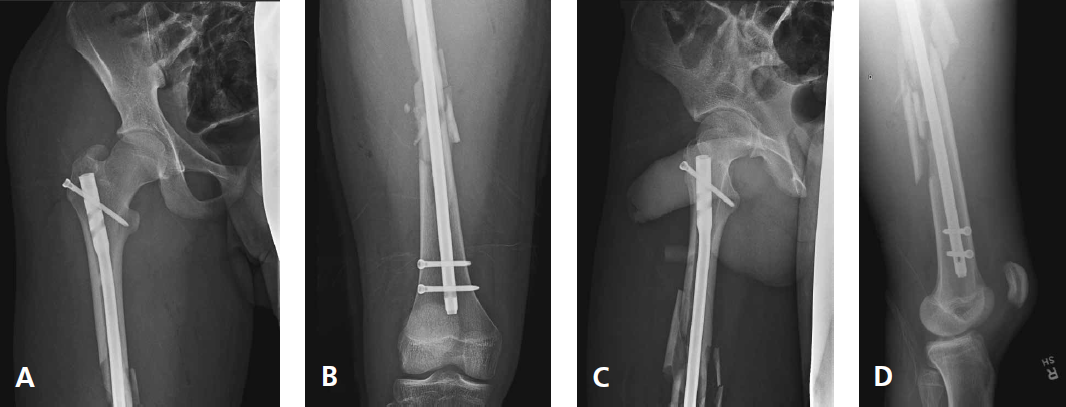
On hospital day 1, the patient underwent placement of an anterograde long intramedullary nail in the right femur via a greater trochanter entry point as well as bullet removal from the thigh. Postoperative radiographs are shown.

The patient was seen for regular follow-up at 3 weeks, 2 months, and 6 months after surgery. At that time he complained of intermittent mild lateral thigh pain. Radiographs from the 6-month follow-up visit show interval healing of the right femoral shaft fracture with callus formation.
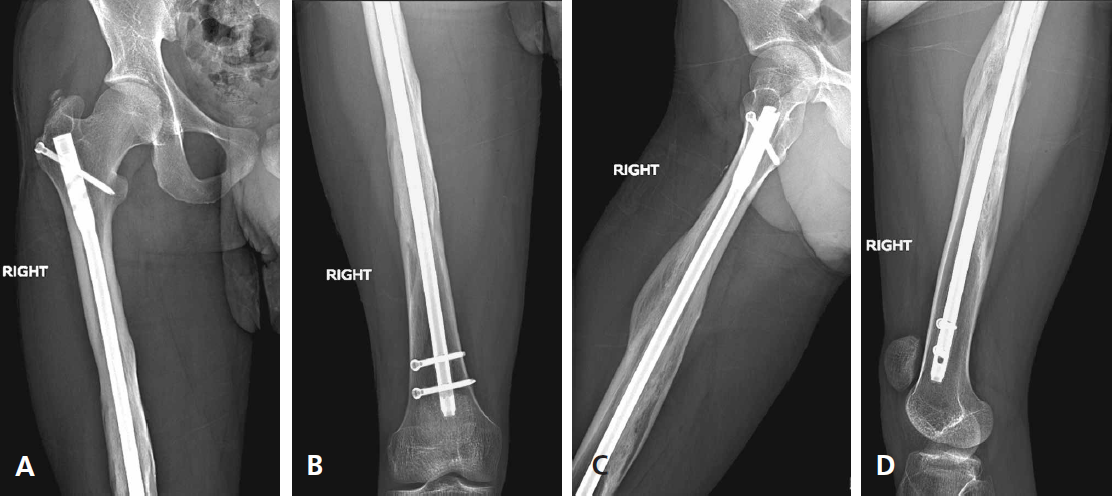
The patient was seen again for follow-up 3 years after surgery. At that time, he complained of an occasional sensation of knee buckling, although examination with Lachman, McMurrary, pivot shift, anterior drawer, and posterior drawer tests were not indicative of knee instability. Radiographs show a healed right femoral shaft fracture. He was prescribed physical therapy for quad strengthening and instructed to return to the clinic in 3 months.
Long-Term Follow-Up and Outcomes
There were no physeal fractures, growth disturbances, or angular deformities documented at the time of maximum follow-up. The mean length of follow-up in the pediatric orthopaedic clinic was 132 days or approximately 4.4 months (N = 18, range: 2 d to 2.95 y). Sixty-seven percent of patients were seen at least once in the pediatric orthopaedic clinic. Thirty-three percent of patients were never seen for followup in the pediatric orthopaedic surgery clinic after discharge from the index hospital admission; however, 56% of that subset of patients were seen for follow-up in the hospital’s trauma clinic. Of those patients not seen in the pediatric orthopaedic surgery clinic, 20% sustained fractures isolated to the upper extremity that were treated non-operatively, while 80% did not sustain a fracture.
The mean SF-36 Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were 48.7 (N = 3, range: 44.0 to 56.2) and 58.2 (N = 3, range: 51.3 to 62.2), respectively. The mean CTSQ score was 4.7 (N = 3, range: 4 to 5), (Table 3).
Patients with lower extremity GSWs complained of knee-buckling and stiffness subjectively, reporting mild to moderate difficulty with daily and recreational activities.
Discussion
As demonstrated by this study and others, firearm injuries cause significant morbidity to children and adolescents. Overall, demographics and clinical outcomes for this study population are comparable to those of previous studies. Previous studies on firearm injuries have consistently reported a predominance toward male victims. 4 , 6 - 8 , 14 - 16 This study had a mean time to follow-up of approximately 4.4 months, which is consistent with these investigators’ previous followup period for similar cohorts, which ranged from 3 to 6.6 months. 5 , 7 This limited follow-up may imply that patients in this cohort are transferring their care to other facilities or are not receiving appropriate follow-up. The rate of fractures secondary to extremity GSWs has been reported from 31% to 70% in prior studies, with this study’s findings falling at the higher end of the range. 5 - 7 , 16 - 18 The preponderance for GSWs to result in lower extremity fractures more often than upper extremity fractures is also consistent in the literature. 5 , 7 , 16 , 17 , 19 Other studies have identified the femur as the bone most frequently fractured, 16 , 17 , 19 and others have instead found the tibia 5 , 7 or hand bones 5 to be most common. The fibula was affected most commonly in this study population, followed by the tibia, and next the femur. There were no cases of infection in this study, compared to previously reported rates of infection from GSWs ranging from 3% to 19%. 16 , 17 Other investigators 6 , 7 have included prophylactic intravenous or parenteral broad spectrum antibiotics as a standard of care for their study populations.
Also of note, there were no cases of physeal arrest, growth disturbance, or angular deformity in the study population. The frequency of physeal injury secondary to extremity GSWs has been estimated to range from 0% to 28% and has been reported in the literature even when the bullet passes in close proximity to the physis but does not appear to violate it. 6 Letts and coworkers identified limb-length discrepancy (LLD) secondary to epiphyseal plate injuries as a major complication in their study population, occurring in 17% of children. 17 Stricker and colleagues diagnosed physeal injury in 4% of patients, which resulted in significant LLD, including a patient who required radial lengthening. 6 Bartotonicek published a case of avascular necrosis of the femoral head and resultant limb shortening secondary to a GSW in close proximity to the proximal femoral physis. 20 Naranje and associates reported on one patient with a femoral fracture secondary to a shot gun wound, which required multiple procedures for non-union and LLD. 7 Development of growth disturbance is also possible among those with extra-physeal fractures. Although all fractures in this study were extra-physeal, the lack of documented growth disturbance among this cohort may not be a generalizable finding but rather may reflect that the length of follow-up was insufficient to diagnose this particular complication of pediatric extremity GSW.
A finding unique to this study was that pediatric patients with extremity GSWs reported below average physical health and above average mental health relative to SF-36 age and gender-controlled national norms. 21 , 22 The psychological implications of ongoing disability and pain after orthopaedic trauma is important to consider, especially for postoperative rehabilitation and long-term function. 23 CTSQ scores were below the threshold for probable post-traumatic stress diagnosis in children and adolescents (PTSD). 24 This finding is likely not statistically significant because of poor follow-up and thus cannot be generalized to all pediatric GSW victims. To our knowledge, this study is the first to report the patients’ physical and mental health after extremity GSWs. Anecdotally, patients contacted for follow-up expressed relief in having the opportunity to see an orthopaedic surgeon for clinical evaluation.
There are several limitations to this study that must be taken into account when interpreting our results, including the limited sample size from a single-center and its retrospective design without a comparative or control group to perform statistical analysis. The conclusions derived from this research, especially from the functional outcome surveys, are limited by poor follow-up rates. This limitation is not unique to this study, as aforementioned, but rather a consistent challenge to our understanding of this orthopaedic issue nationally. For instance, a previous study on adult trauma clinic follow-up reported a follow-up rate of 57% at 4 weeks post-GSW, which was lower than all other injury mechanisms, such as blunt trauma, pedestrian struck, or motor vehicle collision, other than “not otherwise specified penetrating injury” at 9%. 25 This may also reflect a potential bias for our findings because patients with no long-term complications or functional deficits do not have a pressing need for care and are, therefore, less likely to be seen for follow-up. It is also possible that patients were brought by emergency medical services to the Level 1 trauma center at which this study was performed but then sought follow-up care at community hospitals.
Future public health efforts should be directed at maximizing outpatient follow-up after pediatric firearm injuries, which will in turn benefit future research on the long-term complications and functional deficits associated with extremity GSWs. The absence of documented growth disturbances or angular deformities in this study population may potentially be secondary to poor long-term follow-up. Outpatient follow-up for GSWs in the pediatric population is a concern because most complications, including deformity and limblength discrepancy, occur months to years after the injury. It is recommended that facilities treating these patients take a multidisciplinary approach and create a protocol to ensure long-term follow-up.
Footnotes
Conflict of Interest Statement
None of the authors have a financial or proprietary interest in the subject matter or materials discussed, including, but not limited to, employment, consultancies, stock ownership, honoraria, and paid expert testimony.