
Abstract
Remote telemetric monitoring of fetal haemodynamics in pregnant sheep would allow unrestricted animal movement, minimize suffering and distress, and improve animal welfare, while enhancing the quality of data collected. This may also be useful in clinical practice following fetal surgery. Using an open fetal surgical technique at approximately two-thirds of gestation, we implanted the catheter of a D70-PCTP haemodynamic telemetric device (Data Sciences International, Tilburg, The Netherlands) into the carotid artery of the fetal sheep (n = 4). The attached transmitter was secured to the posterior aspect of the maternal anterior abdominal wall. Two receivers, with a range of 1 m each, were sited in an 11 m2 sheep enclosure to maximize animal freedom while allowing continuous monitoring of the ewe. The receivers were connected by cable to a nearby computer. In the first two procedures, both fetuses died eight and 12 days after surgery, and the catheter tip was observed to be lying in the bicarotid trunk. In the next two procedures the catheter tip was threaded further upstream from the insertion point, in an attempt to reach the fetal aorta, and both fetuses survived until the scheduled postmortem examination at the end of pregnancy. After catheter implantation, fetal blood pressure (BP) and heart rate (HR) were successfully recorded continuously for seven days and then hourly per day for a further three weeks. The fetal BP and HR values were in the normal range for healthy sheep fetuses.
The chronically catheterized fetal sheep has been used extensively to study changes in fetal haemodynamics. 1 However, this type of experiment involves space restriction or animal restraint which has been shown to be a significant stressor. 2,3 Refinement of animal experiments to reduce the potential for suffering and stress and to improve animal welfare has been shown to improve the quality of data obtained. 4 It is also one of the cornerstones of the 3Rs, a widely accepted ethical framework for conducting scientific experiments using animals humanely. 4 We considered that telemetric monitoring of fetal blood pressure (BP) and heart rate (HR) in the freely moving pregnant ewe would meet these expectations. We thus report on our experience and technique using the D70-PCTP telemetric device (Data Sciences International, Tilburg, The Netherlands). This consists of a 49g (diameter 57 mm, thickness 8 mm) transmitter connected to two haemodynamic catheters (35 cm long, 1.2 mm outer diameter), one of which was used to measure the fetal arterial BP and the other to measure amniotic fluid pressure. An additional electrocardiogram (ECG) and temperature probe were available but were not used in these experiments. The device transmits data to two wireless receivers with a range of 1 m each. The receivers themselves are connected by cable to a computer where the data are stored.
This study was part of a larger experiment investigating the long-term effect of adenovirus vector-mediated local over-expression of vascular endothelial growth factor (VEGF) on uterine artery blood flow (UABF) in pregnant ewes. 5 All work was conducted in accordance with the Animals (Scientific Procedures) Act (1986) under aseptic conditions.
Four time-mated pregnant Romney ewes (weight range 54–74 kg) carrying singleton (n = 3) or twin fetal sheep (n = 1) were supplied by the Royal Veterinary College (Hertfordshire, UK) and delivered by van. The ewes were acclimatized for one week before initial intervention and housed in a group of two or three in an 11 m 2 pen (minimal required area = 1.9 m 2 per animal when housed in groups, Home Office, London, UK) with straw bedding that was replaced weekly and topped up daily. The covered open air pen provided natural temperature and humidity levels. The lighting was mainly natural through the open stable door but also by two fluorescent strip lights on a 12 hourly cycle (on 12:00–00:00 h). Air changes per hour and ammonia levels were unmonitored as the straw was being added daily. The diet consisted of natural grazing at tupping, then hay and concentrates (149-Super Ewe and Lamb; Lillico Attlee Ltd, Surrey, UK). Drinking water was untreated, unregulated and provided via an auto-replenishing volume controlled container.
The night before each surgery the pregnant ewes were kept fasted in a pair in a holding pen on woodchips. Initial laparotomy was performed at 101 days of gestation (term = 145 days) where general anaesthesia was induced with thiopental sodium 20 mg/kg intravenously (Thiovet; Novartis Animal Health UK Ltd, Hertfordshire, UK) and maintained with 2–2.5% isoflurane in oxygen (Isoflurane-Vet; Merial Animal Health Ltd, Essex, UK) after intubation. The gestational age was confirmed using ultrasound examination of fetal size according to standard measurements. The abdomen was sheared, cleaned with povidone iodine and draped. Laparotomy was performed using a midline incision below the umbilicus and the abdomen was opened in layers. A 6PS transit-time flow probe (Transonic Systems Inc, Ithaca, NY, USA) was then placed around each main uterine artery on both sides to investigate changes in UABF after adenovirus-VEGF vector injection. 5 The flow probe cables were then exteriorized on the upper right flank of the ewe. Following this the uterus was palpated and the fetal parts were identified. In an area of myometrium away from placentomes, a 5 cm uterine incision was placed just above the fetal head using a No. 21 blade. The fetal head was exteriorized through the uterine incision and the Babcock clamps were used to compress the amniotic membrane against the uterine wall in order to minimize bleeding. A 3 cm longitudinal incision was placed in the fetal neck 1 cm to the right of the trachea and the right common carotid artery was identified and mobilized from beneath the strap muscles. Two 3-0 silk ties (Mersilk; Ethicon Ltd, Edinburgh, UK) were passed under the vessel proximally and distally and held without tying using Kelly clamps. The right common carotid artery was then elevated under tension from the two sides to prevent excessive bleeding, while an incision was made in the vessel wall between using fine-tipped scissors until the lumen could be identified. A pair of fine-tipped curved forceps was inserted into the arterial lumen and the jaws were held apart to maintain luminal patency. One of the haemodynamic catheters of the telemetric D70-PCTP device was inserted into the arterial lumen and threaded upstream towards the aorta for a distance of around 5–7 cm until a clear signal to the nearby receiver could be obtained. The silk lines were then tied, one to occlude the vessel distally and another to secure the catheter within the vessel proximally. The neck skin was closed over the catheter using 2-0 Vicryl (Ethicon, St Stevens-Woluwe, Belgium) and a few coils of the catheter were secured to the fetal skin to prevent accidental stretching of the catheter. The fetal head was returned to the amniotic cavity. The other haemodynamic catheter was inserted into the amniotic cavity to record background pressure. The uterine incision was closed in two layers using 2-0 PDS (Ethicon, St Stevens-Woluwe, Belgium) in a running fashion with the catheters passing through the incision at a distance from the angles. While the first layer incorporated the whole thickness of the uterine wall along with the amniotic membrane, the second layer buried the first to provide a water-tight seal. The transmitter was then attached to the inner surface of the abdominal wall slightly lateral to the laparotomy incision using 3-0 Prolene (Ethicon, Norderstedt, Germany). This step is necessary to allow easy accessibility since an external magnet is needed to turn the transmitter on and off. A 3 mL intramuscular injection of Penstrep (200 mg/mL procaine penicillin and 250 mg/mL dihydrostreptomycin; Norbrook Laboratories Ltd, County Down, UK) and a 75% intraperitoneal/25% intrauterine injection of sodium benzylpenicillin G 3 g (Crystapen; Schering-Plough, Uxbridge, UK) + gentamicin 80 mg (Genticin Injectable; Roche Products Ltd, Hertfordshire, UK) were given at the end of the procedure for infection prophylaxis. The abdomen was then closed in layers and buprenorphine 0.01 mg/kg intramuscularly (Vetergesic; Alstoe Animal Health, York, UK) was administered every 6–12 h for analgesia during the first 48–72 h after the operation and the ewe was allowed to recover. Seven days later, the ewes underwent a second general anaesthetic and laparotomy for local administration of the adenovirus-VEGF vector (Ark Therapeutics Plc, Kuopio, Finland) into the uterine artery. The uterine incision was observed at this time but the uterus was not opened.
In the first procedure, the catheter was placed into the common carotid artery. Fetal BP and HR data were collected and appeared to be in the normal range for the first 11 days after catheter placement. Adenovirus vector injection was performed uneventfully seven days after catheter placement. On the 12th day after catheter placement, there was a sudden drop in BP and HR followed by fetal death. Postmortem examination performed 48 h later showed no fetal abnormality, haemorrhage or structural damage, and culture of tissues from the uterus and fetus revealed no evidence of microbial invasion. The tip of the catheter was found lying in the bicarotid trunk where it may have caused a partial obstruction of blood flow to both common carotid arteries. As there is some evidence that cannulation of the fetal sheep carotid arteries can result in ischaemic brain damage especially when bilateral obstruction has occurred, 6 we attempted to cannulate the second fetus through the femoral artery as an alternative route. On examining the fetal femoral artery at hysterotomy, this proved impossible to achieve at this gestational age due to the discrepancy between the small diameter of the femoral artery when compared with the catheter tip. The second fetus was thus cannulated through the common carotid artery as before. Fetal death again occurred suddenly, on the eighth day after catheter placement, and one day after vector injection. The catheter tip was observed at the bicarotid trunk in a similar way to the preceding fetus. There were no abnormal findings at postmortem examination.
In the subsequent two procedures we adjusted our technique to thread the catheter tip further upstream in the carotid artery in an attempt to bypass the bicarotid trunk and reach the descending aorta. We used the distance between the point of insertion and the middle third of the sternum as an estimate of the threading distance which was approximately 7 cm in both fetuses. The cannulation of the common carotid artery in these two fetuses was uncomplicated, and both survived until the end of gestation. At scheduled postmortem examination in one fetus (138 days of gestation), the catheter tip was found to be lying in the right common carotid artery just below the point of insertion. This downstream migration of the catheter tip might have been a result of fetal growth and movement. We were not able to ascertain the position of the catheter tip in the other fetus, which was unexpectedly born overnight two days before scheduled postmortem at term (139 days of gestation). During birth the catheter was pulled out from the carotid artery without obvious haemorrhage or structural damage to the fetal neck. This lamb survived until planned postmortem examination at four months of age.
The D70-PCTP implanted devices can transmit in a range slightly exceeding 1 m and we arranged our two receivers in a way to maximize free animal movement while maintaining a good signal. The monitoring room set-up is graphically illustrated in Figure 1. Fetal BP and HR data were transmitted telemetrically to the receivers that were in turn connected by cable to a computer in the adjacent room. Uploaded traces were viewed using the Dataquest software (Data Sciences International), then selected traces were copied onto a database (Microsoft Office Excel 2007 software; Microsoft Corporation, Redmond, WA, USA) for further analysis. The difference between the fetal arterial and amniotic fluid pressure was used to calculate the true fetal BP. Data were collected continuously for three days before and seven days after vector injection and then for one hour a day until the end of gestation.
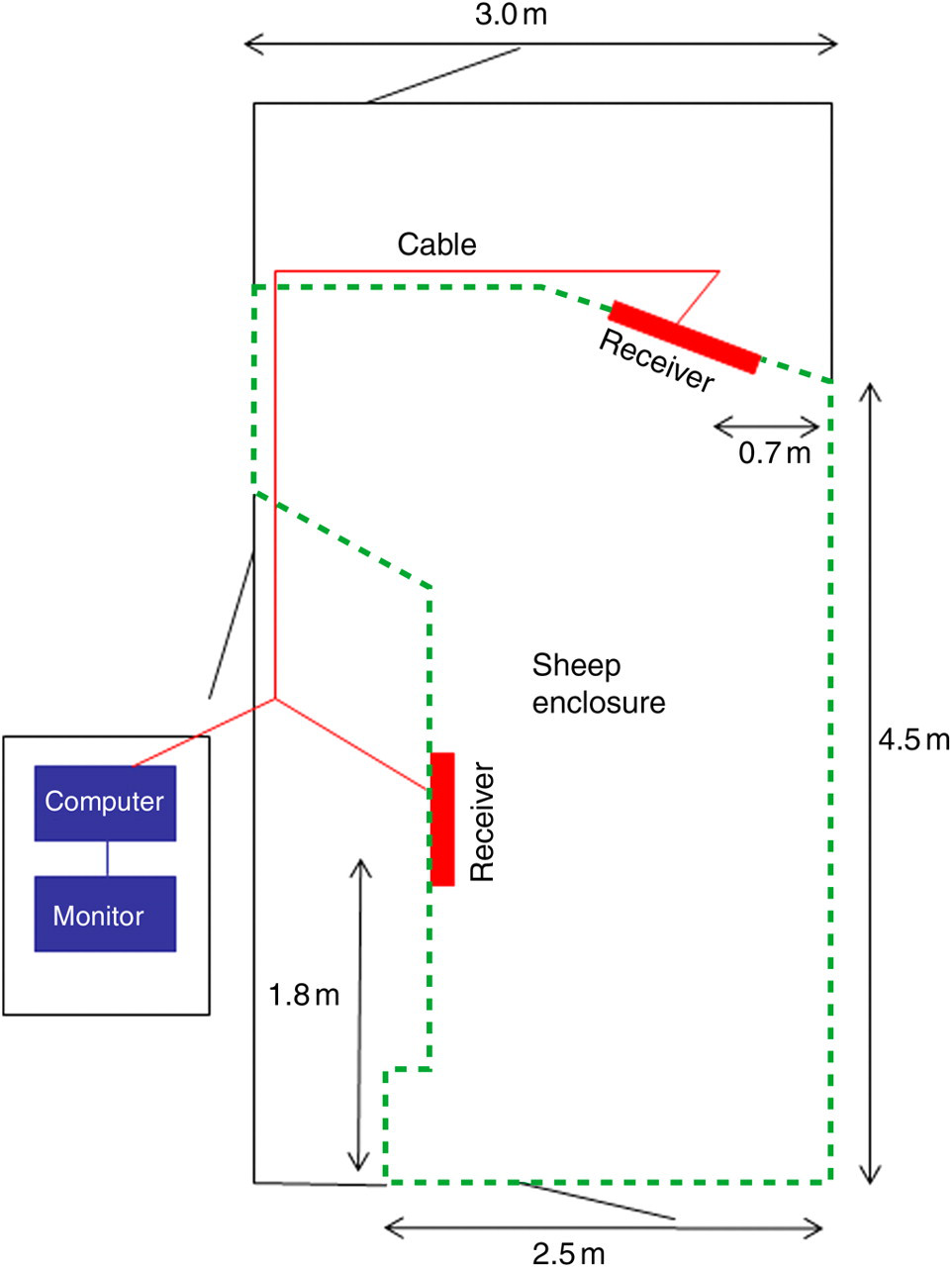
The monitoring space consisted of an animal enclosure room adjacent to a computer room. The two receivers, which were fixed at 53 cm above ground level on the inside of the enclosure, were arranged in a way to maximize free animal movement in the space available while maintaining a good signal. The dashed line indicates the area of the enclosure in which the sheep were free to roam. Cables ran from each receiver to the computer outside the sheep enclosure and above the height of the ewe to avoid damage
In all four ewes, fetal BP and HR recordings were successfully obtained in a continuous fashion as well as for one hour a day by turning the transmitter on and off in the ewe to be monitored. Short intermittent periods of signal loss were initially noticed when the ewe strayed away from the receivers. After repositioning of the receivers, this was kept to a minimum (Figure 1). Using this set-up, the signal could be detected by one of the two receivers at any one time, providing data for hourly monitoring in 100% of the diurnal and daily monitoring periods. Figures 2a and b show the fetal BP and HR during gestation as recorded daily over one hour in the morning. The fetal BP and HR values obtained using this method agree with the normal gestational-age dependant values published previously. 7–9
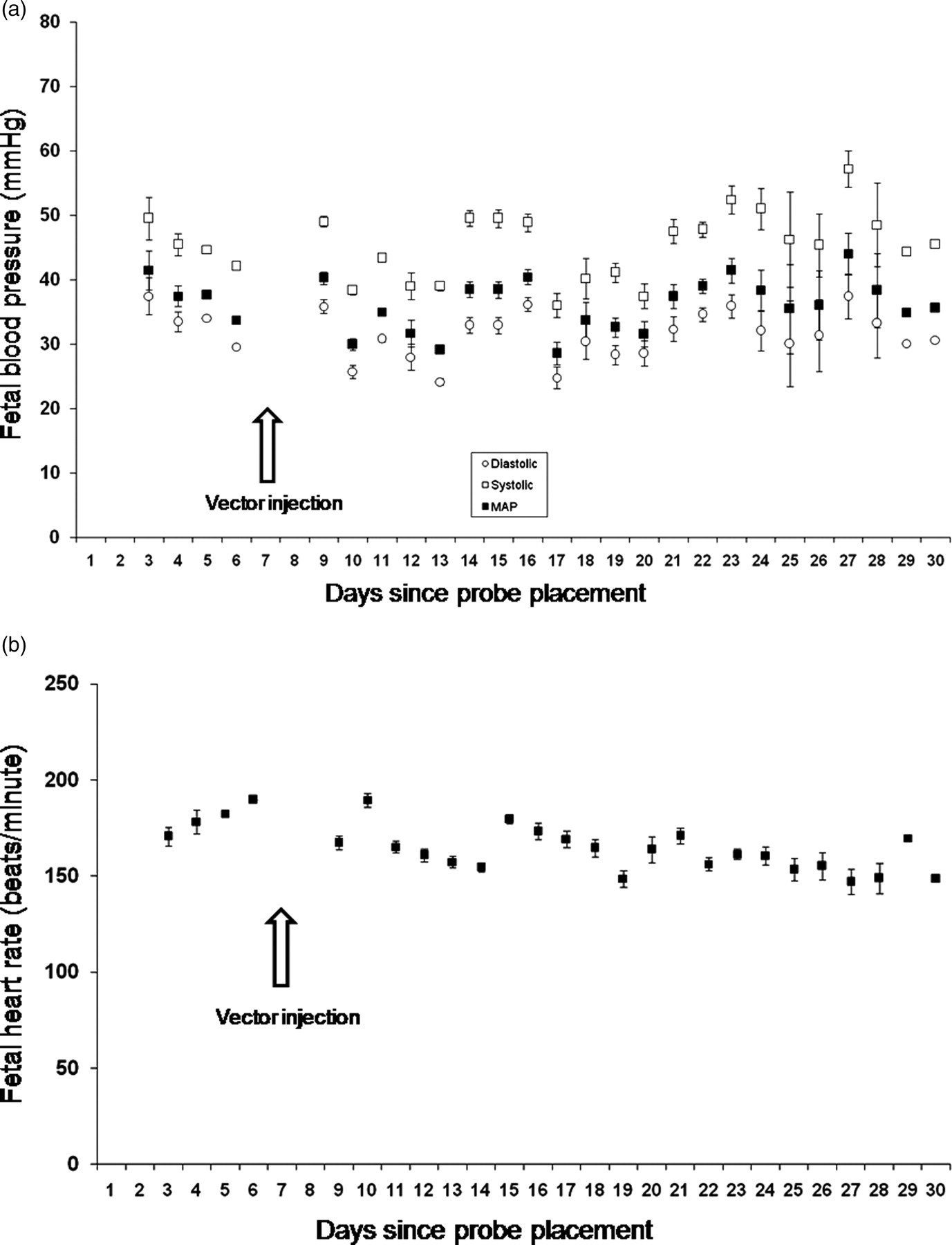
Results of telemetric fetal (a) blood pressure and (b) heart rate measurement as monitored daily for four weeks after device insertion into the carotid arteries of one sheep fetus. Measurements are shown as the mean ± SEM. MAP: mean arterial pressure
It would have been feasible to attach the ECG probe of the D70-PCTP device to the fetal sheep for ECG monitoring. This can be accomplished by subcutaneous implantation of the ECG leads over the fetal chest. We decided not to attach the ECG probe as it was unnecessary for our experimental protocol and would have involved an additional fetal invasive procedure. A report describing the telemetric acquisition of fetal ECG traces in the sheep has been published. 10 In this study, a miniature ECG device with a signal transmission range of 20 cm was implanted subcutaneously in the fetus. Because of the limited range, the receiver was taped to the maternal abdomen externally along with a custom-made amplifier/transmitter in order to transmit the signal over 5 m to an adjacent computer base. 10 We present a more simple method using commercially available implantable hardware. In addition, hardware taped to the external surface of the ewe may be easily damaged compromising the length of time during which data could be obtained. An advantage of the more traditional method of chronic fetal catheterization using implanted externalized catheters is that it permits access to the fetal circulation and amniotic cavity for fluid sampling over time, and this is not feasible using the telemetric monitoring method described here.
As a conclusion, we have shown that chronic monitoring of fetal BP, HR and most probably ECG is feasible using an implantable telemetric device in the freely moving pregnant ewe. This is in line with published recommendations to limit animal stress, improve animal welfare and satisfy its physiological and ethological needs as far as practicable when performing necessary animal experimentation. While intra-arterial haemodynamic monitoring of the fetus is too invasive to justify for human application, telemetric electrocardiographic fetal monitoring may be useful in clinical practice following open fetal surgery to monitor fetal wellbeing long term. 11,12
Footnotes
Acknowledgements
The authors wish to thank David Manners from the Royal Veterinary College at Hawkshead for his help in providing the pregnant ewes.
All the authors revised the manuscript critically for important intellectual content and approved the final version.
Project Licence PPL 70/6546, Home Office, UK, January 2007.