
Abstract
Thyroglossal duct cysts (TGDCs) are congenital midline neck lesions commonly diagnosed in pediatric patients but are relatively rare in adults. They are often discovered incidentally during thyroid imaging. An example case is provided of a female patient in the third decade of her life, referred for routine thyroid sonographic follow-up, in whom a midline TGDC slightly deviated to the right, was identified. Notably, imaging conducted less than a year prior showed no evidence of the cyst. This raises the possibility that the lesion was either previously missed or has enlarged since the prior study. This patient case signifies the importance of considering TGDCs in adult patients and underscores the role of thorough sonographic evaluation in their detection.
Thyroglossal duct cysts (TGDCs) are among the most common nonodontogenic congenital neck cysts in children but are relatively rare in adults.1,2 Some authors have reported the incidence of TGDCs in children to be approximately 75% while the estimated prevalence of TGDCs in adult population is 7%.3,4
Embryologically, the thyroglossal duct guides the migration of the thyroid gland from the foramen cecum at the tongue base to its definitive position inferior to the hyoid bone at the level of thyroid cartilage by the end of the first trimester.1,5,6 In some cases, the duct fails to involute and persists postnatally, potentially manifesting as a pyramidal lobe of the thyroid or a TGDC along its original path. 1 TGDCs are typically midline, but lateral deviations have been documented, particularly in adults. 2 Approximately 65% are located inferior to the hyoid bone. 1 The cyst’s epithelium can secrete fluid, leading to enlargement, especially in the presence of infection or inflammation. 7
Diagnostic sonography is commonly used to evaluate superficial neck masses in pediatric and adult populations. These masses may include thyroglossal duct cysts (TGDCs), epidermoid and dermoid cysts, branchial cleft cysts, lymphadenopathy, and thyroid or parathyroid abnormalities. 8 In cases where sonographic findings are equivocal or nondiagnostic, cross-sectional imaging techniques such as computed tomography (CT) or magnetic resonance imaging (MRI) are recommended.1,8 The example patient case presents an incidental TGDC identified on a routine thyroid sonogram.
Case Report
A woman in her third decade of life was referred to the imaging department for routine sonographic follow-up examination, based on a previously identified thyroid nodule. Her medical history included a left submandibular gland neoplasm first identified with sonography in 2021, following a referral for localized pain. A 2.7-cm hypoechoic solid mass was detected and later confirmed by CT. The lesion was surgically excised without documented fine-needle aspiration (FNA), although FNA would typically precede excision. An incidental TIRADS-4 thyroid nodule was also noted during the initial sonographic examination. Subsequent follow-up sonograms confirmed the nodule’s stability. The most recent examination, prior to the current exam, was performed less than a year ago. The patient reported no current symptoms related to the neck in the interim. On objective assessment, the sonographer did not visualize or palpated any lump in the neck, especially in the midline.
In this study, performed using a LOGIQ E10 system (GE HealthCare, Wauwatosa, WI, USA) with a linear ML4-20 transducer (4–20 MHz), the thyroid gland appeared unchanged. However, a well-circumscribed cystic lesion measuring 2.3 cm was identified, at the level of the hyoid bone. As the trace measurement tool was not available, in the thyroid exam setting, the sonographer manually recorded three dimensions to capture the full extent of the lesion (See Figure 1). In addition, this cystic structure did not demonstrate any flow on color Doppler (See Figure 2). The lesion demonstrated dynamic movement and superior displacement with tongue protrusion and retraction, consistent with a TGDC (refer to QR code for video).
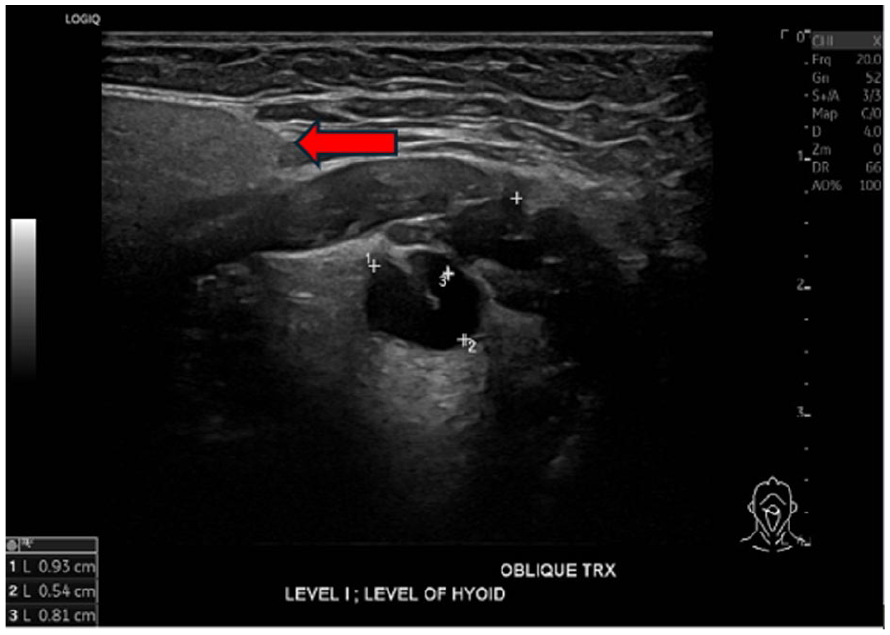
An oblique transverse sonogram is provided that demonstrates a well-defined cystic lesion located just to the right of the midline at the level of the hyoid bone. The right submandibular gland is also visible in the field of view (see red arrows).
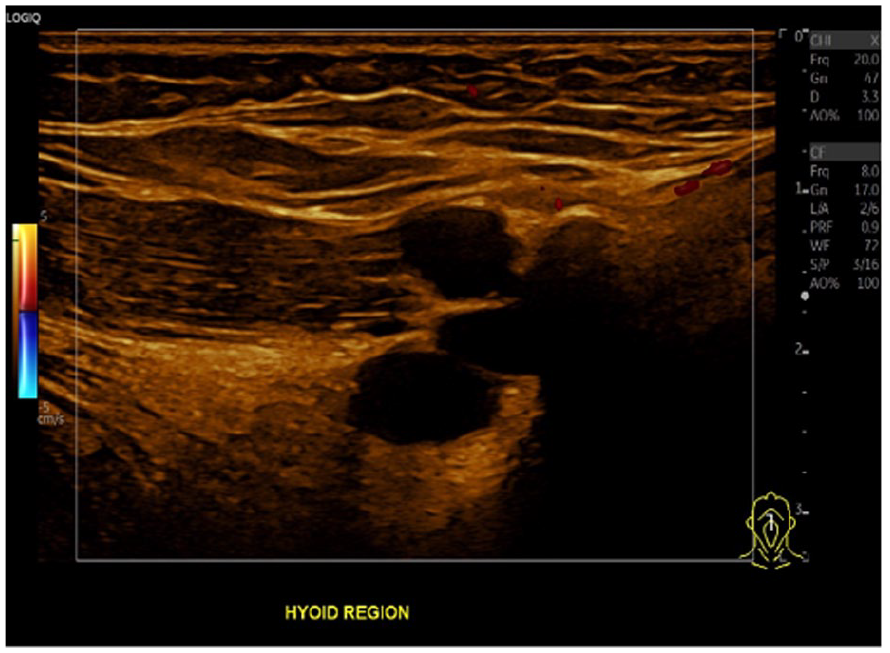
A sagittal sonographic view demonstrates the cystic lesion, with no internal blood flow detected with color Doppler.
A preliminary diagnosis of TGDC was made based on the sonographic findings. A retrospective review of four previous sonographic examinations, revealed no evidence of this cystic structure detected on a review of images archived within the picture archiving and communication system (PACS) or within the associated radiology reports. In addition, an initially performed contrast-enhanced neck CT was reviewed for comparison, and no cystic lesion was identified, at the level of the hyoid bone (See Figure 3).
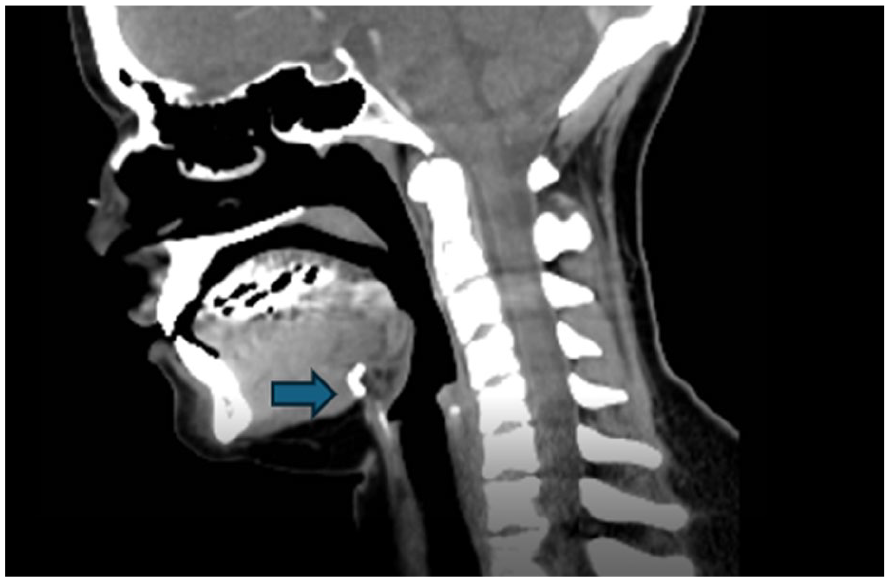
A sagittal image plane is provided of a contrast-enhanced neck computed tomogram (CT). This image shows no definitive evidence of a thyroglossal duct cyst (TGDC), at the level of the hyoid bone (see blue arrows).
Discussion
Thyroglossal duct cysts are occasionally identified during a routine thyroid sonography in adults, though they are more commonly encountered in pediatric patients. Branchial cleft cysts, epidermal inclusion cysts, dermoid cysts, laryngocele, thymic cyst, necrotic metastases and lymphatic malformations are some of the differential diagnoses to consider when evaluating TGDC, with sonography.1,9 On a sonogram, any cystic structure, in close proximity to the hyoid bone, is a vital clue to the potential diagnosis of TGDC. 1 In the current case, a TGDC was incidentally discovered during follow-up imaging of a TIRADS-4 thyroid nodule.
Thyroglossal duct cysts are formed because of failure of the involution of thyroglossal duct, after the thyroid gland descends from the foramen cecum of the tongue to its final location in the inferior neck, around the late first trimester.1,10 TGDC appear as a painless mobile mass that tends to move with tongue protrusion. 11 Sonographically, TGDC do not always manifest as unilocular, thin walled anechoic cysts. Sometimes TGDC can become infected and inflamed and might display complex echoes within. 12
Thyroglossal duct cysts are evaluated using sonography, MRI, or CT. On MRI, they appear hyperintense on T2-weighted images and show variable signal intensity on T1-weighted images depending on protein content. 6 CT typically reveals a smooth, thin-walled, fluid-density lesion near the hyoid bone. 6 Sonography remains the preferred initial imaging choice due to its safety, portability, and dynamic imaging capability.6,13 In the current patient, TGDC was not visible on objective assessment, hence imaging appears to be the only method for diagnosing smaller asymptomatic TGDCs.
The diagnosis of TGDC is based on its characteristic location near the hyoid bone and its dynamic movement with tongue protrusion, which is considered pathognomonic for TGDC on sonography. 14 A review of four prior sonographic studies revealed no evidence of cystic lesions with imaging or noted in the radiology reports. Further complicating the diagnosis, a contrast-enhanced neck CT from 2021 did not demonstrate any cystic structure at the hyoid level (See Figure 3). It is suspected that the hyoid region was not thoroughly examined during the earlier sonograms, potentially leading to a missed detection. Alternatively, it is speculated that the TGDC may have developed or enlarged in the interval, specifically after the sonogram performed in 2024.
Thyroglossal duct cysts may enlarge due to infection or inflammation of the epithelial-lined duct. 1 However, the patient had no history of TGDC surgery (e.g., Sistrunk procedure), no recent upper respiratory infection, and no local symptoms such as odynophagia. This case is notable for the apparent de novo or progressive development of a TGDC, in an asymptomatic adult, without precipitating factors. The standard treatment for symptomatic or complicated TGDCs is the Sistrunk procedure, which involves removal of the cyst, central hyoid bone, and adjacent tongue base tissue.15,16
Although TGDCs are usually benign, there is a small risk of malignant transformation. The reported incidence ranges from 0.7% to 1.5%. 17 Papillary and squamous cell carcinoma are two of the malignancies reported in TGDC, with an incidence of 94% and 5%, respectively. 18 Squamous cell carcinoma of the TGDC has a very dismal prognosis with a mortality rate between 30% and 40%. 18 Thus, it is crucial to report any evidence of TGDC on any radiologic examination, to create a baseline for imaging the patient. Fine needle aspiration (FNA) assists in definitively diagnosing the TGDC carcinoma in suspicious cases. 17 Given the malignant potential, some authors advocate for surgical excision even in asymptomatic adult patients.2,6,19
Conclusion
This patient case emphasized the diagnostic value of sonography in identifying incidental TGDCs, even when previous imaging appears unremarkable. Any cystic structure in the vicinity of the hyoid bone should entail the sonographer to evaluate this cystic mass scrupulously in addition to using dynamic sonographic maneuvers to diagnose this as TGDC. Detection of an asymptomatic TGDC should prompt clinical follow-up and potential specialist referral to determine the need for surgical intervention. Effective interdisciplinary collaboration between imaging professionals and surgical specialists is crucial to ensuring optimal patient care.
Supplemental Material
sj-pdf-1-jdm-10.1177_87564793251362211 – Supplemental material for An Incidental Thyroglossal Duct Cyst in an Adult Female: A Case Report
Supplemental material, sj-pdf-1-jdm-10.1177_87564793251362211 for An Incidental Thyroglossal Duct Cyst in an Adult Female: A Case Report by Gurinder Dhanju, Ashraf Goubran, Iain Kirkpatrick and Vivake Umadat in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from University of Manitoba REB# HS26986 (H2025:190).
Informed Consent
Written informed consent was obtained from the subjects before the release of the report for review.
Peer Reviewer Guarantee Statement
A member of the JDMS Editorial Board is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editorial Board member had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.