
Abstract
Thyroglossal duct cysts account for most diagnosed midline neck masses. They generally sit at or below the hyoid bone. They can vary in appearance and area of infiltration, although few cases of laryngeal involvement have been reported. Sonography is the modality of choice for imaging these cysts, followed by a Sistrunk procedure to remove the cyst. This case report focuses on the sonographic appearance of these cysts and their management.
Thyroglossal duct cysts (TDCs) are the most common congenital abnormality of the neck. They account for 75% of congenital midline neck masses. 1 Two-thirds of thyroglossal duct anomalies are diagnosed within the first three decades of life, with more than half being identified before 10 years of age. 2 Sonography remains the primary imaging modality used to evaluate these masses, although the use of computed tomography (CT) and magnetic resonance imaging (MRI) also has been well documented. 3 It is uncommon for TDCs to cause laryngeal invasion, and few cases have been reported about the effect of thyroglossal duct cysts on the vocal cords. Dysphagia, respiratory distress, or influence on the voice is extremely rare. 4 The following case report demonstrates the sonographic characteristics of these cysts and shows the potential for affecting the vocal cords.
Case Report
A 30-year-old woman presented to otolaryngology after discovering a palpable midline neck mass. She stated that it had been enlarging over the past four months. Upon physical examination, a soft compressible mass at the level of the hyoid bone was observed. She noted a mild globus sensation described as fullness when swallowing and a change in voice while singing. Thyroid laboratory values were all within normal limits. A fiber-optic laryngoscopy was performed to examine the patient’s throat and larynx, with normal results.
Sonography was ordered to further evaluate the palpable mass. A sonogram of the neck was done using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington) with a 12-MHz linear array and an 8-MHz curved linear transducer. Ample gel was used as a standoff pad to image the superficial palpable area of fullness. A midline cyst was observed with a lobulated component that extended posteriorly toward the vocal cords. The cyst was anechoic with echogenic floating debris (Figure 1) and was located anterior to the hyoid bone (Figure 2). The borders of the cyst were distinct anteriorly but became vague along the posterior aspect (Figure 3). The cyst measured 2.8 × 2 × 1.9 cm. No internal flow was observed with color Doppler imaging or by spectral Doppler (Figure 4). Due to the characteristics and location of this mass, it was diagnosed as a thyroglossal duct cyst.

Transverse gray-scale image of the midline neck cyst, showing echogenic floating debris.
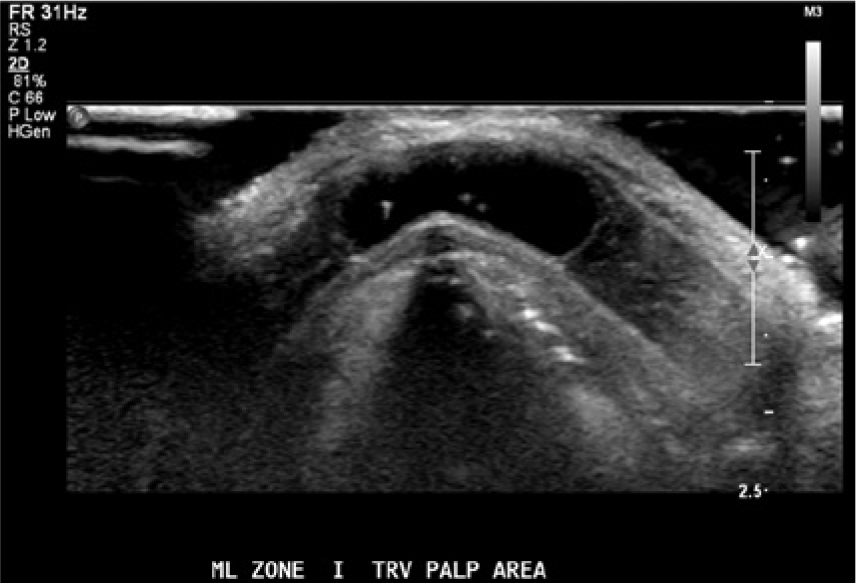
Transverse gray-scale image of the neck cyst anterior to the hyoid bone.

Sagittal gray-scale image of the neck cyst showing prominent anterior borders and more vague posterior borders.
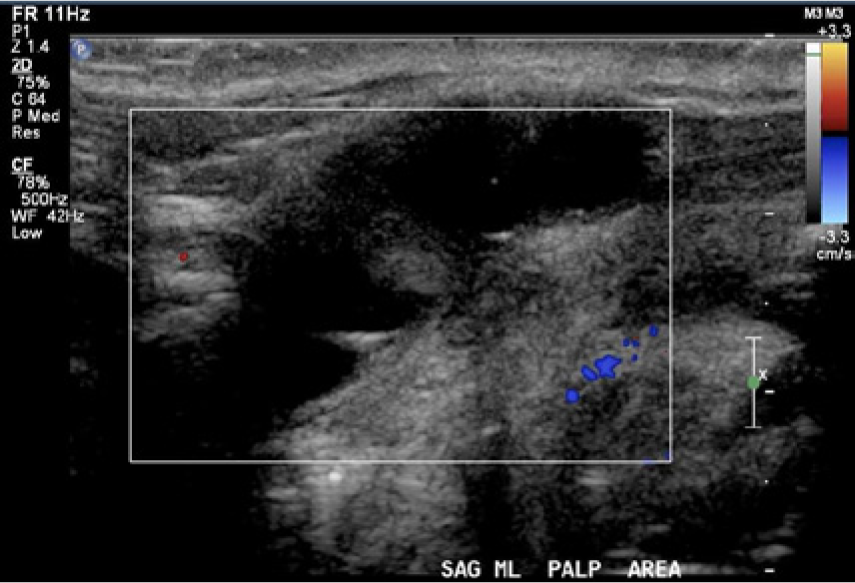
Color Doppler imaging of the cyst showed no internal flow within the lesion.
The otolaryngologist recommended a Sistrunk procedure for TDC removal, a surgical procedure that involves the removal of the cyst as well as resection of the thyroglossal duct up to the base of the tongue and the medial segment of the hyoid bone if involved. 5 The patient was admitted and the mass was dissected circumferentially. No communication with the thyroid was observed. However, the mass was continuous with the midline aspect of the hyoid bone, and therefore the hyoid bone was removed along with the mass as is commonly done for this procedure. There was no communication with the base of the tongue, nor was there any evidence of laryngeal involvement. Pathologic evaluation revealed a respiratory epithelial cyst with adjacent partially atrophic thyroid follicles, consistent with those of a thyroglossal duct cyst.
Discussion
Between the fourth and seventh weeks of development, the thyroid gland descends from the foramen caecum at the base of the tongue to its final position anterior and lateral to the trachea. 6 The thyroid remains connected to the tongue by the thyroglossal duct. This duct normally involutes by the tenth week of development. The thyroglossal tract passes through the muscles of the tongue and then anterior to the hyoid bone and larynx and is intimately positioned to the hyoid bone. 6
Abnormal involution of the thyroglossal duct accounts for most midline cysts and fistulae of the neck; thyroglossal duct cysts are thought to represent a failure of only a segment of the thyroglossal duct to involute.7,8 They can develop anywhere along the course of the thyroglossal duct remnant, which extends from the base of the tongue to the suprasternal region. 3 Thyroglossal duct cysts are located at the level of the hyoid bone (15%) or immediately below it (65%). 9 Thyroglossal duct cyst is the most common anomaly found in the midline cervical region in children.7,10 They occur with approximately equal frequency in boys and girls, and most of these cysts are detected in the first decade of life.2,11
The sonographic appearance of a thyroglossal duct cyst typically is a round or oval anechoic cyst that is well circumscribed, with posterior acoustic enhancement. 9 These cysts can be multilocular or have a pseudosolid appearance. Clinically, they typically present as a gradually enlarging, painless midline neck mass that usually occurs in children and young adults. They are found midline in about 75% of cases and slightly off midline in 25%. 9 When symptomatic, TDCs are removed surgically using the Sistrunk procedure described below. However, in some cases, the TDC can remain asymptomatic. 12
The differential diagnosis of a TDC includes dermoid cysts, branchial cleft cysts, lymphadenopathy, or cystic nodules arising from the thyroid gland. 3 Dermoid cysts are usually complex with both cystic and solid components. Branchial cleft cysts appear anechoic with posterior enhancement. They are located lateral to midline. Because the appearance of this cyst is relatively similar to a TDC, the location of the branchial cleft cyst plays an important role in differentiating these two entities. Lymphadenopathy presents as a well-defined circular or oval lymph node with or without an echogenic hilum. Although the appearances of TDCs can vary, the midline location is the most important variable in distinguishing between these entities.
Sonography is typically the initial modality for evaluating anomalies of the neck. 13 Sonography is widely available and of relatively low cost; in addition, it does not use ionizing radiation or require intravenous contrast material or sedation, important considerations especially in the pediatric age group, when most of the thyroglossal duct cysts are found and treated. In cases of large lesions or suspected malignancy, CT or MRI may be required for diagnosis and follow-up.
Thyroglossal duct cysts are removed with a Sistrunk procedure.2,5 This procedure consists of removing the mass and surrounding structures to limit reoccurrence. With the patient in a supine position, a transverse incision is made over the mass, and dissection is carried down to the cyst. Dissection is then made toward the hyoid bone. The central hyoid bone is removed, along with tissue from the muscle, at the base of the tongue to the foramen cecum. The cyst is dissected and the associated tract is excised. With complete excision, the rate of recurrence is less than 5%, although with lesser procedures, a significantly higher recurrence rate has been reported.14,15 There currently are no viable alternatives to the Sistrunk procedure; however, if an infection occurs in conjunction with a TDC, the patient may have the cyst drained and receive antibiotics prior to the surgery.
After surgery, the specimen is sent to pathology to determine its characteristics. In less than 1% of cases, TDCs are malignant.9,16 Few cases have been reported showing laryngeal invasion of the TDC. Most cases of TDC are diagnosed when the cysts become inflamed and enlarged, but they can also be hidden and present with respiratory and vocal symptoms. Unusually located cysts have been reported in the thyroid, larynx, hyoid bone, lateral neck, and the tongue. 17
Conclusion
Sonography is an important modality to provide a thorough evaluation of neck masses. Diagnosis of a neck mass such as a thyroglossal duct cyst is relatively easily made based on its location and sonographic characteristics. Although the thyroglossal duct cyst in this case was not noted to have laryngeal invasion, its effect on the patient’s vocal cords was unusual.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.