
Abstract
An accurate evaluation of thyroid volume, in patients of all ages, is important for the correct diagnosis of a goiter and for sonographic monitoring of thyroid diseases. It is especially important in pediatrics because the linear measurements of a developing thyroid gland do not correlate well with age, sex, or body composition variables. Diverse methods are used to estimate thyroid size and volume. Sonographic volumetry and visual inspection and palpation are used to evaluate the thyroid. Although thyroid size can be easily assessed on physical examination, due to the superficial location of the gland, palpation has low sensitivity and specificity for the management and diagnosis of thyroid disorders. Therefore, thyroid volume measured sonographically is more accurate than thyroid size assessed with a physical examination. Imprecise calculation of thyroid size and volume may lead to false-positive or false-negative diagnoses of thyromegaly, which may result in unnecessary or delayed care.
Keywords
Besides the incidence of benign and malignant thyroid nodules, up to 14.7% of Americans have various thyroid disorders, of which subclinical hypothyroidism is the most common. 1 Thyroid nodules are found in up to 50% of the general population. 1 There is a noticeable sexual dimorphism of thyroid diseases, with females being 5 to 10 times more likely than males to have thyroid problems. 1
Numerous factors affect the size of the thyroid gland. Factors such as age, sex, weight, height, body mass index, and body surface area have been positively correlated with thyroid volume. Diets lacking sufficient iodine and even cigarette smoking have also been shown to affect thyroid volume. 2 An enlargement of the thyroid gland is called a goiter. Goiter is also known as struma and thyromegaly. The most common cause of endemic goiter worldwide is iodine deficiency. 3 However, in iodine-replete countries, such as the United States, thyromegaly usually develops as a result of autoimmune thyroid disorders, the most common being Hashimoto thyroiditis, Graves disease, and thyroid nodules. 3 Other associated causes of a goiter are intrinsic thyroid hormone production defects, as well as various medications such as aminosalicylic acid, lithium, and even excessively large doses of iodine.4,5
Physical examination by a family doctor, pediatrician, or endocrinologist is usually the first step in uncovering thyroid diseases. Experienced clinicians can determine an enlarged thyroid by palpation. However, in approximately one-third of cases, the sonographic measurement of thyroid volume differs from the estimated size on a physical examination. 6 The clinical relevance of establishing accurate thyroid volume becomes invaluable for surgical planning, calculating the dose of iodine 131 needed for thyrotoxicosis treatments, and monitoring of effectiveness of various thyroid therapies. 7
No current guidelines in the United States require measurements of a thyroid volume as part of sonographic examination of the gland, which precludes an accurate and reproducible diagnosis of thyromegaly. The American College of Radiology (ACR), as well as other radiologic organizations, recommends obtaining the three linear thyroid measurements: anteroposterior (AP), transverse (TR), and longitudinal (L) of each lobe, plus the AP measurement of the isthmus, without establishing an upper limit for a normal thyroid size in various age groups. 8 As a result, there is a concern that some US radiologists may not be documenting whether the gland is enlarged.
From a technical point of view, thyroid volume can easily be recorded for each patient, given that modern sonographic equipment calculates volume automatically, when three linear measurements are obtained per lobe. This makes the documentation of total thyroid volume feasible for a thyroid sonogram and should improve the diagnostic value. Such a volumetric approach has been accepted outside of the United States for years.9–13
Historical Review
The largest of all endocrine glands, the thyroid produces hormones that are vital for growth, development, and metabolism. The Belgian anatomist Vesalius made one of the first scientific descriptions and drawings of the thyroid, as a discrete organ, in his thesis “De humani corporis fabrica libri septem” (“The Seven Books on the Structure of the Human Body”), published in 1543. 14 In 1656, the English anatomist Wharton named the gland thyroid because it was shaped like a shield (thureos or thyreos in Greek). 14 Interestingly, Wharton thought that there were two thyroid glands, assuming that the right and left lobes represented individual organs. He even recorded the weight of a 28-year-old man’s individual thyroid lobe as 29.2 g (7.5 drachms in the original publication). 14 Recognizing the correlation between an enlarged thyroid and thyrotoxicosis, a thyroidectomy was successfully performed in 1884, as treatment for a toxic goiter. 15 In the early 20th century, the thyroid’s secretion of an iodine-containing substance was discovered. In 1914, Edward Kendall isolated the first thyroid hormone, crystalline thyroxine (T4), at the Mayo Clinic in Rochester, Minnesota. 15
In 1960, the World Health Organization (WHO) defined a goiter as a condition in which the thyroid lobes exceed the volume of the terminal phalanges of the thumbs of an examined individual. 16 Endemic goiter is a worldwide problem, which seriously affects the growth and development of children, as well as leading to numerous adult thyroid disorders. 16 Currently, there are still recorded cases of endemic goiter in the United States, after decades introducing a universal iodization program. 17
There is physical anthropological evidence of goiters occurring 2000 years ago in North America, likely due to an iodine deficiency. 18 The affected regions of the continent were called the “goiter belt.” It included the Pacific Northwest, the North-Central States, Great Lake District, and the Appalachian Highlands. 18 Among the main reasons for iodine insufficiency, in these areas, were iodine-depleted soil and water related to the advance of Ice Age glaciers thousands of years ago and yearly heavy rains. 19 Other factors that increased the frequency of a goiter in the American population included tobacco smoking and a diet lacking in seafood. 19
Since the United States implemented a universal iodization program during the 1920s, the incidence of thyromegaly has dropped significantly. Nevertheless, an endemic goiter still occurs in the United States and may be due to a trend of decreased salt consumption, including iodized salt, as well as an increased awareness of hypertension and coronary artery disease. 17
Physicians used physical examination to assess the thyroid for many years. In 1962, Fujimoto began performing thyroid sonograms in Tokyo, Japan. 20 Physicians used a transducer made of barium titanate with a tip measuring 10 mm in diameter and frequency of 2.25 MHz, submerged right under the surface of water, in a vinyl bag. The distance from the probe to the examined thyroid (through the water bag) was approximately 7 to 8 cm. The bag, with a transducer, was placed on the patient’s neck in close contact with the skin. At that time, the thyroid sonographic analysis was purely descriptive. Currently, gray-scale real-time sonography; spectral, color Doppler, and 3D imaging; elastography; high-frequency linear probes; high-resolution monitors; and powerful computer software create and record numerous measurements that have replaced the original thyroid imaging methods. According to Kim et al., 21 thyroid sonography has a 91.3% accuracy, 87.7% sensitivity, and 92.1% specificity for detecting asymptomatic diffuse thyroid diseases.
Sonographic Features
High-resolution linear transducers (7.5–15 MHz) are commonly used for thyroid sonography. In cases of severe enlargement and/or retrosternal extensions of the gland, convex or sector probes can be used to document the entire extent of the thyroid. A standard protocol for a thyroid sonogram includes 2D gray-scale imaging of the right and left lobes, isthmus, and, if present, the pyramidal lobe, with sagittal and transverse views. A standardized thyroid sonographic report should include the thyroid’s position, shape, size, content, echogenicity, and vascular pattern. 22 Three linear dimensions were measured for each lobe: the length (L) and anterior-posterior (A-P) diameters of each lobe were assessed on the sagittal view, while the width (W) was measured on the transverse view. Alternatively, the A-P dimension can be measured on a transverse image. A volume (V) of each lobe can be automatically calculated, after recording the abovementioned three linear dimensions (Figure 1) (using the ellipsoid equation with a correction factor: V (mL) = L (cm) × A-P (cm) × W (cm) × 0.523).
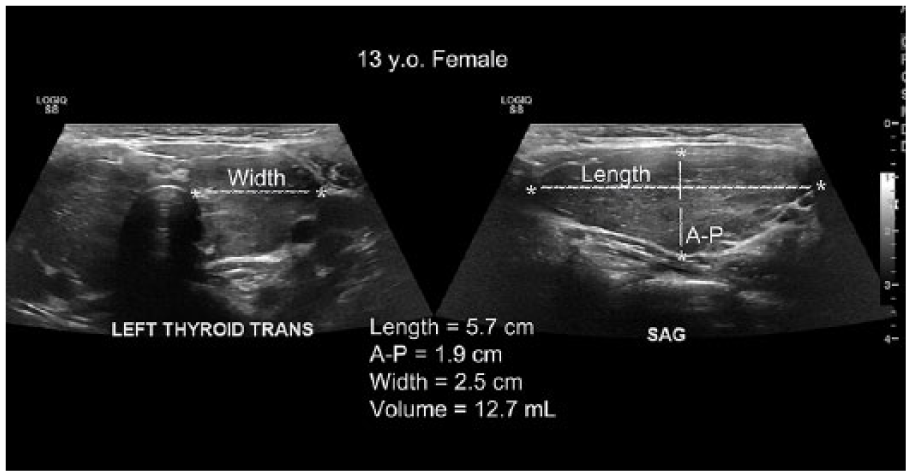
Gray-scale images of the left thyroid lobe with three linear measurements and volume: left side of the image shows a transverse view of the width (W); right side of the image shows a sagittal (longitudinal) view of the length (L) and anterior-posterior (A-P). The lobe’s volume equals 12.7 mL.
After measuring the volumes of each lobe, the total thyroid volume is calculated, as the sum of the right and left lobes’ volumes. The A-P dimension of the isthmus is also recorded (Figure 2).
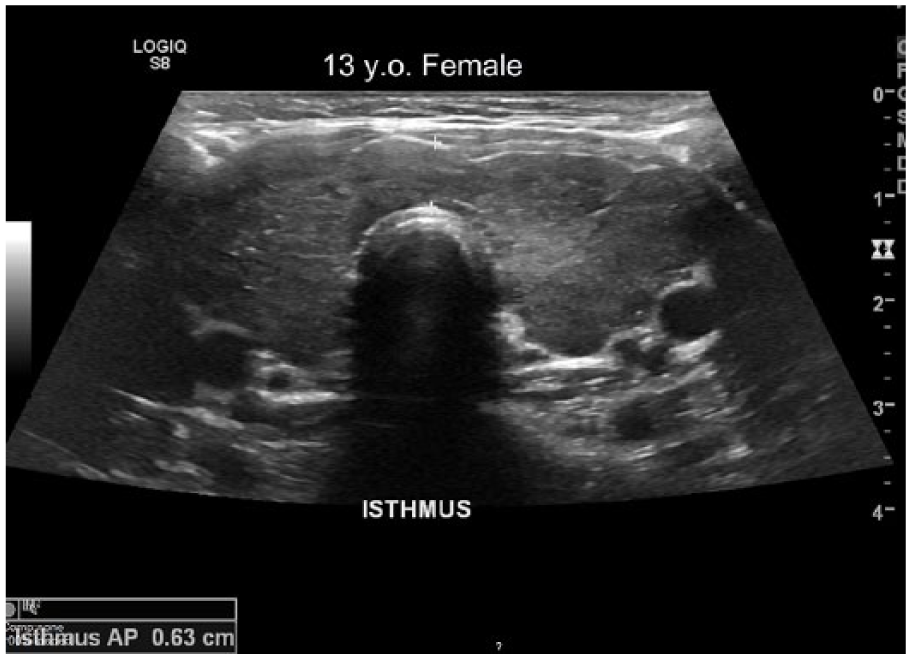
Gray-scale transverse image of the thyroid with the anterior-posterior dimension of the isthmus measuring 0.63 cm. Also, note diffuse hypoechogenicity and heterogeneity of the gland. (This patient was diagnosed with hyperthyroidism.)
If present, the pyramidal lobe is added to the total thyroid volume’s calculation. 22 Every thyroid nodule is measured and assessed individually, including its location, size, internal structure, and vascularity. Color and spectral Doppler allow assessment of the vascularity of the gland (Figure 3).
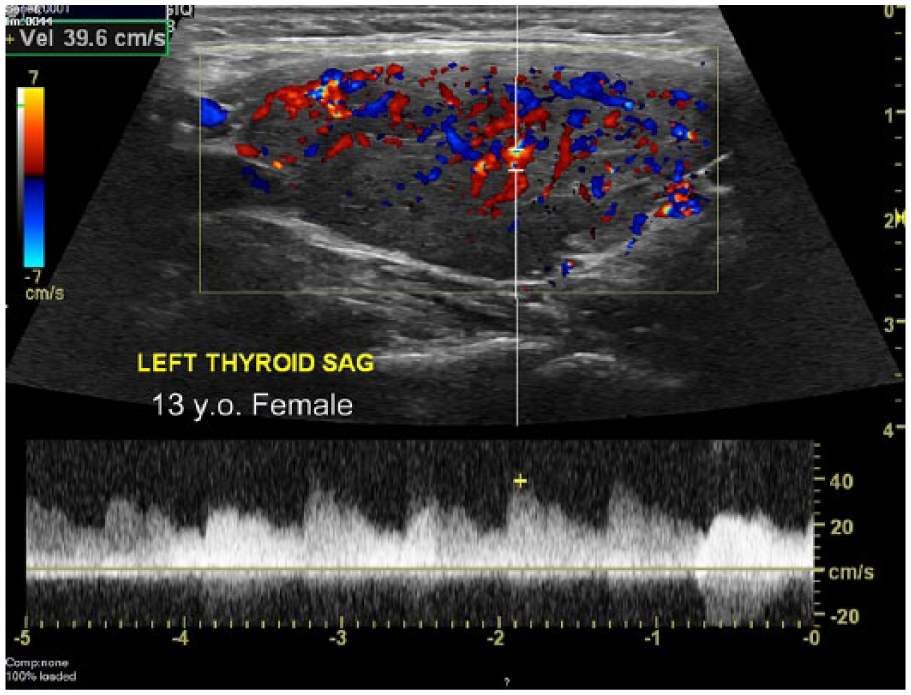
Sagittal view of the left thyroid lobe with color and spectral Doppler demonstrates hypervascularity, which is a common sonographic presentation of hyperthyroidism. It is the same patient shown in Figures 1 and 2. Considering that the right thyroid lobe volume of this 13-year-old female measured 13.4 mL, her total thyroid volume measured 26.1 mL (13.4 mL plus 12.7 mL).
According to the ACR, the cervical lymph node interrogation should be included as part of a standard thyroid sonogram. 8
Normal thyroid lobe dimensions change from birth into adulthood: the length (L or craniocaudal) diameter is 1.8 to 2.0 cm in newborns and 4.0 to 6.0 cm in adults, while the A-P dimension measures 0.8 to 0.9 cm in newborns and 1.3 to 1.8 cm in adults. 22 The limits of normal thyroid volume are 10 to 15 mL for adult females and 12 to 18 mL for males. 22
The WHO has documented normal thyroid volumes for children from 6 to 15 years of age in iodine-replete regions of the world, based on age, sex, and body surface area variables. This information can be referenced to the WHO guidelines. 23 Based on that data, an estimate of the maximum normal thyroid volume can be obtained by subtracting “1” from the calendar age, in years, for a group of children 6 to 11 years old, whereas for those 12 to 15 years old, the maximum normal thyroid volume would be equal to their reported age. For example, the upper limit of normal thyroid volume of an 8-year-old female can be calculated as 8 − 1 = 7 mL, matching the WHO’s estimate of 6.9 mL. Accordingly, a 13-year-old female’s maximum normal thyroid volume would be approximately 13 mL, equal to her calendar age and corresponding to the WHO guideline of 13.1 mL. 23
The 13-year-old female with hyperthyroidism presented in Figures 1, 2, and 3 had a total thyroid volume of 26.1 mL, but her thyroid volume should not have exceeded 13.1 mL, given the WHO guidelines. Her thyroid was also diffusely hypoechoic, heterogeneous, and hypervascular, with no nodules detected. All that information, including the thyroid volume, was a valuable addition to the results of her physical examination and blood panel. This complete set of data was used by that patient’s physician to determine her treatment: methimazole to control her hyperthyroidism and atenolol to control her heart rate. Moreover, recording that patient’s thyroid volume also provided a baseline, which can be used to monitor the progress of her treatment.
Methods and Clinical Significance of Thyroid Volumetry
There are various methods of measuring thyroid size and volume. The least accurate method in assessing thyroid size is physical examination. Common diagnostic radiologic methods such as 2D and 3D sonography (US), multiplanar computed tomography (CT), magnetic resonance imaging (MRI), photon emission tomography (PET), and planar scintigraphy (PS) are used for more precise measurements of thyroid volume. The absolute way of determining thyroid volume is by immersion of a resected thyroid gland. This can be accomplished by placing the gland into a measured reservoir filled with water after total thyroidectomy or autopsy. This method is based on Archimedes’ principle that an object displaces its own volume. Although this approach is highly accurate for volume computations, it is not applicable in routine clinical practice. 24
One of the most accurate radiologic procedures for the calculation of thyroid volume is multiplanar cross-sectional measurements on MRI, which have been used to determine thyroid volumes, with a coefficient of error less than 4%. 24 However, sonographically determined thyroid volumes also correspond well to the postsurgical measurements: a predicted thyroid volume under 25 mL was confirmed after thyroidectomies in 94% of cases. 25
Children’s calendar age and sex can serve as a simple reference for the maximum normal thyroid volume. 23 Regional differences play a significant role in determining the upper limit of normal thyroid volume. Nevertheless, a generalized approach based on whether a certain region of the world is iodine sufficient or not can also be used for the assessment of the thyroid size.
Evaluating thyroid size by its linear dimensions instead of the volume would not be as informative, including the example patient presented in this review. None of the gland’s three measurements (L, A-P, or W) can be used to define clearly the maximum normal thyroid size, especially in different pediatric age groups, sexes, and body constitutions. It is also undetermined whether all three linear dimensions, a combination of the two, or only one of the three must exceed the normal to diagnose goiter.
The data from different pediatric populations from iodine-sufficient parts of the world correlate well with the WHO nomograms. For example, Viduetsky 26 performed a study of the thyroid in children and adolescents of the Vinnitsa region in Ukraine in the late 1990s. Based on the results, the upper limit of normal thyroid volume for 13-year-old females is 12.1 mL, 27 which roughly corresponds to the WHO data of 13.1 mL. 23 In iodine-replete Japan, top normal thyroid volume for 13-year-old females is 11.9 mL. 28 In the iodine-sufficient area of Switzerland, it is approximately 12.5 mL. 29 Considering that the pediatric population of the United States includes a sizable immigrant minority from different parts of the world, including both iodine-deficient and iodine-replete regions, sonographic thyroid volumetry can assist in identifying endemic goiter and other thyroid disorders.
Sonographically measured thyroid volume is an operator-dependent procedure. Inevitably, technical factors influence the accuracy of thyroid volume estimated either on a 2D or 3D sonogram, especially if the thyroid has an irregular shape, is partially situated behind the sternum, or is very enlarged. Using the ellipsoid formula with a correction factor (provided as part of this review) to calculate the thyroid volume in a 2D approach results in a mean estimated error of approximately 15%. 5 The clinical case of the 13-year-old female with enlarged thyroid and hyperthyroidism presented demonstrates the importance of carefully monitoring the thyroid status in children, especially in adolescents. The maximal thyroid growth rate occurs at approximately 12.5 years of age. 29 Moreover, the burst in thyroid growth overlapping with the start of menarche in girls may cause a higher incidence of goiter during puberty. 29
Conclusion
Visual inspection and palpation of the thyroid gland are the accepted methods to evaluate thyroid size as part of a physical examination. However, the results of such examinations are often inaccurate and may lead to an incorrect diagnosis of a goiter. Sonographic estimation of thyroid volume is more precise than only the discrete linear dimensions of the individual thyroid lobes. Incorporating the length, anterior-posterior, and width measurements of each lobe into one computation provides better clinical information about the gland’s size as a whole organ. Thyroid volume is necessary for surgical planning, for proper calculations of radioactive iodine dose for thyrotoxicosis treatment, and in monitoring changes from different medications. There are regionally established normal values of thyroid volume based on body habitus, calendar age, and sex. Even though the US population is iodine replete and has a very low incidence of endemic goiter, health care professionals provide medical care to millions of patients born outside the United States, some of whom came from iodine-deficient parts of the world. Incorporating thyroid volume measurement into routine thyroid sonographic examinations in the United States for patients of all ages may improve the accuracy and the clinical value of thyroid sonograms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.