
Abstract
Objective:
Access to health care services, including diagnostic tools, such as sonography, remains limited in rural areas and could lead to negative health outcomes. Telerobotic ultrasonography (TUS) systems, which enable remote sonography from centralized locations, offer a promising solution to this challenge. This study examined the implementation of TUS in a rural community in southern Saskatchewan.
Materials and Methods:
A non-sequential mixed-methods research approach was used to study this intervention. A thematic analysis was conducted of the surveys and interviews that were conducted. The work was guided by the Canadian Network for Digital Health Evaluation Framework and Khan’s Access to Care and Prevention Framework.
Results:
Data were collected through 25 semi-structured interviews with providers (n = 11) and patients (n = 14). This was complemented by surveys from patients (n = 44). Findings revealed that accessibility, convenience, and timeliness of TUS significantly influenced acceptance and utilization. Patients valued the technology’s ability to deliver local care, minimizing disruptions like travel to an urban center. Among providers, enhanced coordination between technical and non-technical staff and service expansion emerged as pivotal for optimizing health care delivery.
Conclusion:
These results underscore the importance of increasing awareness and refining the integration of TUS to improve diagnostic access for underserved communities. The possibility of implementing TUS must focus on the magnitude of use and advancement directions to provide equitable health care delivery.
Access to health care services is a key determinant of health outcomes, with equitable access recognized as a constitutional right for Canadian residents. 1 However, significant disparities persist, particularly in rural and remote areas, where systemic barriers hinder timely and effective care, leading to poorer health outcomes.2,3 Rural and remote communities in Canada often suffer from inadequate imaging infrastructure and a shortage of trained professionals. These limitations hinder the provision of essential diagnostic services, including sonography, thereby affecting patient care. 4 Point-of-care ultrasound (PoCUS) has become increasingly valuable in emergency medicine over recent decades. However, its adoption in rural emergency medicine departments remains limited due to barriers such as insufficient equipment, training, funding, quality assurance, and difficulties in skill retention, and the capabilities of PoCUS are substantially limited compared to formal diagnostic sonography. 5
In Saskatchewan, where one-third of the population resides in rural areas, 6 geographic isolation further compounds these challenges. Research indicates that living more than 50 km from a tertiary health care center is associated with worsened health outcomes, particularly among vulnerable groups such as pregnant women, children, and the elderly.7,8 These populations face disproportionately negative health outcomes compared with their urban counterparts. 7
Accessing basic diagnostic tools like sonography remains difficult, even with the availability of telehealth visits, which only provide virtual health consultations. The team at the Virtual Health Hub has developed a model that integrates telehealth visits, point-of-care clinical examinations, remote diagnostic imaging, and remote pharmacy services. The current research focuses specifically on telerobotic ultrasound technology (TUS), which involves using a robotic arm controlled remotely by an expert sonographer. A patient-site assistant adjusts the robotic arm as needed during a live video call, enabling the capture of high-quality sonographic images essential for patient care and management. The TUS process enhances diagnostic accessibility in remote settings.
Recent studies have highlighted critical inequities in obstetric sonography access for rural residents, Indigenous populations, and low-income groups in Saskatchewan. 7 For instance, pregnant women in rural communities are 30% less likely to receive an obstetric sonogram, with Indigenous women 50% less likely compared with non-Indigenous women. 7 For example, in Gravelbourg, a rural community in southern Saskatchewan, pregnant women must travel 248 km round trip to Moose Jaw for a prenatal sonogram. Patients may often spend half a day away from work and family, while incurring substantial travel costs. 9 Despite sonography being covered by provincial health insurance, travel expenses, exacerbated by high gas prices, and the elimination of Saskatchewan’s public transit system remain a significant burden for patients.9,10
Sonography, a widely utilized imaging technique based on high-frequency pressure waves, is vital for the diagnosis of a range of medical conditions. 11 Yet, Saskatchewan and Canada are dealing with a large shortage of trained sonographers and retention in rural and remote areas remains a challenge, which further limits access. 12 As a potential solution, TUS offers a novel approach to bridging the gap in diagnostic imaging services in underserved regions.13 –15 This technology enables sonographers or radiologists to perform remote sonograms from centralized locations, thereby enhancing health care accessibility while maintaining diagnostic quality comparable to in-person imaging. 16
Although promising, the real-world implementation of TUS in rural and remote settings remains underexplored. The aim of this study was to address this gap by evaluating the impact of TUS in a rural community within Saskatchewan and capture the perspectives of patients and health care providers. By examining accessibility, convenience, and systemic challenges, this project was designed to better understand how robotic technologies can transform health care delivery in underserved communities.
Materials and Methods
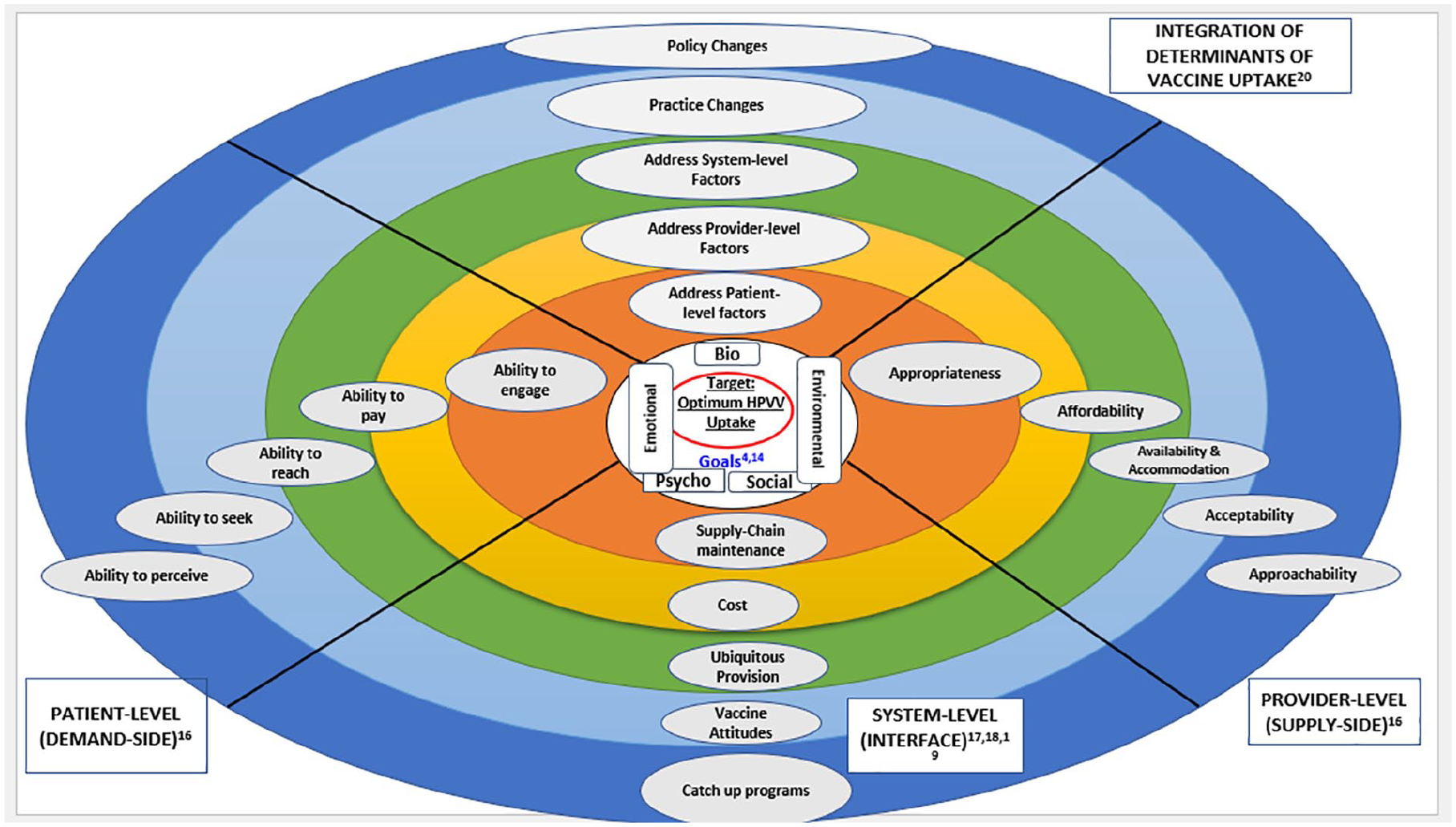
This study employed a dual framework approach that integrated the Canadian Network for Digital Health Evaluation (CNDHE) framework 17 and Khan’s framework: Access to Care and Prevention, 18 to guide its exploration of TUS implementation, in rural Saskatchewan. These frameworks were instrumental in shaping the study’s design, particularly in developing the interview guides, identifying key domains for analysis, and interpreting findings.
The CNDHE framework 17 is designed to evaluate the implementation and integration of digital health technologies, emphasizing domains such as usability, operational effectiveness, and health care system integration. This framework provided a structured lens to examine how TUS functioned, within the existing health care infrastructure of a rural community. In parallel, Khan’s framework: Access to Care and Prevention 18 offered critical insights into systemic barriers and equity considerations, focusing on patient-centered care delivery and the intersection of social determinants of health with health care accessibility. This framework was particularly valuable in addressing themes of equity, patient empowerment, and the impact of health care innovations on underserved populations and informed the exploration of patient experiences (See Figure 1). It ensured that the study captured not only the technological aspects but also the socio-ecological factors that influence the adoption and utilization of TUS services.
Khan’s framework: access to care and prevention.
Research Setting
This study was conducted in a rural community in southern Saskatchewan, Canada, with a population of 986, based on census data. 19 This community was served by the local hospital, where TUS was being offered, but operated remotely by a sonographer based at the Royal University Hospital in Saskatoon, approximately 248 km away. The TUS system uses secure videoconferencing and remote control software; sonographers operate the TUS system from a distance. A patient-site assistant adjusts the robotic arm as needed during a live video call. Patients are scheduled through standard procedures but, instead of an on-site sonographer, a robotic arm performs the examination under remote control. A patient-site assistant positions the frame for the transducer, while the remote sonographer performs fine movements and controls ultrasound settings. Sonographic images are transmitted to the picture archiving and communication system, with routine reports available by the next day and urgent findings communicated immediately. Radiologists can review images in real time and collaborate with sonographers via voice or text, ensuring seamless diagnostic oversight.
The study focused on assessing the impact of the TUS system on health care accessibility, particularly in rural settings, where patients and providers face logistical and systemic challenges.
Research Study Design
This study utilized a qualitatively driven, non-sequential mixed-methods design20,21 to evaluate the impact of the TUS system on health care accessibility in rural settings. This was accomplished through capturing the perspectives of patients and health care providers. Reporting of findings followed COREQ guidelines. 22 Semi-structured interviews served as the primary method of data collection, complemented by patient surveys to provide additional quantitative insights. Ethical approval for the study was obtained from the University of Saskatchewan Research Ethics Board before the commencement of data collection. The interviews were designed to explore participants’ experiences and perceptions of TUS, focusing on themes of accessibility, convenience, and systemic challenges. To guide these discussions, interview questions were developed using domains from the CNDHE framework 17 and Khan’s framework. The interview guides were iteratively refined by three researchers to ensure alignment with the study objectives and relevance to the participants’ context. Surveys complemented these interviews, allowing for the collection of broader patient-reported data related to their experiences with the technology. While patients and the public were not involved in the study’s design or planning stages, they played an integral role in the research through their active participation in interviews and surveys. This approach ensured that their voices contributed to the understanding of TUS services and their potential to address health care disparities in underserved rural communities. By employing this qualitatively driven mixed-methods approach, the study captured a comprehensive picture of the multifaceted impact of this innovative technology.
Participant Sample and Recruitment
Participants were recruited through a purposive sampling strategy, using a combination of direct outreach and collaboration with local health care providers. Patients who had undergone TUS examinations at the community hospital in rural Saskatchewan were identified and invited to participate. Health care providers involved in the delivery of these services, including both technical staff (i.e., sonographers) and non-technical personnel (i.e., administrative staff), with a minimum of 1 year of experience, were also invited to participate. Recruitment was facilitated by a patient-site assistant for patients and by site managers for providers, which ensured a streamlined process. Participation was entirely voluntary, with no financial compensation offered, and efforts were made to accommodate participants’ schedules by conducting interviews via telephone or Zoom, thereby enhancing accessibility and convenience. Only patients who indicated willingness on the surveys to participate in interviews were contacted to schedule an interview. Except for one patient, all participants who indicated willingness to participate took part in the interview.
Data Collection
Data collection was carried out between November 2023 and April 2024 by a research team at the University of Saskatchewan. The research team comprised physician-scientists, a population health officer, a radiologist, a senior tele-diagnostic imaging services specialist, and a virtual care operations manager. The team used a combination of surveys and semi-structured interviews to capture the perspectives of patients and providers on TUS services. Surveys were distributed exclusively to patients and facilitated by a patient-site assistant based in the rural community. All participants provided written consent prior to completing the surveys. Responses were anonymized at the point of collection and digitized for subsequent analysis. The physician-scientist conducted semi-structured interviews. The interviewer had no prior relationship with patients; however, she was known to the researchers on the team and providers of the TUS services. Interviews were the primary qualitative data source, focusing on participants’ experiences with TUS, particularly regarding accessibility, convenience, and systemic challenges. The interview guide was pilot tested with a sample of one provider and two patients to find areas of improvement and guide the creation of prompts in the interview guide. The interview guide incorporated open-ended questions and was iteratively refined by three researchers to ensure a robust gathering and reflective understanding of the data. Preliminary results were discussed with some participants to reveal convergences or divergences in data. Interviews were conducted virtually via Zoom and telephone, accommodating participants’ geographic constraints and schedules. Each session lasted between 25 and 35 minutes and was audio-recorded with participants’ informed consent. Consent for interviews was gathered during the preliminary survey, where participants were asked at the end of the survey if they would be willing to share their experience with the new technology in a brief interview. Those who agreed and provided their preferred contact method were later reached out to for scheduling an interview.
The interviewer, trained in qualitative research methods, obtained consent and summarized the study’s objectives, aims, and goals to the participants in an easily understandable way and employed follow-up questions, probing techniques, and clarifications to ensure depth and richness in participant responses. In addition, the interviewer practiced reflexivity by actively reflecting on her biases, assumptions, and preconceptions throughout the research process, including employing strategies to minimize the potential influence on study design, data collection, analysis, and interpretation. These strategies involved maintaining a reflexivity journal to document thoughts and reactions, engaging in regular discussions with the research team to challenge interpretations, and ensuring the use of open-ended, neutral questioning techniques during interviews to prioritize participants’ perspectives. This approach facilitated a conversational dynamic, allowing participants to provide nuanced accounts of their experiences with TUS services. Anonymity and confidentiality were maintained throughout the process, with all recordings and transcripts securely stored. Moreover, besides the participants and researchers, no one else was present during the data collection and analysis. Surveys complemented interviews, offering additional insights into patients’ views and enhancing understanding of telerobotic ultrasound’s impact on rural health care delivery.
Data Analysis
Analysis of the impact of the TUS systems on health care accessibility required a qualitative thematic analysis approach guided by Braun and Clarke. 23 A hybrid coding approach was utilized, combining deductive codes derived from the CNDHE framework 17 and Khan’s framework 18 with inductive codes that emerged directly from the data. Audio recordings of the interviews were transcribed using Otter AI and independently reviewed by two researchers for accuracy, cleaning, and de-identification. The anonymized transcripts were uploaded to NVivo, version 14 software for qualitative analysis, which facilitated the systematic exploration of key patterns and themes. Following the CNDHE framework, the analysis explored domains such as technological efficacy, usability, and health care integration, while Khan’s framework provided insights into systemic barriers, equity considerations, and patient-centered care. The coding process began with familiarizing transcripts through multiple rounds of reading and correlation with the field notes, where researchers immersed themselves in the data to identify preliminary patterns. Deductive codes, informed by predefined themes from the two frameworks, included “accessibility,” “timeliness,” and “equity,” while inductive codes such as “patient empowerment” and “logistical challenges” emerged during data engagement. Thematic development was iterative and collaborative, involving regular discussions to refine the coding structure and consolidate emerging categories into broader themes. A coding matrix was created to map these themes to their respective frameworks, ensuring coherence and alignment with the study objectives. The CNDHE framework was instrumental in identifying themes related to the operational and functional aspects of the TUS system, such as its integration into existing workflows and its ability to address the accessibility gap. In contrast, Khan’s framework highlighted systemic inequities and the potential for technology to enhance patient-centered care delivery, particularly for underserved populations. Together, these frameworks provided a comprehensive lens to evaluate the interplay between individual experiences and systemic health care challenges. The analysis revealed a nuanced understanding of how TUS influence health care delivery in this rural setting. Thematic categories such as “technical and logistical barriers” and “equity in care access” encapsulated the multifaceted experiences of participants. Data saturation was achieved when no new themes emerged, ensuring the robustness of the analysis. Double coding of all transcripts enhanced the reliability of the findings, with discrepancies resolved through re-evaluation and consensus discussions. Anonymized quotes from participants were included to substantiate key findings, providing rich and contextual insights into their experiences with the technology.
Results
A total of 44 survey responses were collected from patients who had a TUS examination. Telerobotic ultrasonography significantly improved accessibility and convenience for patients in this rural area, and 100% of the respondents were satisfied with the service. A total of 65% of the respondents had previously been referred for a sonogram, and 69% had undergone at least one sonogram in the past 5 years. Notably, 53% of respondents did not face delays due to scheduling difficulty, and 79% reported no delays due to transportation issues. On average, patients travelled approximately 117 km for the examination. Patient preferences showed that 40% would opt for TUS if conventional services were delayed, 30% preferred telerobotic over conventional methods, and 28% were indifferent. Furthermore, 91% did not encounter any difficulties using TUS, with 98% reporting no issues in scheduling appointments. These findings underscore the high satisfaction and acceptance of TUS in this cohort and highlight the potential to enhance healthcare delivery in underserved regions. A summary of the survey questions and descriptive statistics of the survey responses is provided as an appendix (Please scan the QR code for Table 1).
A total of 25 participants (providers [n = 11] and patients [n = 14]) were recruited for semi-structured interviews. Patients were adult males, females, and pediatric subjects under age 18 who underwent TUS for abdominal, renal, pelvic, and obstetrical sonograms. Providers included a tele-diagnostic imaging services specialist, primary care providers, radiologists, a robotics engineer, a robotics manager, a patient-site assistant, a program manager, a manager of operations, and telerobotic sonographers. Providers had at least 1 year of experience developing, operating, or supporting TUS clinics across various rural and remote communities in Saskatchewan.
Results of interview data are reported based on themes identified from patient and provider interviews. Interestingly, more convergences than divergences of participants’ perspectives were found during data analysis. The thematic analysis of patient interview transcripts identified three major themes: (1) accessibility, convenience, and timeliness; (2) comparability to conventional ultrasound procedures; and (3) technical, logistical, and other aspects. The provider interview transcripts also identified three major themes: (1) operations and provision of telerobotic ultrasound, (2) launch and awareness of telerobotic ultrasound, and (3) future improvements and recommendations. Emergent themes and subthemes with exemplary quotes from patient and provider interviews are provided in the discussion below.
Patients’ Perspectives
The participants expressed the importance of the accessibility and availability of sonographic services in their home community. Many patients highlighted reduced travel time as a major benefit of TUS. For many, the ability to access sonographic services, within their community, rather than traveling to a distant urban center significantly improved their healthcare experience. Considerable reduction in travel time made it easier for them to attend appointments without the need for a long commute to larger urban center.
Several patients highlighted that the TUS service was quick in terms of seeking a time for an appointment as well as receiving results. The prompt availability of results was deemed critical for effective patient management, reducing the anxiety associated with waiting and enabling timely medical decisions and treatments. Timeliness of service was consistently noted by patients, emphasizing the efficiency of TUS operations. An example quote from a patient was:
It helped you for the purpose you were there. Like for diagnosis or referral or treatment or management. It did help in that way because it was very quick. Like if I was waiting for a conventional ultrasound, I might wait another month yet. Also, my results were back within a week.
The efficiency of scheduling and quick turnaround time for appointments were repeatedly mentioned as positive aspects. Patients appreciated the reduced waiting times compared with traditional sonographic services. Patients highlighted the streamlined scheduling process, contributing to a smoother and more efficient patient experience.
Comparability to Conventional Sonographic Procedures
Patients found the telerobotic ultrasound process comparable to that of conventional, noting minimal differences in the actual procedure. They noted that familiarity with the overall procedure helped reduce anxiety and increase acceptance of the new technology. An example patient comment was: “It was just like having pretty much similar to having it done in the hospital. I couldn’t tell any difference really except . . . I was listening to her (the remote sonographer).”
Patients generally felt comfortable with the remote operation of sonography, appreciating the advancements in technology. Patients discussed that acceptance of technological advancements was a positive indicator for the future adoption of TUS systems in this and other communities.
Technical, Logistical, and Related Aspects of Care
A significant number of patients reported issues with locating the TUS clinic due to inadequate signage and a lack of community awareness. Patients suggested improving signage and directions within the health care facility to ensure patients can find their way to their appointments. In addition, patients suggested various methods to improve awareness and acceptance of TUS, including local advertising and information dissemination through health care providers. Patients cited that effective promotion and clear communication can significantly enhance patient engagement and utilization of TUS services. Patients made this observation: “There were no signs posted; you were not given any map of where it is located in the basement. Some people might have benefited from better direction in the building.” “Also, there is no community awareness . . . maybe have it on the local website or promote it through the physician and the nurse practitioners.”
Some patients noted the lack of personal interaction with the remote sonographers as an area for improvement, suggesting that a more personable approach could enhance the experience. Patients deemed that building rapport with patients, even through remote interactions, can help make the process more comfortable and reassuring for patients.
Patients highlighted those logistical issues, such as the clinic’s location in the basement and the lack of clear instructions, had made navigating the facility and locating the TUS clinic challenging. Addressing these challenges is crucial to improving overall patient satisfaction and ensuring smooth access to services. A few patients also reported that the waiting room was not well indicated.
Providers’ Perspectives
Providers generally found the TUS system easy to use and efficient in terms of operation and provision. The quick booking and reporting times were frequently highlighted. The efficiency and privacy associated with the TUS system were critical factors that enhanced the overall health care delivery process, allowing for quicker diagnoses and treatment planning. Moreover, providers discussed that the technology has significantly improved access to essential diagnostic services for patients in rural areas, reducing the need for long travel times and making health care more accessible. The accessibility of TUS in rural areas is a major advantage, particularly for elderly patients who may have challenges traveling long distances for medical care.
Overall, patient feedback has been positive, with many appreciating the convenience and quality of the TUS services. However, there are areas for improvement, particularly in patient navigation and understanding of the technology. Positive patient feedback indicates high satisfaction, but addressing specific concerns about navigation and communication can further enhance the experience. In addition, providers reported that patients communicated their struggle with navigating the facility to access the TUS services, particularly due to the location of the services in less familiar areas of the hospital. One provider made this remark:
Patients were actually very happy with the service . . . I cannot think of a single patient that had any sort of criticism; However, I strongly suggest that integrating telerobotic ultrasound with other diagnostic services could enhance its utility and convenience for patients.
Operational challenges included the need for better communication between providers and the administrative team handling the telerobotic services. Providers deemed that effective communication was essential for the smooth operation of telerobotic services, and addressing these gaps can further enhance the system’s efficiency.
Launch and Awareness of TUS
Providers deemed that health care professionals play a crucial role in promoting TUS services to patients and their endorsement can significantly enhance acceptance and utilization. Providers highlighted that their recommendations and reassurance about the quality and reliability of TUS are vital for patient acceptance of this remote service.
Many providers discussed that while the initial launch included efforts to raise awareness through local newspapers and postings, there is still a need for more comprehensive communication strategies to ensure that both patients and providers are fully informed about the available services. Continuous and diverse methods of communication, such as social media, community postings, and direct communication from health care providers are necessary to keep the community informed. Despite efforts to inform the community, some patients remain unaware of the services, highlighting the need for improved strategies to disseminate information. This was exemplified by this patient statement:
I know when the service was launched the local newspaper did have actually quite a nice write-up about it. But obviously not everybody reads the newspaper. So, they kind of start turning around the hospital they don’t know where to go.
Future Improvements and Recommendations
Many providers recommended expanding the range of services offered through TUS, such as including Doppler and other specialized examinations, to meet more comprehensive diagnostic needs. Doppler is critical for diagnosing conditions like a deep vein thrombosis (DVT), which require urgent attention. The absence of such services limits the utility of the TUS system and forces patients to seek these tests elsewhere, often involving travel and additional wait times. Providers emphasized that expanding the capabilities of TUS services can enhance their value and utility for a broader range of medical conditions. Expanding the service to include a broader range of diagnostic tests would improve its effectiveness and ensure patients receive the necessary care promptly. This was illustrated by this provider’s comment:
Another burden here is like we don’t have kind of an extensive service. It’s just once a week like one day per week which makes you know create some limitation to the numbers they can do. And also, I’m not really sure how it works but they just do abdomen and pelvic. So, let’s say if you need kind of an urgent ultrasound for DVT like I would really appreciate if kind of a Doppler ultrasound could be added to the service as well. I’m not sure if this is a possibility you know we do a lot of pelvis like soft tissue ultrasounds. You know lumps and bumps and shoulders and joints. I’m not sure if it’s possible for that to be added to the current list.
Providers highlighted the importance of improving communication among providers, administrative staff, and patients to enhance telerobotic ultrasound service delivery. Streamlining communication processes can reduce errors and improve patient satisfaction. Providers expressed frustration over inadequate communication between technical and non-technical staff, leading to follow-up delays and emphasized the necessity for better communication channels to ensure timely requisition processing.
Providers emphasized the importance of increasing public awareness and education about TUS to alleviate patient anxiety and improve acceptance. They suggested that clear, comprehensive information about the procedure could manage patient expectations and enhance their overall experience. Providers advocated for accessible information dissemination through platforms like social media and community postings to familiarize patients with TUS and mitigate potential surprises or confusion.
Discussion
The key findings of this study examining experience with TUS services were (1) the significant potential improvement in accessibility and convenience of sonographic services for rural and remote communities, (2) the high level of potential acceptance among patients and providers for the TUS technology, and (3) the critical need for expanding services and improving communication and coordination within the health care system.
The implementation of TUS has notably improved the accessibility of diagnostic services for this cohort of patients, as well as reducing travel time and wait times for appointments. This aligns with previous literature emphasizing the importance of telehealth technologies in bridging healthcare gaps in underserved areas.24,25 The convenience of local access to high-quality sonographic services has led to positive patient experiences, highlighting the potential for telehealth to enhance healthcare delivery in remote regions.
There is a clear need to expand the range of diagnostic services offered through TUS, including venous and arterial Doppler and soft tissue sonograms, and to improve communication and coordination among healthcare providers and administrative staff. Previous research has highlighted similar challenges in telehealth implementation,24,26 underscoring the necessity for comprehensive service offerings and seamless and secure communication channels to optimize healthcare delivery. Addressing these issues is crucial for maximizing the utility and efficiency of telehealth services.
Limitations
The study has several limitations, primarily concerning the generalizability of findings due to its qualitative nature and specific geographic and demographic focus. The study concentrated on a single rural community, and participant experiences may not reflect those in other regions or health care contexts. While the sample size was adequate for qualitative analysis, broader populations, especially in diverse geographic or cultural settings, warrant consideration in future research. Moreover, reliance on self-reported data introduces potential social desirability bias. The study’s time frame may also limit capturing the long-term impacts and sustainability of TUS services. Future research should explore larger, more diverse samples and employ mixed methods approaches over extended durations to enhance the robustness of findings.
Conclusion
The introduction of TUS technology was well received in this rural community due to its accessibility, convenience, and timeliness, as it allowed for quality diagnostic imaging without the need for extensive travel. However, it is noted that improvements would be needed to foster community awareness, communication, and logistical support within other healthcare facilities. Addressing these issues could refine the TUS program, enhance patient experience, and promote broader acceptance of this technology. Policymakers and healthcare providers should consider these insights to optimize telehealth strategies and promote health care equity, which could improve healthcare delivery efficiency for all patients.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793251326870 – Supplemental material for Enhancing Ultrasound Access in Rural Saskatchewan: A Mixed-Methods Study of Telerobotic Technology
Supplemental material, sj-docx-1-jdm-10.1177_87564793251326870 for Enhancing Ultrasound Access in Rural Saskatchewan: A Mixed-Methods Study of Telerobotic Technology by Amal Khan, Scott J. Adams, Brent Burbridge, Stacey Lovo, Joseph P. Deason and Ivar Mendez in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
We would like to extend our gratitude to all the patient and provider participants who consented to take part in this study. Special thanks to the family practitioners from Gravelbourg for their assistance with participant engagement and overall support of the research. We greatly appreciate Ms. Casandra Rushinko for her help with survey and interview data collection and participant recruitment and Ms. Abby Jia for her help with organizing and entering survey data. We acknowledge the contributions of all members of the Virtual Health Hub team, particularly Ms Martine Pringle for data organization and Dr. Corinne Berger for her assistance with the survey data entry and analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for this research project was received by Saskatchewan Health Research Foundation (SHRF), 2022-23 Collective Impact Focus: Rural and Remote Healthcare, Impact Grant, Grant # 6309.
Ethics Approval
Ethical approval for this study was obtained from the University of Saskatchewan Research Ethics Board (Bio-REB-15-276).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.