
Abstract
Background
Mandarin-speaking consumers requiring interpreter services face significant barriers to telehealth access in Australia, often due to systemic and cultural disconnects which widens healthcare access disparities. This qualitative cross-cultural cross-lingual study explored the perspectives of Mandarin-speaking individuals at a metropolitan hospital in Queensland to identify barriers, enablers, and solutions for equitable telehealth access.
Methods
Three Mandarin cross-lingual focus groups were conducted. Situated within the interpretive research paradigm and informed by intersectional critical inquiry, consumers described their perspectives on lived experiences interacting with the tertiary healthcare system while accessing telehealth and requiring interpreter services. Analysis was conducted by two researchers, starting with open coding, cross-checking and application of an intersectional lens.
Results
Eight Mandarin-speaking consumers and two carers attended three cross-lingual focus groups with qualified real-time interpreters. The analysis revealed six themes: 1) lack of telehealth awareness; 2) clinicians are gatekeepers of telehealth services; 3) the healthcare system is monolingual; 4) navigating the healthcare system is disempowering; 5) power is transferred to interpreters and carers; and 6) alternative solutions do not align with participants needs. Participants expressed openness to telehealth but emphasised the need for culturally sensitive and clearly communicated options.
Conclusion
This study reveals significant challenges accessing telehealth for Mandarin-speaking consumers needing interpreter services in metropolitan Queensland and highlights that clinician assumptions and the monolingual nature of healthcare services as major barriers. While video interpreting is often recommended, participants preferred simple, safe, and culturally appropriate communication strategies. Co-designing telehealth solutions with multicultural consumers can prevent the deepening of existing inequities and to foster inclusive healthcare practices.
Keywords
Introduction
Language barriers contribute significantly to disparities in access to healthcare, 1 especially for culturally and linguistically diverse (CALD) communities in Australia.2–5 Among these communities, language-related barriers are linked to reduced uptake of health services, 6 increased prevalence of non-communicable diseases, 7 higher rates of complications, 8 and a lack of trust in the service provision when compared to their English-speaking counterparts. 9 Conversely, in the absence of these barriers, CALD communities report higher rates of prevention program uptake 8 and increased health literacy, 10 leading to better self-management of health conditions and greater satisfaction with service provision, including in-person and telehealth modalities of care.11,12
Strategies to overcome language barriers typically involve using interpreters, training healthcare providers in cultural competence, and implementing health navigators. 13 However, while these strategies seem feasible and effective, they are not routinely integrated into healthcare provision. Tang et al. attribute the low uptake of interpreter services to a lack of clinician knowledge around accessing interpreters, limited interpreter availability, and non-professional forms of interpreting (such as family members or non-clinical staff). 6 Unaddressed language barriers combined with a lack of health literacy and trust in healthcare provision limit access to telehealth, perpetuating health inequities among CALD communities.7,14 However, solutions to address these barriers have been typically analysed one-dimensionally, failing to integrate the intersectional multidimensional nature of inequities. 15 Given these findings, further studies should explore these barriers and their interactions with the healthcare system through a cross-cultural lens. A cross-cultural lens can support the modification of healthcare service provision by incorporating consumers’ perspectives, which will ultimately optimise the reach, engagement, and benefits of virtual care interventions. 16
To overcome the challenges of accessing and navigating the health system, healthcare delivery options, such as virtual care, could reduce healthcare access barriers for CALD communities living in Australia while providing effective care and reducing geographical barriers,17,18 representing an opportunity for improving health equity. However, the increased adoption of telehealth during and after the COVID-19 pandemic has widened existing inequities of access for CALD communities.19,20 Moreover, CALD communities in Australia are reportedly among the least likely recipients of telehealth services. 21 As such, strategies must be explored to overcome language barriers and improve equity of access to healthcare (including telehealth) among CALD communities. For this, a cross-cultural lens is needed.
Mandarin-speaking communities living in metropolitan areas
Chinese Australians represent one of the largest CALD communities, with approximately 1.4 million people in the Australian population (approximately 6%). 22 While multiple languages and dialects are spoken in mainland China, Mandarin remains the dominant language. 23 Mandarin-speaking communities, like other CALD communities, face language barriers, directly impacting their ability to navigate the Australian healthcare system. 22 These barriers can result in restricted uptake of healthcare services, mistrust in medical services and ultimately increased health-related costs.24,25 For example, their cultural experiences and perceptions of medical services in Australia can differ culturally from those provided in China. 25 Consequently, Australian healthcare provision can be perceived as time-consuming compared to the hospital-based Chinese medical health system. 25 In light of this concern, cross-cultural solutions have been proposed to overcome the structural, cultural, and language barriers that emerge from these healthcare interactions.16,26 However, there is limited cross-cultural evidence from Mandarin-speaking communities that informs solutions to accessing healthcare in Australia. While healthcare services explore ways to enable better access to healthcare for CALD communities, consideration of lived experiences is critical for the optimisation of these strategies. Therefore, using a cross-cultural lens and informed by intersectional critical inquiry, this study aims to explore the experiences of accessing telehealth among Mandarin-speaking individuals who require interpreter services in metropolitan Queensland, Australia. Our results will support the development of practical solutions that enable more equitable access to telehealth.
Telehealth access barriers are multifactorial and, therefore, complex. 27 Given this complexity, evidence incorporating consumer perspectives remains limited. This highlights the need for active involvement of consumers in the planning of these services and to improve cultural appropriateness and acceptability of telehealth services.26,28 Understanding the CALD consumer experience at the health system level is necessary to implement culturally informed, equitable solutions that can translate into more positive health outcomes and consumer experiences. Given the intersectional nature of health inequities and language barriers among CALD consumers, this study aimed to examine the experience of CALD consumers, such as Mandarin-speaking individuals, who require interpreter services when accessing telehealth in a tertiary hospital in metropolitan Queensland, Australia.
Materials and methods
Study design and setting
This study had a qualitative design and was conducted in collaboration with the interpreter services of a tertiary hospital located within Metro South Health (MSH) between November 2023 and November 2024 in Brisbane, Australia. MSH Interpreter Services (MIS) serves a diverse community, considered the most culturally diverse area in Queensland, with 20% of the population (approximately 19,000 people) having a first language other than English. 29 Previous research involving the same region demonstrated that CALD consumers are 66% less likely to be offered telehealth services when they need interpreter services. 21 Similarly, Mandarin is one of this region's most commonly requested languages for interpreter services. For these reasons, we designed our study to explore personal experiences accessing health services in the MSH region from the perspective of Mandarin-speaking people. We adopted the Standards for Reporting Qualitative Research (SRQR). 30 The Metro South Research Ethics Committee approved the study (HREC/2023/QMS/95080). The process of the study design is described in Table 1.
Summary of steps undertaken for the study from planning to synthesis.

*Team members described with their initials.
Participant recruitment
A convenience sampling strategy based on telehealth experience was used. 31 Given the exploratory nature of the study, our sample size was determined by the need to examine meaningful telehealth access among Mandarin-speaking participants who required interpreter services. Consequently, a small sample size was sufficient given our narrow study aim, the specificity of our sample, and the anticipated richness of data. We focused on exploring individual experiences in depth; this means richness of input rather than the number of participants. As such, information power 32 allowed us to recruit a small sample of Mandarin-speaking participants while maintaining rigour. We sought to capture diverse experiences and perspectives within the Mandarin-speaking cohort, balancing variation with feasibility and ensuring deep engagement in the hospital context. We recruited Mandarin-speaking participants who required interpreter services for their medical consultations at a MSH hospital and had experience with any modality of telehealth offered in the same hospital (telephone or videoconferencing). Participants with no prior self-reported experience with telehealth were excluded from the study.
Recruitment process
The initial step in our recruitment process was stakeholder engagement. The Health Equity and Access Team from MSH, MIS, as part of their routine care, identified participants who had an existing booking for an outpatient appointment with an interpreter.21,33 MIS provided translated study information to potential participants in their language, in written and oral form. If participants agreed to participate in the study, Mandarin-speaking members of the research team (YL, XZ) contacted potential participants via telephone to ensure a clear understanding of the study, coordinate an appropriate time for the focus groups and to plan for any additional needs (such as parking, food preferences and accessibility). To ensure complete understanding and voluntary participation, written informed consent was obtained from all participants in their preferred language (English or Mandarin) before each in-person focus group session. This process was assisted by Interpreters, carers and/or Mandarin-speaking researchers. Given the initial telephone contact with participants, the risk of coercion was minimal. The recruitment process is graphically represented in Figure 1.

Recruitment process for cross-cultural, cross-lingual focus groups. MIS: Metro South Health Interpreter Services.
Data collection
Three cross-lingual focus groups were conducted in person using real-time, certified Mandarin interpreters. The development of focus groups was informed by the recommendations of Quintanilla et al. and their cross-lingual, cross-cultural work exploring maternal health among a diverse group of women living in Canada. 34 Using a convergent–divergent approach, questions explored participants’ journey accessing telehealth (telephone and videoconferencing), perceptions of telehealth - including perceived barriers and potential opportunities for accessing telehealth services (see Supplementary File 1 for the focus group guide). Focus groups occurred in a research centre within the hospital campus, for up to 90 min in duration. The research team conducting the focus groups consisted of two non-Mandarin-speaking researchers and two fluent Mandarin speakers (at least one attended each focus group). At the same time, one certified Mandarin interpreter assisted researchers in real-time interpreting, which allowed for enriched data with follow-up questions. Mandarin-speaking researchers assisted with verifying the accuracy of translations derived from simultaneous code switching during the real-time interpretation. Given our sampling strategy based on information power, and based on the recommendations of Malterud et al., 32 the concept of data saturation was not appropriate to our study. Therefore, our sample size provided sufficient data, given our niche sample and the anticipated richness of data.
Analysis
An overview of the analysis process is provided in Table 1. Data from the focus groups were transcribed automatically in English using the Zoom® meeting transcription tool into a Microsoft Word document. These transcriptions included real-time translations from Mandarin to English during the focus groups. Transcriptions were checked and deidentified by VG. Then, using de-identified transcripts, a member of the research team, with the National Accreditation Authority for Translators and Interpreters (NAATI®) translator (LZ), verified the accuracy of the real-time translation. These documents were uploaded to NVivo® software for coding. Two independent English-speaking coders (VGR and JK) performed the coding, informed by intersectional theory. 35
Initial coding
Transcripts were openly coded to explore the ways in which age, race and language intersect in shaping participants’ experiences accessing telehealth services to identify critical intersections between the consumer and the health system. 36 To ensure coding reliability, the coders (VG and JK) first developed a shared codebook based on initial transcript reviews and then coded a transcript independently. Discrepancies were discussed and resolved through consensus, and the codebook was refined iteratively.
Key stage organisation
Participants’ experiences were organised around five key stages: (1) telehealth offered by the clinician, (2) booking a telehealth appointment, (3) preparing for your telehealth appointment, (4) meeting with the clinician via telehealth and (5) after the telehealth appointment. As conceptualised by Crenshaw (1991) 37 and further developed by Collins (2019), 35 the core constructs of intersectionality, including relationality, power, social inequality, social context, complexity, and social justice, were considered to inform the development of initial coding and themes. Using intersectionality's core constructs, the analysis revealed six themes describing barriers to telehealth access, how these barriers shape participants’ social status within the health systems, and their relationship with the health system as a structure.
Theme development
The next step was developing themes, searching for connections across emergent themes, seeking patterns across cases and moving the interpretation to a deeper level by reviewing themes and using temporal referents to understand the meaning of the participants’ experience. Themes were then reviewed and discussed with the research team to be refined and verified. Several strategies were used to ensure the trustworthiness of the findings. These included providing focus group guides for real-time interpreters and researchers, checking recordings with a certified English-Chinese translator, and maintaining a reflective journal to document the research process and potential biases introduced during the analysis. Member checking was not performed. While data saturation was neither appropriate nor discussed, our small sample had sufficient information power for the research question and knowledge-generating purposes of the study. The process is described in Table 1.
Intersectionality as critical inquiry
This study is informed by intersectionality as a critical inquiry as described by Collins. 35 While the definition of intersectionality has yet to reach a consensus, for the purpose of this piece of work, intersectionality is used as an analytical tool to investigate how power relations shape social relationships, considering that multiple social categories such as gender, race, class, ability, age and ethnicity intersect.15,37–40 This approach helped consider the multiple social, cultural, and systemic influences on the digital divide in telehealth access across Australia.39,41
This study considers accessing telehealth in the Australian health system as having multiple layers in which race, age, ability and ethnicity interplay to create a phenomenon of access to telehealth.20,39 This is not unilinear yet static. Moreover, Australian CALD communities are more likely to experience language barriers, low health literacy, lack of access to technology and lack of support to use the technology at higher rates than those with Anglo-Saxon heritage, which results in additional barriers to telehealth access.19,42 These differences in telehealth access can also reinforce health and social inequities, ultimately impacting health outcomes.42–45 These dynamics and complexities allow intersectionality to be an appropriate tool for studying the digital divide in the context of Mandarin-speaking individuals accessing telehealth in metropolitan areas. Therefore, intersectionality provides a framework that describes and interprets how access to telehealth in metropolitan Queensland is shaped for Mandarin-speaking individuals requiring interpreter services. As conceptualised by Crenshaw and further developed by Collins, intersectionality's core constructs, such as relationality, power, social inequality, social context, complexity and social justice, were considered for the analysis.35,37
Researchers’ positionality
Researchers acknowledge their own positionalities and their potential implications on data interpretation. VGR is a male Spanish-speaking medical doctor immigrant to Australia who built relationships with MIS and Mandarin-speaking researchers to ensure the validity of the data. Moreover, from VGR's post-colonial heritage, there is ongoing reflexivity to avoid assumptions based on shared cultural backgrounds. To synthesise findings, VGR searched for cross-cultural methods that captured key intersecting dimensions of oppression embedded in the healthcare provision in a metropolitan hospital, including how age, language barriers, socioeconomic status, cultural factors and health conditions combined to shape participants’ experiences with telehealth and interpreter services. Key themes were mapped into elements of the intersectional framework as described by Collins 35 and validated by Mandarin-speaking researchers, balancing the need to respect individual perspectives with extracting cross-cultural insights about the interplay of telehealth offers and disadvantages from an outsider Spanish-speaking perspective.
Results
Participant characteristics
Between June 2024 and November 2024, a total of eight participants (n = 8) and their caregivers (n = 2) participated in one of three focus groups. For this research, caregivers provided support and did not participate as respondents or add to the analysed sample size. The average age of participants was 69 years (range 45–80 y). Six participants (n = 6, 75%) had a university or college education, access to the internet, and a computer or tablet device. Conversely, while participants had experience with telephone consultations, only two (25%) had experience using videoconferencing for their medical consultations. Participants used the telephone for multiple health conditions, including diabetes, cancer, autoimmune conditions and dermatology (Table 2).
Sociodemographic characteristics by participants’ gender.

*All values rounded to 1 decimal place.
Themes
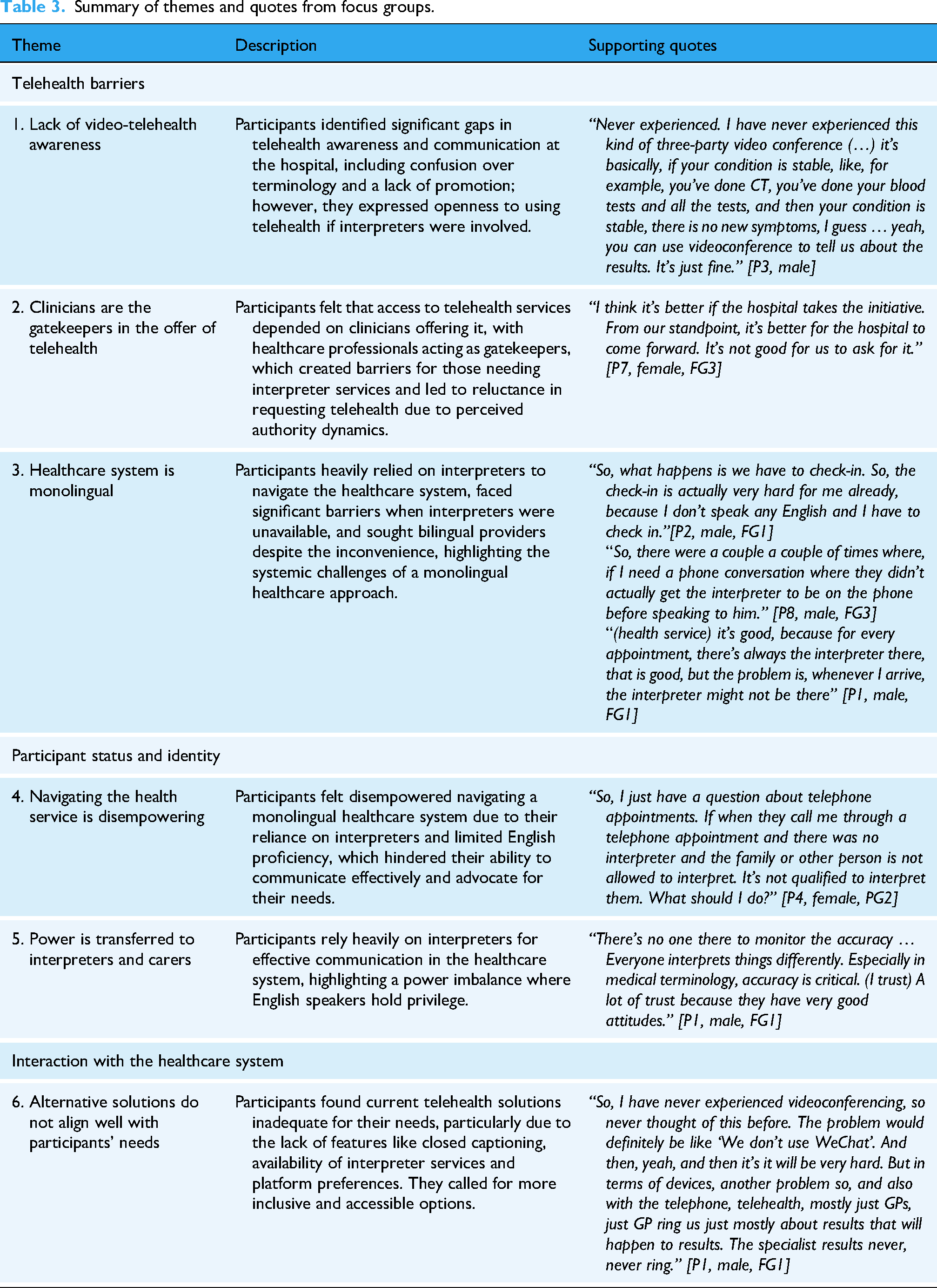
Our analysis revealed six themes describing telehealth barriers, participants’ agency and interactions with the healthcare system. A summary of the themes and supporting quotes is listed in Table 3.
Summary of themes and quotes from focus groups.
Telehealth barriers
Theme 1: Lack of video-telehealth awareness
Participants explored multiple barriers and gaps in telehealth awareness and communication across the service provision at the hospital. They noted that telehealth was primarily used via telephone and offered by their GP. Despite this, participants were unaware that telehealth was an alternative option for managing their conditions at the hospital and were often unaware that this modality had an interpreter option. Participants commented that, at the hospital, they had never been offered telehealth (see Table 3).
There is a misunderstanding in this teleconference. In my opinion, the teleconference has no interpreter: it is just like a video. That's why the people will get very confused.
[P3, male, FG1]
Subtheme 1.1: Telehealth terminology is confusing
Participants reported feeling confused about the terminology used to describe telehealth services. For participants, a ‘videoconference’ implies a conference with multiple people present during the medical appointment with minimal or no interaction with the interpreter or clinician. As perceived by participants, this modality would have made it challenging for them to engage with their service providers, especially when English is the dominant language in the hospital's service provision.
There is a distinction between conferences and consultations. Conferences will usually have one person speaking in a long segment, so we will just sit there and listen. The doctor consultation is an interactive communication. In the case of tele or video conferences specifically for Chinese people who don’t understand English, having an interpreter is a solution. [P3, male, FG1]
Subtheme 1.2: Telehealth uptake should be greater
Participants were also sceptical when asked about the current telehealth access gap among people needing interpreter services. They felt that the gap did not reflect the needs of Mandarin community members, as their peers should have widely adopted telehealth given the large number of Mandarin speakers in their community. Conversely, participants shared their knowledge of telehealth benefits, including reduced travel time and continuity of care. They expressed their willingness to use telehealth, provided that interpreters participated in the consultations with clinicians.
Since the hospital has paid the cost of interpreters, it does not matter whether it is telehealth or face-to-face, so why doesn't the hospital provide us with the same opportunity for telehealth? [P5, female, FG2]
Theme 2: Clinicians are the gatekeepers in the offer of telehealth
Participants noted that their opportunity to access telehealth services largely depended on whether healthcare professionals offered it as an option or took the initiative to offer it. The decision to provide telehealth services rests with healthcare providers, giving them significant control over consumers’ access to these services.
Subtheme 2.1: Selected consumer group may not request telehealth
In this study, Mandarin-speaking consumers relied more on clinicians to recommend telehealth rather than initiating the request themselves. They were reluctant to request telehealth, as it would go against the clinician's perceived/implied authority, and they preferred to follow the clinician's recommendation.
“I think it's better if the hospital takes the initiative. From our standpoint, it's better for the hospital to come forward. It's not good for us to ask for it.” [P7, female, FG3]
Subtheme 2.2: Age-related assumptions
As perceived by participants, a telehealth appointment offer may be less likely to occur if clinicians assume that age will limit one's ability to use the required technology. For participants, there is an assumption that age limits the use of telephone or videoconferencing. In line with this assumption, participants considered less technological modalities of care. Participants relied on the doctor's initiative, interpreter support or a carer to fulfil their telehealth appointment goals.
So, I think telehealth depends on the age. We’re getting older. We don’t have to use technology, so telehealth… ring me and tell me what you just want to say. Maybe younger people, younger, they would like to use it.” [PG3, male, FG1]
Theme 3: Healthcare system is monolingual
Participants manifested their heavy reliance on interpreters to navigate the healthcare system, especially when interacting with the clinician. However, in the absence of interpreters, communicating with the healthcare system in English became a significant barrier to accessing services.
“The interpreter is the most important thing, OK? The most important thing. Without interpreters, nothing can be done in the hospital.” [P1, male, FG1]
Subtheme 3.1: Telehealth services are typically monolingual
All aspects leading up to a telehealth appointment are monolingual, which makes it extremely difficult for a patient from a CALD background to navigate. For example, when booking or trying to book an appointment, requesting an interpreter, and navigating other steps of the service provision, including asking for additional medical support, technological assistance, and contacting their GP, participants will face monolingual obstacles to accessing telehealth. Moreover, participants reported that interpreters were not offered if they spoke basic English, often leaving them struggling to communicate effectively. Similarly, interpreters cannot communicate with participants until the day and time of the appointments, which may limit time for rapport building.
Usually, what happened is the doctor… the hospital is making the appointment over the phone, but they were not aware that I needed the interpreter. [P8, male, FG3]
“… I never get (interpreters) … when I am on the phone” [P4, female, FG2]
Subtheme 3.2: Language barriers when accessing healthcare
Lacking interpreter access during hospital check-in created a significant barrier for Mandarin-speaking consumers, who felt unprepared and lacked confidence in navigating and preparing for an appointment. This forced reliance on family members for basic access to healthcare services. While interpreters can be requested during the appointment, additional support is often required before and after the appointment (e.g., navigating directions, communicating with administrative staff, and booking follow-ups). Similarly, not being proficient in English was perceived as a barrier, further complicating access to telehealth and healthcare. This led to participants often seeking alternative options to continue their care, such as bilingual providers, even if it may involve travelling longer distances or spending more time.
“I live in the northern part of the city, where is very difficult to find a GP that speaks Mandarin. So, my GP is actually in the south of Brisbane. He speaks Mandarin and it's very easy for me to communicate with him. So, the telehealth is really good.” [P2, male, FG1]
Participants’ agency
Theme 4: Navigating the healthcare system is disempowering
Participants perceived the experience of navigating the healthcare system as disempowering, particularly in a monolingual healthcare system. As mentioned in themes 1 and 2, the Australian health system provides its services in English, which, from the participants’ perspective, is a barrier that affects their ability to access telehealth and their independence as individuals. For participants, loss of independence and agency can represent a power imbalance.
Subtheme 4.1: Agency is lost when participants are not proficient in English
Participants’ heavy reliance on an interpreter and lack of English proficiency significantly diminished their sense of agency and control over their healthcare-seeking journey. Participants expressed that without English, their ability to navigate the healthcare system was severely compromised.
“Seeing a doctor is very hard. Yeah, very hard to see a doctor. We have language problems, and when I make an appointment to see a doctor, I have another person. I need a transport to go to the hospital, and it is hard to make time to guide them.”
[P4, female, FG2]
“I also feel that if I see the doctors face to face, I can ask a lot of questions. When I’m there, I just I can and will ask more questions than when the appointment is over the phone. The phone is like I’m just listening to what the doctor says, and then it is finished. So, I don’t have a lot of chance to ask questions”[P5, female, FG2]
Subtheme 4.2: Differences in experiences across healthcare systems
Participants felt that their ability to engage in meaningful, bidirectional communication during a telehealth appointment was compromised, leaving them feeling unheard and disempowered. Consequently, participants expressed their perceived inability to communicate effectively in English, which leads to a loss of autonomy for consumers, making it difficult for them to advocate for their needs and preferences. Participants also compared the Chinese health system to the Australian system. They noted that they could always communicate effectively in the Chinese healthcare system and feel comfortable asking doctors questions. However, in the current context, due to their limited proficiency in English, they encounter significant barriers and confusion when trying to communicate with healthcare providers via telehealth. Similarly, participants expressed their fear of missing telehealth phone calls and having reduced agency to ask questions freely over telehealth, given the uncertainty of the interpreter's availability. For participants, anxiety emerged from not being able to establish bidirectional communications, considering their health could be endangered.
“Telehealth is a very good method, but there's one thing with the telephone appointment. I receive a lot of scam calls on my phone every day. When the doctor calls, even if it happens to be a private number, I will think that is a scam call and most likely reject the phone call or even block this phone call.”[P4, female, PG2]
Theme 5: Power is transferred to interpreters and carers
Participants emphasised their profound reliance on interpreters to navigate the healthcare system. Interpreters are considered to be key personnel to help participants navigate a monolingual healthcare system. Despite interpreters not being present at all stages of the service provision or having established previous communication with consumers, participants expressed mixed feelings about interacting with interpreters.
Subtheme 5.1: Reliance on carers and interpreters to make telehealth work
This reliance is not just a preference but a necessity, as they have no choice but to depend on interpreters for effective communication and understanding the healthcare offer.
“Telehealth must have an interpreter. Videoconferences must have an interpreter's presence. Otherwise, this won’t work.” [P1, male, FG1]
“They call me through a telephone appointment, and there was no interpreter, and the family or other person is not allowed to interpret. What should I do?”
[P4, female, FG2]
Subtheme 5.2: Trusting the accuracy of medical interpreting
In a monolingual service provision, there is an implicit expectation that the accuracy of the translation meets participants’ needs and is to a high medical standard. From this perspective, participants feel that their cultural and language needs are acknowledged and respected. Unlike with health professionals, trust emerges from the power transferred to interpreters and their ability to understand participants’ needs.
“There's no one there to monitor the accuracy … Everyone interprets things differently. Especially in medical terminology, accuracy is critical. I trust interpreters because they have very good attitudes.” [P1, male, FG1]
Interactions with the healthcare system
Theme 6: Alternative solutions do not align well with participants’ needs
Participants expressed that current alternative solutions for telehealth do not effectively integrate with their needs, particularly when it comes to videoconferencing. For example, simple additions like closed captioning could significantly improve their experience but are not being utilised or offered. Also, restrictions in choice of videoconferencing (provider preferred) platforms could also limit access to telehealth.
“So, I have never experienced videoconferencing, so I never thought of this before. The problem would definitely be like ‘We (the hospital) don’t use WeChat’. And then, yeah, it will be very hard. Another problem with the telephone, telehealth, mostly just GPs ring us mostly about results. The specialist results never, never ring.” [P1, male, FG1]
Subtheme 6.1: Willingness to try other virtual care modalities
Participants are open to innovative solutions and call for telehealth options to be promoted among Mandarin speakers and clinicians at the hospital. However, participants mentioned that using an interpreter on demand via telephone is unavailable during videoconferencing telehealth sessions, limiting their ability to communicate effectively when videoconferencing issues arise. Ideally, when using videoconferencing, participants would expect a user-friendly platform with minimal technical issues and opportunities to access technological support; if not, it would reduce confidence and desire to use videoconferencing. On the other hand, an equitable telehealth offer would significantly contribute to their health-related cost and time, particularly when considering travel costs and parking difficulties.
“Now we should experiment with tele-consultation, and then we will know more about it. It's easy to ask for a consultation by phone now (after the focus group), but no consultation via WeChat or computer yet. Specialists have never had one tele-consultation.” [P1, male, FG1]
Subtheme 6.2: No one to contact when patients feel lost or unsure
Increasing the likelihood of a telehealth service being made available would require additional input from the health system, which must be clear and bidirectional at the starting point. As such, participants requested a dedicated contact person for technical issues, the need for post-consultation support mechanisms – such as administrative and technical - and infrastructure for interpreter services in telehealth.
“I think having a phone call is better. Use the phone to notify the time of the teleconsultation and what you need to prepare, for example, laboratory tests. Then, just start on time with an interpreter in place.” [P3, male, FG]
Subtheme 6.3: Security concerns
According to the participants, trust and security concerns are shaped by cultural experiences and previous experiences with scam callers. In this sense, communication infrastructure gaps, including calling from private numbers, poor hospital internet and lack of callback options, are perceived as barriers for Mandarin-speaking consumers. Participants shared their preference for using telehealth platforms or technologies that are familiar to them and can link them with the health system easily.
I can’t call back to the hospital or go somewhere. I just…. I’m guessing. I tried to find the call, sometimes take a long time to find out who called me. [P4, female, PG2]
Discussion
Our study used a cross-cultural, cross-lingual intersectional approach to examine the experiences of Mandarin-speaking participants who require interpreter services when accessing telehealth in a tertiary hospital in metropolitan Queensland, Australia. This study has shown that Mandarin-speaking participants face significant challenges accessing the current telehealth service, particularly video consultations. We found that the key barriers to accessing telehealth are the monolingual healthcare offered and the clinicians’ assumptions about participants’ abilities to use telehealth. More broadly, our participants described a reliance on interpreters and carers to communicate on their behalf, transferring privilege to English-speaking voices. This transfer risks causing disadvantage and oppression for Mandarin-speaking participants. However, while alternative technological solutions are proposed, such as videoconferencing interpreters, participants claim that more straightforward and safe communication strategies are needed to engage with their healthcare provision.
In the Australian healthcare access context, the ability to speak English fluently can reflect a position of privilege and power. Describing language barriers is not new to healthcare provision. 1 However, by using an intersectional approach, our study highlights the inconsistency of healthcare provision in a tertiary hospital in a metropolitan area when interpreters are required. This enables English-speaking health consumers to make and negotiate decisions about a Mandarin-speaking participant's health through efficient communication and navigation in the health system. However, while ageism can interplay in this dynamic, this is not the first study reporting Chinese Australians’ inequitable participation in other healthcare provision forms. For example, Yu et al. 22 described English as a leading factor preventing Chinese Australian carers of people living with dementia from participating in dementia carer interventions. As such, interactive Mandarin-based telehealth offers could significantly improve carers’ participation by motivating them to improve health literacy more effectively. 22 Similarly, our work contributes to the academic evidence supporting interventions incorporating bilingual options across the service provision, such as interpreters, digital health navigators 10 or bilingual health professionals to promote equitable access to telehealth.
Participants shared their willingness to access and benefit from telehealth. A limiting factor was reported to be the healthcare provider perceived bias in offering telehealth. Husain et al. 15 described the potential normalised discrimination in the digital health service offering. For Husain et al. 15 language barriers often intersect with the perception of racial discrimination, reducing engagement with other telehealth offers. As such, Roy et al. add the need for cultural appropriateness in the healthcare service provision, given the reports of discrimination in the intersection with low social support or limited English proficiency among South Asian immigrants in the US. 46 However, our previous work 9 suggests that despite the low offer of telehealth, acceptability and trust in telehealth among people needing interpreter services do not differ from those who do not require interpreters, particularly when medical doctors are the leading healthcare providers. Notwithstanding, despite its availability, Tang et al. found a reduced use of videoconferencing interpretation. 6 However, clinicians doubted that this strategy was effective and could communicate efficiently, which might have added to existing barriers. 6 Across our work, participants described the lack of opportunities for Mandarin speakers to engage in telehealth services requiring interpreter services in a metropolitan setting. While a form of discrimination from health professionals may be implied, there is also evidence of a reduced likelihood of being offered telehealth if a participant did not speak English as a first language.21,33 Further research should examine clinicians’ perspectives using mixed-method or qualitative emancipatory approaches to unveil this exclusion phenomenon. Similarly, from a health system perspective, a multicultural healthcare delivery option, considering video telehealth, could reduce some barriers for CALD communities.16–18,47
Multifaceted interventions that address intersecting elements of the health system, such as administrative processes, interaction with healthcare providers and education, appear to improve the uptake of interpreter services, overcome language barriers and ultimately optimise access to healthcare.1,15,26 However, Troung et al., 28 in a review of multiple interventions addressing these barriers, found that culturally appropriate interventions and inclusion of multicultural consumers’ perspectives are commonly absent. As such, real-life consumer experiences informed our research, and the findings can support the direct transfer of knowledge from consumers to researchers, implementers, and healthcare professionals, aiming to improve access to telehealth and overcome the digital divide. Guided by cross-cultural research, we ensured that the voices of our participants were accurately represented by using real-time interpreters during our focus groups, incorporating Mandarin-speaking researchers, and verifying the accuracy of the translation before analysis with a certified translator. The results of our study highlight the importance of consumer involvement, bidirectional communication strategies between hospital and consumer (appointment scheduling and options), and cultural competence training for clinicians. Nevertheless, multiple strategies have been proposed to overcome these barriers and improve equity of access to care. Strategies include improving telehealth infrastructure,44,48,49 integrating cultural competence into healthcare,20,50 and promoting digital health literacy among consumers and providers.20,48 Crenshaw 37 and Husain et al. 39 argue that societal differences and their consequences have yet to be fully addressed. A broader understanding of multiple layers of inequities needs to be envisioned and translated into pluricategorical solutions to stop widening injustice.35,39 However, consumer perspectives have yet to be incorporated to accurately identify gaps in service provision and optimise the effectiveness of the proposed strategies.2,44 This will facilitate designing and implementing culturally competent telehealth interventions to improve equitable access.43,44,51 Similarly, this piece of work highlights the need to increase interpreter uptake among clinicians and delivery of health services to accommodate language diversity. Further research could explore the challenges of interpreter uptake for telehealth appointments among clinicians.
Limitations
This study has limitations worth acknowledging. We recruited elderly populations from a tertiary hospital in metropolitan Queensland. Our results may represent the experiences of participants with more complex needs than those requiring interpreter services in primary care settings. Similarly, given the firm establishment of the Chinese Australian community in metropolitan Queensland, personal and social agencies outside the hospital system might have influenced the ability to access technology and engage with their care. These characteristics differ from those of other CALD communities, in which social agency is severely affected by discrimination or low socioeconomic status.52,53 Similarly, our study recruited a small sample. These demographic characteristics might limit individual and geographical diversity and the degree of access to technology. Moreover, the study's dependence on participants’ interpretations of their experiences expressed in Mandarin and then translated into English could affect the comprehensiveness and variety of the insights obtained. However, we consulted cross-cultural methodological references, double-checked translations, and engaged in critical reflexivity to represent the experience shared accurately and translate these learnings into tangible solutions promoting equitable access to telehealth. Our efforts to ensure rigour in the methods were informed by Quintanilla et al. 34 and their work exploring maternal health in a diverse group of women living in Canada. While this provided strong methodological foundations for conducting cross-lingual focus groups, 34 our analysis responded to the need for a diverse and intersectional understanding 39 of the complexities of the digital divide and access to telehealth among communities living in metropolitan Australia.
Strengths and implications
To our knowledge, this is the first cross-cultural, cross-lingual focus group exploring telehealth access among culturally and linguistically diverse (CALD) communities living in Australia from the participant perspective, in their preferred language, using an intersectional lens. Given the limited methodological foundation for cross-cultural, cross-lingual focus groups exploring the multicultural digital divide, our study describes a fundamental patient-centred approach to guide similar multicultural research around the globe. Our findings can inform future actions aimed at narrowing the healthcare equity gap. As such, this study highlights and corroborates several actionable insights13,20 that support targeted implementation actions for multiple stakeholders.
For health providers and clinicians, culturally responsive care, including training in cultural competence, offers an opportunity to better understand the intersectional barriers faced by CALD communities, including language barriers, trust concerns, and digital literacy. Similarly, seamless integration of interpreter services embedded into telehealth workflows, with clear protocols for scheduling and communication, would avoid delays and miscommunication. Moreover, clinicians should adopt flexible communication strategies that accommodate diverse cultural structures and caregiving roles, particularly in CALD communities facing intersectional inequities in accessing healthcare, including age, gender, disability, and ethnicity.
For administrative staff and health systems, co-creating telehealth services with CALD communities can help ensure that technology, platforms and processes are culturally appropriate and responsive to user needs. As such, health services can explore telehealth platforms that support multilingual access and interpreter integration. Technical support should be available in multiple languages to assist with language needs. Additionally, given the maturity in exploring the cultural digital divide in Australia, systems should routinely collect data on cultural needs, language needs, and interpreter use to monitor equity in telehealth access and outcomes.
For policymakers, clear national definitions of CALD and consistent reporting standards are needed to guide equitable service planning and evaluation. As telehealth transitions from emergency response to long-term service delivery, policies must ensure that CALD communities are not left behind in digital health transformation.
Our work serves as foundational research for further exploration of the digital divide across multicultural societies. Given the limitations of sample size and single-site recruitment, future research should aim to conduct larger, multi-site studies that include a broader range of CALD populations and language groups. Comparative studies across regions and service types would help identify context-specific barriers and facilitators. We call for more multi-stakeholder co-designed interventions embedded in emancipatory approaches that acknowledge the need for patient-centred approaches in the evolving language and cultural diversity of the healthcare provision. Longitudinal research could explore how telehealth access and engagement evolve, particularly as telehealth systems mature post-COVID.
Conclusion
Mandarin speakers requiring interpreters face significant challenges in engaging with telehealth services, particularly videoconferencing in metropolitan Queensland. The barriers identified using a cross-cultural, cross-lingual intersectional approach include the predominantly monolingual nature of healthcare services and clinicians’ assumptions about participants’ proficiency with telehealth technologies. These barriers not only undermine the social agency of Mandarin-speaking consumers but also perpetuate their disadvantage and oppression while privileging English-speaking individuals. Although alternative technological solutions have been proposed, such as video-based interpreter services, participants advocate for more straightforward and secure communication strategies that facilitate their engagement with healthcare services.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261415915 - Supplemental material for Understanding the telehealth access through an intersectional lens: Experience of Mandarin-speaking consumers accessing health services from a tertiary hospital in Australia
Supplemental material, sj-docx-1-dhj-10.1177_20552076261415915 for Understanding the telehealth access through an intersectional lens: Experience of Mandarin-speaking consumers accessing health services from a tertiary hospital in Australia by Victor M. Gallegos-Rejas, Jaimon T. Kelly, Ling Zhang, Nicole Marinucci, Karen Payne, Xiaoyun Zhou, Yiran Lu, Anthony C. Smith and Emma E. Thomas in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261415915 - Supplemental material for Understanding the telehealth access through an intersectional lens: Experience of Mandarin-speaking consumers accessing health services from a tertiary hospital in Australia
Supplemental material, sj-docx-2-dhj-10.1177_20552076261415915 for Understanding the telehealth access through an intersectional lens: Experience of Mandarin-speaking consumers accessing health services from a tertiary hospital in Australia by Victor M. Gallegos-Rejas, Jaimon T. Kelly, Ling Zhang, Nicole Marinucci, Karen Payne, Xiaoyun Zhou, Yiran Lu, Anthony C. Smith and Emma E. Thomas in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank Ms Jannie Liao and Ms Xiaomei Liu from Metro South Interpreter Services for their support during the recruitment process. Additionally, we would like to thank our participants for sharing their experiences with us.
Ethics approval
The Metro South Research Ethics Committee approved the study (HREC/2023/QMS/95080).
Author's contributions (CRediT roles)
Conceptualisation (VG, ET); Data curation (VG, ET, JK, LZ, XZ, YL); Formal Analysis (VG, ET, JK, LZ); Funding acquisition (VG, ET, JK, AS); Investigation (VG, ET, JK, KP); Methodology (VG, ET, JK); Project Administration (VG, JK, KP, NM); Resources (VG, KP, ET, NM, JK); Supervision (ET, JK, AS); Validation (LZ, XZ, YL); Writing original draft (VG); Reviewing and Editing (All authors)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
The data that support the findings of this study are available from the corresponding author, VG, upon reasonable request.
Code availability
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.