
Abstract
Objective
We present qualitative findings from interviews with frontline clinicians and service users of a fetal telemedicine service.
Methods
Semi-structured interviews with clinical stakeholders and service users were conducted, undertaken as part of a service evaluation. Data collection was undertaken by different teams, using interview schedules aligned to independent evaluation aims. Data were subjected to thematic analysis.
Results
Sonographers reported four main challenges: delivering a shared consultation; the requirement to resist scanning intuitively; communications during the scan; and restricted room space. Notwithstanding, all clinicians reported that participating women were accepting of the technology. Service users reported few concerns. The main benefits of fetal telemedicine were identified as upskilled staff, increased access to specialist support and improved management of complex pregnancies. Convenience was identified as the main benefit by service users, including savings in time and money from not having to travel, take time off work, and arrange childcare.
Conclusions
Service users and clinical stakeholders were accepting of the service. Service users reported satisfaction with communications during the consultation and awareness that telemedicine had facilitated local access to clinical expertise. Whilst clinical stakeholders reported challenges, the iterative nature of the evaluation meant that concerns were discussed, responded to, and overcome as the pilot developed. Clinical stakeholders’ perception of benefits for service users encouraged their acceptance. Moreover, the evaluation established that fetal ultrasound telemedicine is a viable method to access expertise safely and remotely. It provided demonstrable evidence of a potential solution to some of the healthcare challenges facing rural hospitals.
Keywords
Introduction
Ultrasound fetal screening is central to antenatal care; when fetal problems are detected pregnant women may be referred to a fetal medicine (FM) Specialist. However, the complexity of FM referrals that can be managed in a District General Hospital (DGH) is dependent on the availability of obstetric ultrasound expertise. In the absence of ‘expertise’, or in cases with complex anomalies, women are referred to a specialised Fetal Medicine Centre (FMC). For women living in remote areas, referral can mean hours of travel at their own expense. Moreover, it has been shown that distance between home address and referral centre has a negative effect on attendance and rates of prenatal diagnosis. 1
The use of telemedicine to provide fetal diagnostic services has widening global appeal. It has been shown that high-quality, real-time, ultrasound images can be effectively transferred via videoconferencing.2–4 Previous studies have confirmed images of sufficient standard.5,6 Further, tele-ultrasonography has been shown to improve clinical accuracy and detection in congenital heart disease;7,8 increase consultation rates and improve access to specialist support;5,9,10 and enable more consultations to be carried out with significant cost savings.11,12 Prenatal management using telemedicine can also produce considerable savings for service users in time and money; studies have reported high levels of satisfaction and reductions in travel time and time off work.11,13,14
Telemedicine also has the potential to upskill DGH staff and has facilitated the education of clinicians in screening methods.10,15 For example, Hishanti et al. found increased skills in staff and improved screening. 15 Telemedicine enabled staff to consult with specialists on subtle anomalies, and this led to better identification of abnormalities and resulted in increased referrals. 15
A ‘Fetal Ultrasound Telemedicine’ pilot, funded by the Academic Health Science Network North East and North Cumbria (AHSN NENC), commenced in October 2015. The primary objective was to initiate a service between the obstetric ultrasound unit of a remote/rural DGH (a subsidiary of Trust1) and the FMC of a major teaching hospital (Trust2), both in northern England. A videoconferencing link was established which enabled a FM Specialist to remotely, and synchronously, examine ultrasound images captured by trained Sonographers at the DGH, and to conduct remote consultations with the women being scanned. A standard FM consultation is made up of a series of tasks/activities undertaken by different staff; fetal telemedicine involves a relocation of some of those tasks/activities. In either scenario, the contribution of a FM Specialist remains the same. Table 1 illustrates the prevailing and telemedicine pathways.
Fetal medicine pathways.

By opening up access to expertise at a distance, the pilot intervention aimed to improve fetal ultrasound services at the DGH and to reduce travelling time and expense for referred women. The DGH faced several challenges, staff recruitment being high amongst these. Both service managers and senior executives reported difficulties in recruiting to clinical roles. In particular, skilled Sonographers are difficult to recruit, either for locum or permanent posts. The DGH had a consultant-led maternity unit but not a FM Specialist, and so the detection of a fetal problem resulted in referral to the FMC for specialist, outpatient consultation. The DGH also served some disadvantaged communities. 16 In this respect, attendance at the FMC could be challenging due to distance (94 miles between sites) and road quality. The journey by car takes approximately 2 hours and 20 minutes, each way. Parking at Trust2 is limited and costly. Train journeys between the two sites take between 3 and 3.5 hours, followed by a 1-mile walk or taxi journey. An appointment therefore needs to be allocated a full day, often by both the woman attending and a partner, family member or friend.
In this paper, we present findings from qualitative interviews with clinicians and service users undertaken as part of the evaluation of the pilot intervention. We examined the perspectives of frontline clinicians because a lack of staff acceptance is identified as a key barrier to adoption of digital health innovations.17–20 The clinical stakeholder study aimed to identify the barriers and enablers of adoption of telemedicine. We explored clinicians’ initial thoughts about fetal telemedicine; their experiences of undertaking consultations in this way; the impacts of fetal telemedicine on job role, service users and organisation; and their view of benefits and their concerns. We considered clinical stakeholders’ perceptions of the experiences of the service users because women’s dissatisfaction with the service would undermine the value of benefits accrued. The service user study aimed to directly assess women’s experiences and acceptance of fetal telemedicine. We explored their initial reactions to the idea of fetal telemedicine; their experiences during the telemedicine consultation; whether there were any associated problems or concerns; and the benefits.
The paper will highlight the challenges faced by both Sonographers and service users and show how these were negotiated. In so doing we show that their attitudes towards and perceptions of telemedicine are the result of a balancing process between advantages and disadvantages.
Methods
Collaborative evaluation
Evaluation of the pilot intervention involved collaboration between two NHS Trusts and two universities. Ethical approval was granted for the evaluation of the service (NRES Committee London – Hampstead REC reference: 14/LO/1671). The evaluation was divided into three parts and undertaken by different collaborators (Table 2).
Evaluation of the pilot intervention.

Timescale
The fetal ultrasound telemedicine pilot was conducted over 12 months from October 2015, during which time 82 consultations were undertaken; studies 1 and 2a continued throughout. Service user interviews for study 2b were conducted between November 2015 and July 2016. Interviews with clinical stakeholders for study 3 took place between November 2015 and February 2016.
Findings from the three studies were fed back iteratively during the pilot phase to enable adaptation. At the end of the pilot phase, internal reports were presented to funders and managers in order to support adoption of the service. Findings from study 2b and study 3 are presented here.
Qualitative data collection
Qualitative data were collected via semi-structured interviews. This method was chosen to facilitate in-depth, guided yet open, two-way discussions wherein interviewees were able to introduce evidence they perceived to be important. Data collection was undertaken by different teams, using interview schedules that were aligned to independent evaluation aims. Data collected in both studies were subjected to thematic analysis. 21
Consent
All interviewees gave their informed consent prior to interview. Interviewees were given an information sheet explaining the project and how the data collected would be used, and were given the opportunity to ask questions. In face-to-face interviews participants signed consent forms; in telephone interviews consent was gained verbally and digitally recorded before interview.
Service user interviews
From questionnaire returns (study 2a), a subsample of service users (n=16) were invited to participate in a telephone interview; the questionnaire included a ‘permission to contact’ form by which women volunteered to be interviewed. Purposive sampling was used to identify participants to achieve maximum variation (Table 3). Telephone interviews (average 10 minutes) were conducted by ML, recorded, transcribed, cleaned and anonymised before being entered into Atlas.ti qualitative data management software for indexing and retrieval. Thematic analysis was undertaken; codes were agreed following independent coding of three interview transcripts by ML and VS. Themes were mostly developed from the interview guide (Appendix 1) which was based on the literature. However, women were able to expand on their answers from which emergent themes were developed. ML (a qualitative health researcher with 20 years’ experience) coded the remaining interviews using the agreed coding frame.
Sampling for service user interviews.

Clinical stakeholder interviews
Semi-structured interviews (average 40 minutes) were undertaken with seven clinical stakeholders by EB: two DGH radiology managers; a DGH Obstetrician; a FMC FM Specialist; two DGH Sonographers; and one FMC Midwife Sonographer, who coordinated the pilot. One interview (Obstetrician) was completed by telephone and the remaining were conducted face to face. AM (over 20 years’ experience in stakeholder engagement) and EB (over 20 years’ experience in social research) are experienced in conducting evaluations of digital health interventions; they employed an established interview schedule which was refined following meetings with commissioners and managers (Appendix 2). Interviews were recorded, fully transcribed and anonymised, and entered into NVIVO (qualitative data analysis software). Data were subjected to thematic analysis by EB. The interview questions structured the initial coding frame; sub-themes were added as they emerged during analysis; codes were reviewed and agreed by AM.
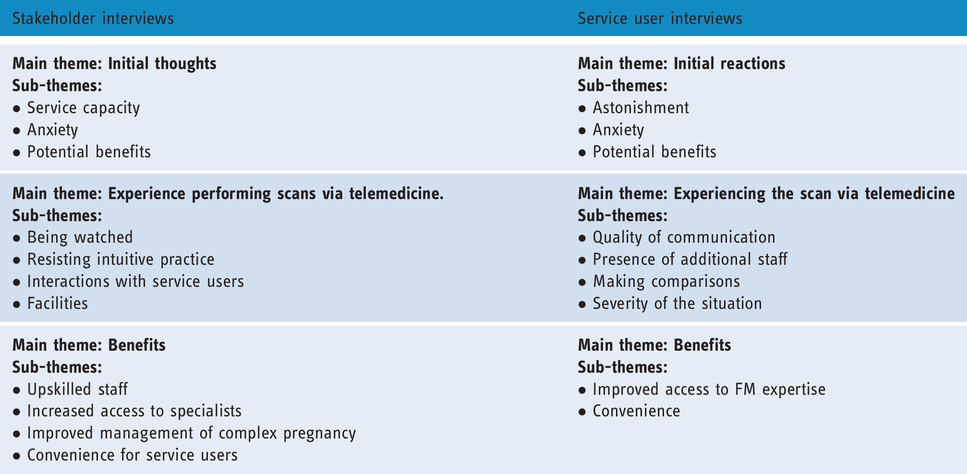
Although data collection was undertaken separately, there was significant crossover of topics between the clinician and service user interviews, and thematic analysis of transcripts engendered similar themes (Table 4).
Thematic coding: main themes and sub-themes.
Findings
Initial thoughts
Service users and clinical stakeholders were asked to recall their initial thoughts about fetal telemedicine; most were generally positive, but concerns were also expressed.
Clinical stakeholders
Service managers at Trust1 reported being supportive of the pilot but had worries about service capacity; they reported major difficulty in recruitment to clinical roles within this rural area. Staff capacity in obstetric ultrasound was especially problematic due to vacancies and maternity leave. Further, the telemedicine service would create additional work for DGH Sonographers. Although the pilot included ‘back-fill’ funding for sonography time, this was difficult to utilise due to the difficulties described above. Thus: I thought it was a very good study to undertake but my first thought … was how on earth we were going to find the capacity in a greatly over stretched service to be able to support the additional workload (DGHMan1).
Sonographers reported having mixed feelings about the pilot. They were concerned about whether the link would work, whether they could perform the ultrasound examinations as required, and whether service users would accept it: I sort of thought it won’t happen, it’ll never happen, you know, the link won’t work, or something like that. And the more that it got, that it is going to happen then it’s will the patients like it? What will we be like? Will we be able to do it? (DGHSon2)
Despite their anxieties, Sonographers recognised potential benefits for service users: ‘I think that’s the biggest thing as far as our ladies are concerned, it’s that they’re not travelling, they’re still getting the same service but they’re not travelling’ (DGHSon2).
Service users
Women participating in the pilot were also asked about their initial feelings. Some expressed astonishment: ‘it was a surprise. I didn’t realise they had that facility, but I thought that was a great idea’ (Int7); ‘I was quite interested about it to be honest because I’d never heard of it before’ (Int15).
Women also expressed anxiety, because they were unsure of what would happen at the consultation and what the outcome might be: ‘I was a little bit anxious about how it was going to happen because obviously we were completely clueless until we got in the room’ (Int11). Furthermore, it was apparent that anxiety felt in relation to the need for a specialist scan influenced women’s initial feelings towards telemedicine: ‘you’d be silly not to feel a little anxious as to what they’re going to find’ (Int9); ‘I was more frightened in case, the results … I think it frightened me more because it was somebody from [the FMC] that was going to do it’ (Int14). There was, therefore, an element of ‘weighing-up’ by the women: ‘I was fine … I knew it was a good thing as long as we found out whether the baby was healthy or not’ (Int10); ‘medically, … I was a little worried as to why I would need it but … nothing to do with the telemed’ (Int9).
However, this must be set in context with anxiety they may have felt over a conventional referral, or indeed any new medical procedure. One service user (Int11) expressed relief at not having to undertake the journey: ‘it would have been like a four-hour round trip’. Another summed up the benefits: ‘I think it will save a lot of people a lot of stress, anxiety, money, time and everything else for something that you know is relatively quite simple’ (Int1).
Experiencing fetal telemedicine
Sonographers reported four main challenges from telemedicine: delivering a shared consultation when one is used to working alone; the requirement to resist scanning intuitively; communications during the scan; and restricted room space. Notwithstanding, all clinicians reported that participating women were accepting of the technology; only one woman had been dissatisfied with the consultation. The women interviewed commented upon the experience, but few concerns were reported.
Clinical stakeholders
Being watched. Sonographers expressed anxiety about being watched by the FM Specialist when undertaking ultrasound scans. Being observed in practice is an unusual experience for Sonographers as they usually work independently with high levels of professional autonomy. Telemedicine required Sonographers to perform scans under the direction of the FM Specialist; the FM Specialist oversaw the consultation and determined how the scan would proceed. In this respect, ‘To have someone not only watching you scan but telling you how to do it is a huge challenge for anybody’ (FMCMid/Son). Anxiety was heightened due to the perceived status of the person doing the ‘watching’; having a FM Specialist survey one’s practice was particularly challenging: It’s being watched when I’m not used to having anyone in around me, or not somebody in around me that’s maybe above me, professionally. I mean I’m used to working in a room with another Sonographer but we’re at the same level. But somebody that’s actually way above me looking down at what I’m doing, that takes a bit of getting used to. His level of expertise is far greater than mine so having him watch what I’m doing; it is a bit off-putting (DGHSon1). If I was doing a twenty-week scan and I got the face, but I couldn’t quite get the top lip, I’d go off, look at the heart, look at something else, come back to it. Still can’t get it, go off and do something else (DGHSon2). DGHSon1: I do feel quite stressed … when I can’t get what I’m asked to get. I know I can get it routinely when I’m sitting on my own but I just think the added pressure of having somebody watching you do it, it just makes it more stressful and I’ve done a couple where I’ve felt a bit incompetent. Interviewer: Incompetent in whose eyes? DGHSon1: In their eyes because I wasn’t getting what was needed. I just felt I was going right back to the beginning again and I’ve been qualified for quite a bit of time. DGHSon1: Sometimes we’re doing what we think we should be doing to get what we need before they’re actually asking us to do it, and we’re already at the point where they wanted us to be… Interviewer: So you’re having to stop behaving intuitively? DGHSon1: Yeah, that’s it, yeah.
Communications with service users. Sonographers also reported that communications with service users were interrupted by telemedicine; the requirement to listen to instructions was said to hinder engagement: I just feel I’m not communicating as much with the patient during these … I feel I can’t talk because I might not hear what he’s asking me to do … and so in that respect I think it’s maybe a little bit detrimental to the Sonographer–patient relationship (DGHSon1).
Sonographers explained how they tried to organise the room to facilitate discussions between the women and the FM Specialist, but they believed this to be unsatisfactory. Sonographers were concerned that the arrangements appeared unprofessional: ‘having to move the bed around to put chairs in; it doesn’t look very professional’ (DGHSon1).
Service users
Quality of communication. Service users were asked about the quality of communications during the telemedicine consultation. The majority described the visual and sound quality as being very good, including the streaming: ‘it was really clear, the sound quality was really good … there was no buffering, there was no ducking in and out, it was just constant’ (Int16). Nor did service users report problems in communicating with the FM consultant; for example: You don’t feel stuck for who to look at … when you are sitting on a chair they are making as near to eye contact as they can do when they’re looking into a machine erm, but at other times you know they might be looking down at their paper or looking at the screen and just looking at what’s on there so you are just kind of sharing a view really (Int7). I can’t possibly ever say that I’ve had … my internals sort of broadcast to somebody in a different county do you know? … it was kind of like well we’ve literally just driven down the road to a normal hospital and had a consultation with somebody over the other side of the country (Int12). When you go for your routine check, they’ll say oh this is the baby’s head, this is this, this is that, whereas it’s just all very silent. All you can hear is [FM Specialist] telling the Sonographer what to do and you are just lying there really quiet, thinking ‘oh, I hope everything’s okay’ (Int9). There wasn’t any … tension between the team members you know. They were all working together on it and erm, it was a nice atmosphere. […] You could hear them discussing it and conferring with each other about different things or double-checking things or adjusting things on the screen … or making suggestions on how to get a better image and things like that you know? I did think it was very valuable actually as a way of, kind of sharing the expertise (Int7). They’ve done very well with the facilities that they’ve got at [DGH] but all the space really is given to the patient. … so you know, they could do with a bigger room really or one that’s been sort of planned for the purpose (Int7). I suppose it’s a little more intense when you’ve got more people in the room and more people watching you … the staff at [DGH] are really good and you know you’ve got their support … for me there’s just a lot more people and it’s like all eyes are on you and it is … quite an anxious and worrying time … sometimes it’s easier to have bad news or not so good news when you haven’t got lots of eyes on you (Int9). I think he was on a children’s ward, ‘cause I could hear the children running about and stuff (Int15). I would hear all sorts of things sort of in the background … you do have even more people than usual as part of the process, because you’ve got two sets of people looking at the same scan and I suppose part of it is you’re not sure with the camera, how much you’re being viewed or how much it’s the screen really and mostly it’s just the screen that they’re viewing (Int7).
Severity of the situation. The project team were cognisant that a serious diagnosis might impact negatively upon women’s feelings about telemedicine. Two of the women interviewed received a diagnosis of a serious fetal abnormality and reported it did not make them feel ‘uncomfortable’ (Int15) or ‘[make] a difference’ (Int8); the latter identified support at the DGH as important. Other women reflected upon how a serious diagnosis might have affected their attitude towards telemedicine; there were contrasting responses. Some did not believe a serious diagnosis would have changed their opinion: ‘I wouldn’t have felt any different to what I would have if someone was standing telling me’ (Int14). One service user reasoned telemedicine was valuable in determining any serious anomalies as soon as possible: ‘I think I’d rather have known there and then’ (Int12).
The benefits of telemedicine
The main benefits of fetal telemedicine to the DGH were identified as upskilled staff, increased access to specialist support and improved management of complex pregnancies. Convenience was identified as the main benefit for service users.
Clinical stakeholders
Upskilled staff. All clinical contributors, including Sonographers, reported that Sonographers based in the DGH had been upskilled. Preparatory training enabled Sonographers to undertake advanced techniques (uterine artery and middle cerebral artery Doppler assessment) and to better interpret images; this had resulted in an improved standard of care being delivered locally. Sonographers also reported being better informed as a result of being involved in the telemedicine consultation and they valued the opportunity to ask questions of specialists: The fact that the link is there you can talk directly to [specialists] about other service users. Just little worries … that you’ve no idea what it is; it’s worth saying can you just cast your eye over these pictures? Do we need to send this patient or scan this patient over telemed? (DGHSon2). I’ve learned about the topic yes, because when we have discussions … we can discuss why x, y, z was said, or raise concerns. We’ve recently had two ladies … and both babies eventually died, stillbirth, so you can say ‘should we maybe have done x, y, z’ and [the answer is] ‘no, no, no, that’s just the way it is’. It doesn’t make it any easier but you’re learning medically (DGHObs1). Because of the travel distance there were a number of … patients who although they should have gone to [FMC] for extra scanning would not do it … because some patients aren’t … financially or emotionally, [or] socially motivated to go (DGHObs1). It’s very much facilitating them keeping their patients but getting advice that it’s the right thing to do and not feeling threatened by asking questions (FMCon1). I think the impact on the patients here is that two hundred and odd mile journey. The petrol, a lot of them just can’t afford it, we’re not in a wealthy area, we’re in a really poor social area. So if they can come to [DGH]; have their scan and as long as they feel that their service has been done well and that they’ve had as good a scan as they could get at [FMC] well then it’s worth it (DGHSon2).
Service users
Improved access to expertise. Several women recognised the benefits of increased access to specialist input ‘for no more than a normal trip to the hospital’ (Int12): The expertise is there because the doctor’s there on screen. You can ask a question without having to think well is he going to be able to answer this, is he not going to be able to answer it … You know the right professional’s there (Int4). …you are speaking to the best person that you can really. I wouldn’t have got a consultant like that at the hospital I go to (Int11). I didn’t need to get the whole day off work, although I would have probably got paid for it, my husband wouldn’t have, if he had come with me … Obviously you save on fuel costs and, it might have been an option to get a hotel if my appointment had been at the same time [and] depending on how I was feeling because obviously I am quite late on in pregnancy; I was 35 weeks when I got the first telemed so it’s obviously not comfortable to sit in a car for two and a half hours (Int8). It would be three or more hours over there. You’d have to … park then you’ve got to get in, then you wait for your appointment and, obviously I know things over run for people, and you know you are sat there, and then you get scanned and then … you’ve got to speak to people again. They might want to see you again for something else. Then you are back, and you are doing it all in reverse aren’t you? So it’s, … literally, we would have to write a whole day off (Int12).
Discussion
The findings from this evaluation of a new fetal ultrasound telemedicine service highlight different issues for the different stakeholder groups. The iterative nature of the evaluation meant that concerns were discussed as the pilot was developed and the different stakeholder groups were made aware of each other’s points of view. Many barriers were overcome in real time.
The views of service users are perhaps the most straightforward. From their perspective the fetal telemedicine consultation was a single event, a transaction, and the relative benefits could be evaluated in this context. Service users did not have previous experience of any FM consultation, over a telemedicine link or face to face, so had nothing to directly compare it with. On the whole, responses were positive; the women interviewed reported satisfaction with communications during the consultation and demonstrated awareness that telemedicine had facilitated local access to clinical expertise. Such satisfaction has been reported in other studies. For example, Sabesan et al., in their study of teleoncology in an under-served community, found high satisfaction scores; service users were initially apprehensive but reported being able to relate to specialists via video and being highly satisfied with the consultation, often to their surprise. 22 Jacobs et al. on teleradiology argued that service users in under-served communities are pragmatic about access to services, with the majority of service users being satisfied with remote access. 23
Notwithstanding, some service users in this study speculated that they might have responded to telemedicine differently had they ‘received bad news’. This is particularly interesting when we consider that the two women who did receive a serious fetal diagnosis remained positive about telemedicine. Why a serious diagnosis ought to be mediated differently was unclear and outside the scope of this study; this issue should be examined in future studies. It would also be useful to understand the impacts of having a serious diagnosis at a distantly located FMC.
The views of the management stakeholders highlighted major structural and financial issues that are beyond the scope of this discussion. With any small-scale pilot, it is difficult to provide economic evidence, other than case studies, consistently a limiting factor for scaling up of digital health.24,25 In this project, additional staff funding was available through the pilot, but could not be utilised due to local staff shortage. One of the major barriers was concern about the impact on routine obstetric ultrasound provision (for both the pilot and ongoing implementation). Pressurised work environments can impact negatively on staff acceptance of digital health; other studies support this finding.17,19,26–29 Frequently, productivity improvements are of no benefit to frontline staff, who simply have to see more service users in the same time. 26 As this is set against a context of increasing austerity and cutbacks to the National Health Service, a pilot that will explicitly create additional work (i.e. Sonographers having to support specialist consultations rather than referring the service user to the FMC) was unsurprisingly greeted with some reservations.
In the event, the impact on workload was less significant than was feared; two factors contributed to this. First, within the time taken to gain management approval for the pilot, the staffing situation improved – largely due to Sonographers returning from maternity leave. Second, the DGH Obstetrician leading the pilot encouraged a rationalisation of scan requests from Obstetricians. Nonetheless, work is needed to investigate how other benefits, such as reduced referrals due to improved local skill levels, and the increased access to specialist input that telemedicine facilitates, outweigh the additional costs to obstetric ultrasound at the DGH.
The staff stakeholder group indicated the most complex responses. Initially, all participating Sonographers found the remote consultations challenging. Sonographers felt under pressure to acquire images on demand, and being observed caused anxiety; it was reported that telemedicine required them to stop scanning intuitively and so interrupted routine practices. Similar concerns have been reported in relation to Tele Intensive Care.30,31 Nevertheless, it was apparent that these challenges impacted individual Sonographers differently. One reported finding their work more interesting and challenging, which led to increased job satisfaction and confidence. Another reported finding the experience very stressful; in one instance, for example, failure to acquire an image had prompted feelings of incompetence which then undermined confidence. So, whilst one thrived the other felt discouraged – albeit they remained supportive of the pilot.
Staff acceptance is frequently identified as a barrier to adoption.17,19,28,29,32 Greenhalgh et al. identify four categories of clinician resistance to the introduction of new technology: resistance to policy, resistance to material aspects of the technology itself, resistance to compromised professional practice, and to compromised professional relationships. 28 In this case, there was resistance to perceived policy that would introduce new work. There was suspicion because the proposal came from the specialist consultant and concerns that it might be counter to local management policy. Problems with material aspects of the technology itself were certainly encountered and needed to be overcome, for example the size and layout of the room and protocols for running the session. Whilst the facilities remain the same, protocols evolved through experience. Feelings of compromised professional practice and relationships were certainly evident in Sonographer staff; they expressed significant concerns about running a session with other professionals present and with themselves perceived as ‘junior partners’ in the process.
Therefore, there remain some outstanding questions. In relation to clinical stakeholders, it would be useful to understand what factors contributed to the diverse reaction to telemedicine experienced by Sonographers. With regards to service users, we need to understand better how they balance preferences for conventional face-to-face interactions with convenience; how this relates to receiving bad news; and whether this preference decreases with experience of using video.
The use of clinical video-consultations is starting to be introduced in many contexts without a thorough examination of how it changes the nature of the consultation, the service user–clinician relationship and the relationship between different groups of professionals. Le Rouge et al. discuss how video modifies the service relationship and propose that both service users and staff need appropriate preparation and training. 33 There is an opportunity to do this within undergraduate education and as part of continuing professional education, which we have explored in a recent paper on the subject. 34 There is also scope for professional institutions to take a lead and develop new standards of technology-enabled care delivery.
In the case of fetal telemedicine, however, DGH managers and clinical stakeholders quickly recognised the benefits of the service to women. There were also tangible benefits for clinical staff (such as direct access to specialist support with immediate input/feedback), which facilitated them to feel more confident in the management of complex pregnancies. Early, tangible benefits are recognised enablers to adoption.19,35 After reviewing the pilot and its benefits, the DGH decided to adopt the telemedicine service. Since inception to February 2020, 303 telemedicine consultations have taken place.
Conclusion
This evaluation has highlighted a range of benefits for service users and clinicians resulting from the introduction of fetal telemedicine. Women with complex pregnancies benefitted from improved convenience (efficiencies in time and money) and better case management of their pregnancies. Participating Sonographers were upskilled, able to undertake advanced scans and interpret images better; and had better access to specialist support. Further, Obstetricians also benefitted from increased access to specialist support and, being better supported, consequently their management of high-risk service users improved, and they developed insight into managing complex pregnancies.
Moreover, this study has made clear the capability of telemedicine. It has shown that it is not always necessary to have expertise on site, and that such expertise can be accessed safely and remotely via telemedicine. Indeed, it has provided demonstrable evidence of a potential solution to some of the healthcare challenges facing rural hospitals.
Supplemental Material
sj-pdf-1-dhj-10.1177_2055207620925929 - Supplemental material for Service user and staff acceptance of fetal ultrasound telemedicine
Supplemental material, sj-pdf-1-dhj-10.1177_2055207620925929 for Service user and staff acceptance of fetal ultrasound telemedicine by Elaine Bidmead, Mabel Lie, Alison Marshall, Stephen Robson and Vikki J. Smith in Digital Health
Footnotes
Acknowledgements
We would like to thank the women who participated in the pilot. We would also like to thank participating staff at Trust1 and Trust2; and to acknowledge the important contribution of the Sonographers in particular. We would like to thank Bob Beckwith for managing the technology set-up.
Contributorship
SR and AM conceived the study. VS was involved in protocol development, gaining ethical approval, and patient recruitment. SR and VS conducted the telemedicine consultations. ML conducted the patient interviews and data analysis of patient data. EB conducted interviews with clinical and management staff and data analysis of that data (with AM). EB wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted for the evaluation of the service from the Health Research Authority Research Ethics Committee (REC), NRES Committee London – Hampstead REC reference: 14/LO/1671.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Academic Health Science Network North East and North Cumbria (AHSN NENC).
Guarantor
AM
Note
a. The link was not made from the children’s ward, rather the FMC consulting rooms are directly beside the waiting room which accounts for the background noise reported.
Peer review
This manuscript was reviewed by reviewers who have chosen to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.