
Abstract
A fecaloma is a solid fecal mass that prevalently forms over time due to fecal matter stasis secondary to chronic constipation, usually in the rectum and sigmoid colon. Computed tomography (CT) is the most helpful imaging technique for this diagnosis. Two case studies of rectosigmoid fecaloma compared by ultrasonographic and CT images are provided. The first case described a 60-year-old female patient with dementia who was admitted with anemia and abdominal distension, despite defecation care for chronic constipation. The second case reported a 50-year-old male patient who presented with nausea, abdominal distension, and daily water-soluble stools. Both patient cases used sonography, as a simple and noninvasive imaging technique compared with CT for fecaloma evaluation.
A hardened fecal mass, also known as fecaloma, usually forms over time because of fecal matter stasis, secondary to chronic constipation. 1 A fecaloma is a rare but severe consequence of fecal impaction (FI) in the sigmoid colon and rectum. 1 This gastrointestinal condition is typically identified on an abdominal computed tomogram (CT) and encountered in course of providing routine medical care. However, the available published information on the use of ultrasonography for detecting a fecaloma, in adults, is limited. These patient cases describe the usefulness of transabdominal ultrasonography (US) for documenting and assessing a fecaloma.
Case Series
Two patients were first assessed with CT imaging, which is the standard method for accurate detection of a fecaloma. Sonograms were acquired in both same patients immediately after identifying a fecaloma in the colon by CT. An Aplio ultrasound equipment system (Toshiba Medical, Tokyo, Japan) equipped with a 5-MHz curved-array transducer 2 was used for imaging. A systematic sonographic imaging method was used in this study to visualize the large intestines of both of these patients. The ImageJ software application (US National Institutes of Health, Bethesda, MD, USA) was used for image analysis and processing. The transducer was positioned on the abdominal skin approximately 2 cm above the symphysis pubis, while the patients were in the supine position. The resulting sonograms was performed with the patients having a full or partially filled urinary bladder. The transducer was angled at approximately 15° caudal, from the transverse plane. 3 A credentialed sonographer measured the transverse rectal diameter from the opposing outer rectum walls. These measurements were repeated three times, based on all the US and CT images. Two independent credentialed sonographers evaluated the sonograms to ensure interrater reliability.
Patient Case 1
A 60-year-old female patient with dementia was evaluated at the hospital for anemia and abdominal distension, despite regular defecation care for chronic constipation. The patient was confined to bed with a spinal subdural hematoma. Physical examination revealed mild abdominal tenderness to palpation and abdominal distension but with no signs of peritonitis.
The CT examination revealed FI from the descending colon to the rectum and rectosigmoid colon, which formed a well-defined intraluminal fecaloma. The mass had a maximum cross-sectional (MCS) diameter of 8.7 cm (See Figure 1A). The descending colon was also dilated. An obstructing intraluminal mass or stricture, in the rectosigmoid region, was not observed. The US examination detected rectal fecal retention as a crescent-shaped acoustic shadow with an MCS diameter of 6.3 cm (See Figure 1B).
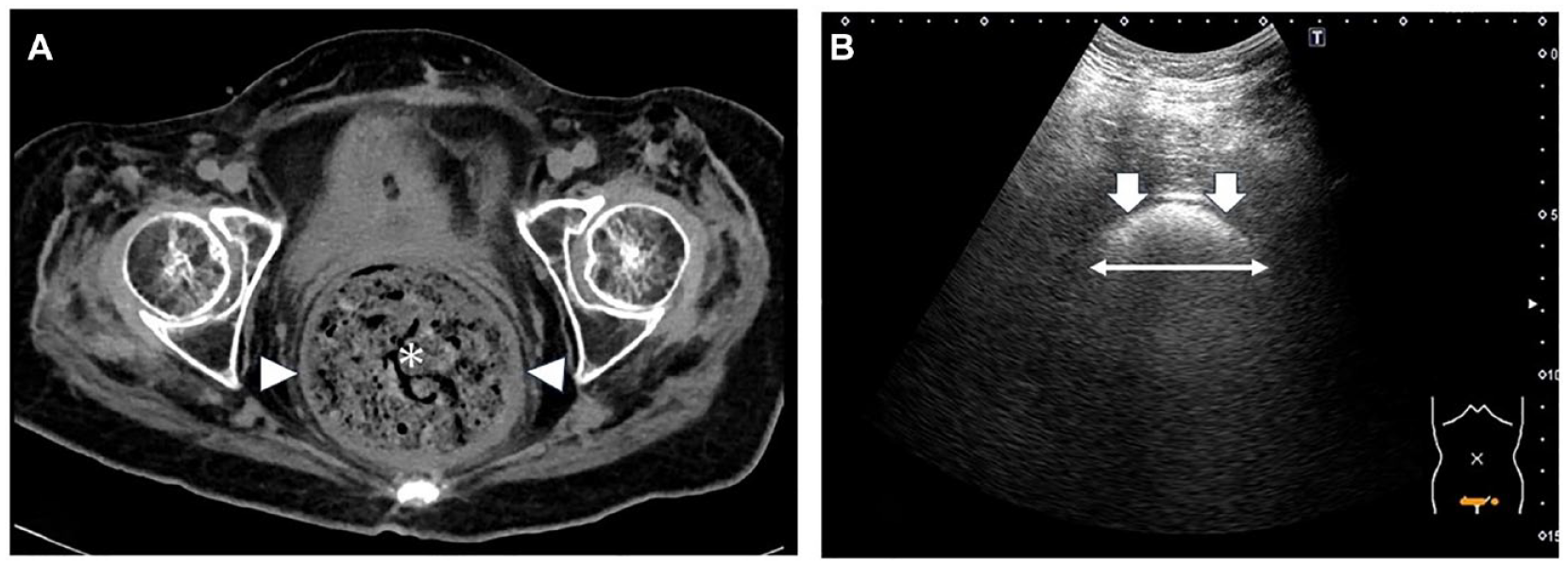
(A) A computed tomogram demonstrated a fecaloma with a maximum cross-sectional (MCS) of 8.7 cm (See arrowheads) and rectosigmoid colon dilation, due to fecal impaction (See asterisk). (B) A transverse sonographic view is provided that demonstrates strong high echoes from the rectal lumen, with a crescent-shaped acoustic shadow (arrows) with an MCS diameter of 6.3 cm (See double-headed arrow).
Patient Case 2
A 50-year-old male patient was evaluated in the hospital due to nausea, abdominal distension, and daily water-soluble stools. This patient reported a clinical history of subarachnoid hemorrhage resulting in paraplegia and wheelchair dependence. A physical examination revealed mild abdominal tenderness to palpation and abdominal distension but no signs of peritonitis.
The CT examination detected FI from the descending colon to the rectum and rectosigmoid colon. An incidental finding of a fecaloma, having an MCS diameter of 9.1 cm, was noted in the rectosigmoid colon (See Figure 2A). The descending colon was also noted to be dilated. An obstructing intraluminal mass or stricture in the rectosigmoid region was not observed. The sonogram allowed for the visualization of the rectosigmoid colon fecaloma, as a crescent-shaped acoustic shadow. The mass had a MCS diameter of 7.3 cm (See Figure 2B). As a result, overflow fecal incontinence, with a fecaloma, was diagnosed based on the CT and US diagnostic results. The patient underwent enemas and manual disimpaction to relieve this obstruction.
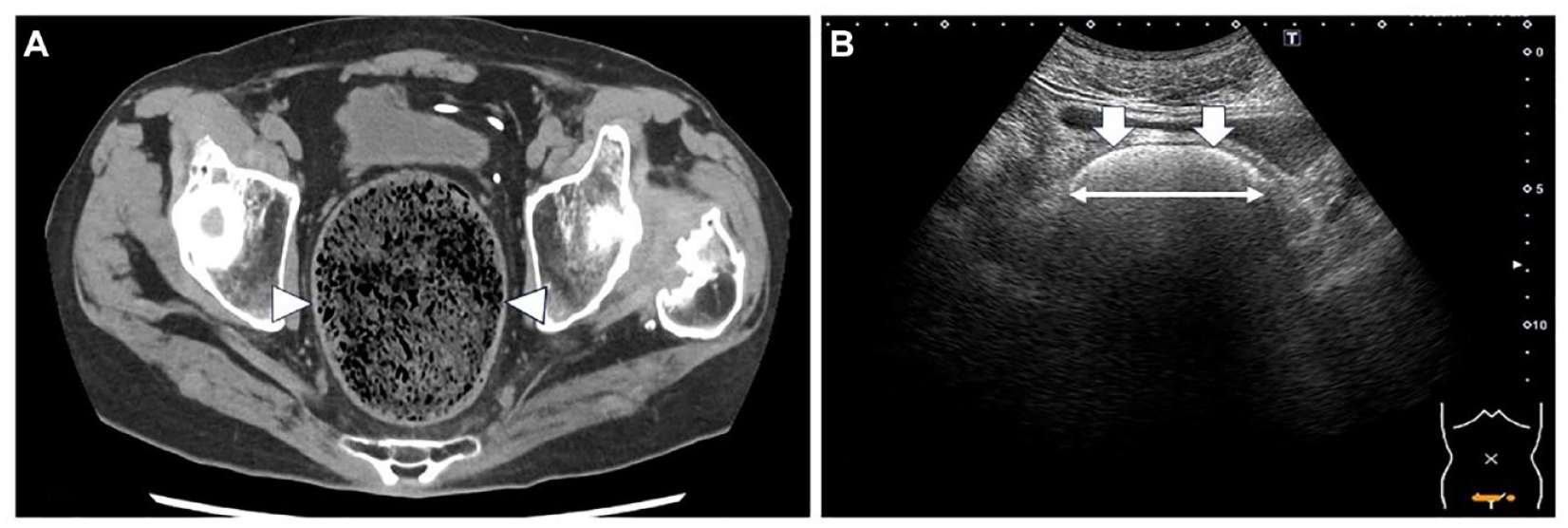
(A) A computed tomogram demonstrated a 9.1-cm fecaloma (see arrowheads) in the rectosigmoid colon. (B) A transverse sonographic view provided strong high echoes from the rectal lumen, with a crescent-shaped acoustic shadow (see arrows) with a maximum cross-sectional (MCS) diameter of 7.3 cm (See double-headed arrow).
Discussion
Fecalomas are associated with a considerable risk of life-threatening sequelae, including large bowel obstruction, colonic perforation, and very rarely, colonic hemorrhage. Fecal impaction is a risk factor for elderly individuals, 4 despite affecting children and individuals with underlying neuropsychiatric diseases, 5 and has significant health care, socioeconomic, and quality-of-life consequences.
Fecaloma is an organized hardened fecal mass that causes impaction, predominantly in the rectosigmoid colon. A CT examination can promptly identify FI and directs treatment, thereby preventing severe complications. 6 Patients are diagnosed when a large fecal mass in the colon and rectum and this is often demonstrated on CT images. 7 Studies have demonstrated fecaloma having MCS diameters as large as 11 to 12 cm on a CT image.8 –11 One study defined FI, based on the results of a CT, such as a distended colon, with a fecal mass or dehydrated fecaloma packed, in the colon, a distended left-side colon, with a cylindrical shape, and an MCS diameter of >6 cm. 12 The current patient cases indicated that CT was able to detected fecaloma with MCS diameters of approximately 7 to 9 cm, which exceeds the 6 cm definition. Interestingly, there was no evidence of colonic wall thickening, which would have indicated acute edema or inflammation.
FI is the involuntary discharge of liquid or solid stools. Patients with FI frequently have slight diarrhea, frequent bowel movements, and loose stools (i.e., based on the Bristol Stool Form Scale types 5–7), regardless of the etiology. 13 Rectal hyposensation due to spinal cord impairment or aging masks the urge to defecate even when the rectum is filled with stool, frequently causing overflow FI in some patients. 13 This problem affects both men and women, irrespective of their social, employment, or financial status. 13 The patient with paraplegia in the current study did not suspect FI, by fecaloma, because of his frequent water-soluble stools. In addition, both US and CT examinations detected a rectosigmoid colon fecaloma, confirming the diagnosis, with overflow FI, based on clinical symptoms and surveillance. However, neither US nor CT can distinguish between a fecaloma and fecaloma with overflow FI.
Previous US studies have demonstrated that fecal retention, in the rectum, is characterized by a crescent-shaped acoustic shadow, compared with the CT definition of fecaloma as a hardened fecal mass, with an MCS diameter of >6 cm.3,14 In healthy adults, storage of rectal feces averages 4 cm in colonic diameter. 3 The current case series demonstrated that US detected rectal fecaloma, as crescent-shaped acoustic shadows, with MCS diameters of approximately 6 to 7 cm. It was also noted that a difference of approximately 2 cm between the measured CT and US MCS diameter values. CT is considered more reproducible than US, in the detection of a fecaloma. 12 The use of CT allows for the delineation of the largest transverse diameter of a fecaloma, however is challenging on US, due to posterior acoustic shadowing from stool. Determining a fecaloma with US is difficult because of the small number of published cases, as evidence for referral. However, the fecaloma may be >5 cm because it is approximately 2 cm shorter than it appears on a CT image.
Complications from the effects of a fecaloma, on the intestinal wall and adjacent structural damage, may cause death. 15 Thus, early fecaloma detection in high-risk groups prevents the need for ordering CT and US. However, US may be practical as a primary assessment, considering that CT exposes patients to ionizing radiation and requires a hospital or free standing imaging facility visit. US is low cost and fast to perform, and allows for noninvasive surveillance. In addition, US equipment systems can be is brought to the patient for a bedside examination. Therefore, CT is the diagnostic gold standard for making a fecaloma diagnosis. However, US is a suitable diagnostic tool for diagnosing fecaloma and providing surveillance for patients with constipation.
Conclusion
Fecaloma, as a result of an FI, is a prevalent problem in elderly individuals, especially those with mobility impairments. US is a simple and noninvasive diagnostic technique that can be used, similar to CT, to evaluate the presence of fecaloma, among adult patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study since it did not comprise of a research study. The case study presented is for educational purposes only.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).