
Abstract
Although foreign body (FB) ingestion is common in childhood, most cases do not have any clinical significance. Radiologic evaluation is crucial to determine the exact location of a persistent foreign body because it dictates the therapeutic approach. In this case report, we present a child with appendiceal perforation caused by a FB and emphasize pitfalls in preoperative imaging assessment. A 3-year-old boy presented with subtle abdominal pain duration for three months. The preoperative imaging examinations were consistent with an intraluminal metallic pin. However, the operative findings and postoperative pathological examination showed that the pin perforated the appendiceal wall, causing chronic inflammatory changes with an omental reaction around the extraluminal part of the pin. The patient underwent appendectomy with an uneventful course. Foreign body is a rare cause of appendiceal perforation with resultant appendicitis. Imaging may reveal some clues regarding the location, but the interpretation of radiologic data could be quite challenging.
Foreign body (FB) ingestion is common in pediatric emergency services. In the United States, each year it is discovered in 100 000 patients, and approximately 80% occurs in a pediatric population.1–3 An ingested FB may be organic or inorganic, sharp or blunt, and usually pass through the digestive system without complaints. 4 However, there may be acute abdomen symptoms due to perforation or even acute appendicitis in a small number of patients. Perforation is seen in 1% of the cases, and it mostly occurs with sharp objects, whereas blunt objects might cause inflammation in intestinal segments with abscess, especially in the appendix.5,6 Radiologic investigations should be performed properly for better patient management follow-up after treatment. We present a child who underwent appendectomy due to perforated appendicitis caused by an ingested pin with spherical head in which the imaging findings were misinterpreted.
Case Report
A 3-year-old boy presented with vague abdominal pain to a primary health care facility. Although there was no relevant history, a plain abdominal radiograph showed an opaque, needle-like FB in the right lower quadrant (RLQ), and the family was advised to take him to a tertiary care center. Patient was then admitted to the emergency room for the ingested pin but was asymptomatic. A plain abdominal radiograph was reordered due to the poor quality of the first radiograph and to display the movement of the pin (Figure 1). The patient was discharged with a scheduled appointment at the outpatient clinic two days later since there was no movement and he had no symptoms of intestinal perforation or significant abdominal pain. But the family did not come to their appointment and came back to the outpatient clinic three months later. Abdominal palpation revealed subtle tenderness in the RLQ. Laboratory values including a leukocyte count was within normal limits. A repeat plain radiograph showed a FB in the same exact RLQ location. Concurrently, a plain radiograph revealed the preoperative exact location, and a computed tomography (CT) scan confirmed a FB in the RLQ. Due to the prominent metallic artifacts and a small amount of intraabdominal fat tissue, an optimal imaging assessment could not be completed (Figure 2). Therefore, a sonographic exam was performed, and the FB was interpreted as a pin with the spherical head located within the lumen of the terminal ileum adjacent to the ileocaecal valve (Figure 3). There was no free or loculated fluid in the abdomen. A laparoscopic exploration was undertaken since the FB remained in the exact same position during the past three-month period. It revealed that the pin was contained within the lumen of the appendix with a tiny perforation at the tip and an omental reaction enwrapping the appendix. An appendectomy was performed laparoscopically at the same session (Figure 4a, 4b). The postoperative course was uneventful. Histopathological examination revealed chronic inflammatory wall changes and appendiceal perforation.

A 3-year-old male presented with vague abdominal pain. The abdominal radiograph demonstrates the needle-like foreign body located in the right iliac fossa (arrow).
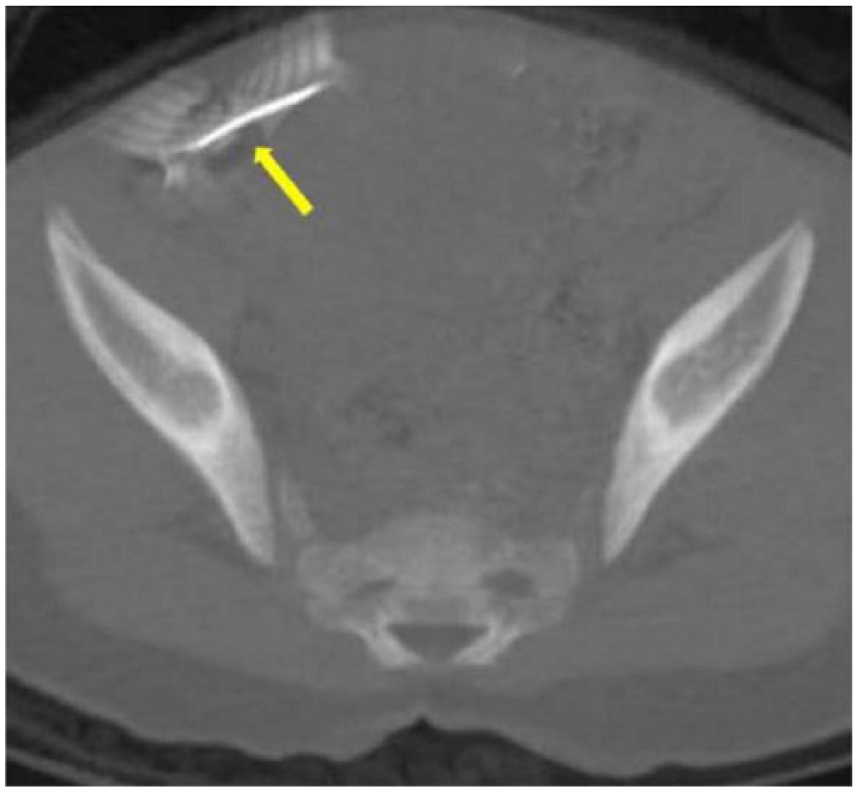
An axial computed tomography image. The foreign body is located in the right lower quadrant (arrow). Because of beam hardening artifacts and small amount of intraabdominal fat tissue, an optimal assessment could not be done.
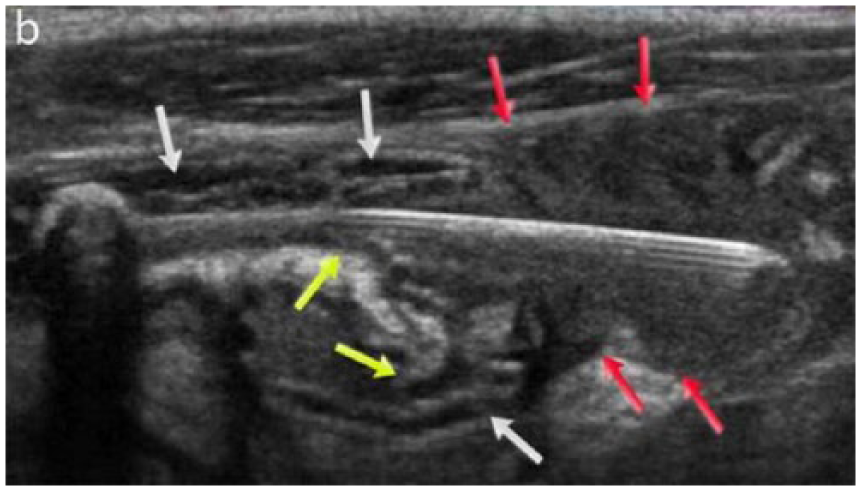
The sonographic appearance of the pin within the appendiceal lumen. The appendix has C-shaped and corrugated contours (yellow arrows). The omental tissue is enwrapping around the extraluminal part of the pin (red arrows). Chronic appendiceal wall changes mimicking ileal wall structure (white arrows). The tip of the appendix probably could not be visualized because the omentum completely encased the area.
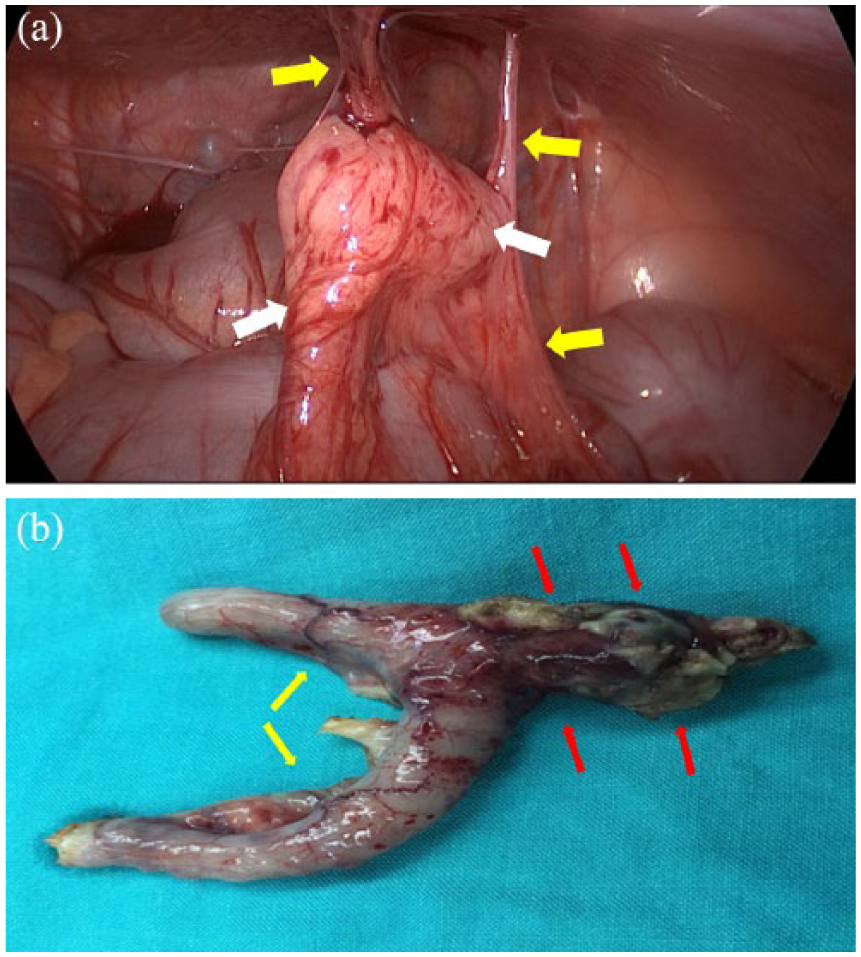
(a) The laparoscopic appearance of the appendix (white arrows) is suggesting a prominent omental reaction around the appendix and attachment to the abdominal wall (yellow arrows). (b) The macroscopic findings of the appendectomy material. Appendix contours seem C-shaped and corrugated (yellow arrows). The omental tissue is enwrapped around the extraluminal part of the pin (red arrows).
Discussion
Foreign body ingestion is relatively common, and most FBs pass the gastrointestinal (GI) tract spontaneously; therefore, an expectorant management is usually undertaken. 4 A surgical exploration should be performed for those stuck in the appendiceal lumen or extraluminal extension. Surgical interventions may be utilized as a laparoscopic or open procedure for appendiceal FBs. In addition, laparoscopy has been described as safe, efficient, and feasible.1,2 The preoperative radiologic assessment is critical especially when sharp objects are concerned. Because of the operative findings in this pediatric patient, we retrospectively evaluated the preoperative imaging data to define the exact causes that resulted in the misinterpretation of the FB location.
The rate of perforation after ingested FBs is less than 1%, and it usually occurs in the small intestine.6,7 The FB may cause a microperforation on the wall of the intestinal segment accompanied by the chronic inflammatory reaction. This kind of perforation generally does not cause acute symptoms and may remain silent for months or even years.5,6,8 Sometimes, these chronic changes are seen on radiologic evaluations performed for any other reasons or defined at a surgical operation as in the presented case. 8 Nicolodi et al. 6 described CT findings of an intestinal perforation caused by a sharp FB in the distal ileal segment. Song et al. 4 established a case that has acute appendicitis with no perforation. They described acute appendicitis with just CT and radiographic findings in their publication. Different than those published, the present case had a perforated appendicitis caused by a sharp long-standing FB with no acute abdominal pain. The FB within the appendiceal lumen caused a chronic inflammatory reaction of the wall of the appendix, as confirmed by histopathological examination. The changes suggest submucosal edema and thickness seemed like a mucosal fold of ileal wall. In addition, the tip of the appendix could not be visualized probably because the omentum completely encased the area. Because of irregular and thickened wall and failure to detect the tip of the appendix, the sonographic appearance of the appendiceal wall imitated ileal wall. Furthermore, there was no free fluid in the abdomen, and the patient did not have acute abdominal findings compatible with a perforated appendix.
On sonographic assessment, the vermiform appendix extending from the cecum can be seen as a compressible intestinal segment with a worm-like appearance, and the length of appendix ranges from 2 to 20 cm. 9 The maximum outer diameter of the appendix is generally acknowledged as 6 mm in children.6,10 Appendiceal wall thickness, luminal distension, and increased outer diameter are the detectable findings in case of acute appendicitis on sonography. Besides, fluid collection, discontinuity of wall, and decompression could be counted as perforation. In prolonged cases, the appendix could be seen elongated and scarred as a result of chronical changes. The appendiceal wall thickness may increase, and wall contours may be irregular. An accompanied echogenic omental reaction may be seen. Sometimes the findings may mimic acute appendicitis. Radiologic examinations are essential in the assessment of FBs’ location and potentially accompanying complications. The choice of the imaging methods mostly depends on the content of FBs and may extend from a plain radiograph to magnetic resonance imaging (MRI). Radiography and CT have a sensitivity of 29% and 63% in detecting FBs, respectively. 11 Considering abdominal radiograph, CT, and sonography, sonography is regarded as an extremely sensitive tool imaging both radiopaque and radiolucent objects. The sensitivity of sonography is around 95% for detection of FBs, but it is significantly reduced in cavities with air. 12 On sonography, FBs usually appear hyperechoic in comparison to adjacent tissues, and objects such as plastic or wood may have posterior shadowing, while metal FBs have comet tail or reverberation artifact. 13 Although sonography is a widely used and highly sensitive diagnostic tool for children, it has the disadvantage of defining the exact location of the involved intestinal segment. 14 To increase diagnostic accuracy, it is important to consider that chronic inflammatory changes in the intestinal wall may obscure the sonographic findings.
Conclusions
Endoscopic removal or surgical exploration are the treatment choices for ingested FBs, and imaging methods are essential for management. Sonographic imaging may be the first choice in the diagnostic search for FBs; however, it should be noted that a sonographic evaluation may be misinterpreted in a prolonged case. In addition, it is important that in these diagnostic cases that the appendix tip is detected and visualized. The location of a FB and accompanied complications are crucial for accurate diagnosis and treatment option.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.