
Abstract
The aim of this study was to compare ultrasonographic assessment of fecal loading in adults with that of computed tomography. Ultrasonography (US) was performed on 43 adult patients immediately after abdominal computed tomography images had identified fecal loading in their colons. In 18 of 43 patients (haustrations-visualized cases), fecal loading was detected as crescent-shaped acoustic shadows associated with haustrations behind the strong echoes off the colon wall. In the remaining 25 patients (haustrations-not-visualized cases), fecal loading was detected as attenuating echoes with multiple high echoic spots behind weak high echoes off the colon wall in 17 patients and similar to those seen in the haustrations-visualized cases but without haustrations in 8 patients. US can be used for qualitative assessment of fecal loading in the colon. This new technique is simple and noninvasive and can be used concomitantly with physical examination to assess severity of constipation.
Introduction
Constipation, a very common condition, is a chronic problem for many people, particularly elderly ones. 1 Chronic constipation can be associated with medical comorbidities and complications such as intestinal impaction and obstruction, anal fissures, hemorrhoids, colonic perforation, volvulus, and irritable bowel syndrome.2-7
The diagnosis of chronic constipation begins with a thorough medical history and physical examination. Widely recommended diagnostic tests for constipation include physiologic tests for colonic transit, anorectal manometry, and balloon expulsion parameters. Also, various imaging studies—plain abdominal radiography, barium enema, colonoscopy, defecography, abdominal computed tomography (CT), magnetic resonance imaging (MRI)—often reveal pathophysiologic abnormalities in selected patients with constipation.5,8,9 Plain radiography is a generally useful, inexpensive test that provides information complementary to the clinical history and physical examination in children and adults with constipation. 10 Barium enemas and colonoscopy may be useful for detecting abnormalities such as megacolon, stenosis, extrinsic compression, and intraluminal masses. Defecography provides useful information about anatomical and functional changes in the anorectum. CT scanning is a highly useful and highly sensitive diagnostic tool. In particular, CT can be considered a gold standard for assessing any constipation present because it allows clear, continuous visualization of the stool properties inside the colon.2,11-13 MRI has the advantage of visualizing all compartments of the abdomen. 9 However, these procedures have a number of limitations. Plain abdominal radiography, barium enemas, defecography, and CT scanning expose patients to radiation. Barium enemas and defecography require use of a contrast medium. Colonoscopy is often poorly tolerated by patients. MRI and defecography are costly and lack standardization. Each of these procedures also may provide inadequate information and are unsuitable for follow-up testing of constipated patients. 8
Transabdominal ultrasonography (US) could be a practical test in primary and secondary care because it is noninvasive and its radiation is nonionizing.14,15 Several recent studies have reported using a pelvic US technique to diagnose constipation when measuring the rectal diameter in children. US images show a fecal mass in the rectum as a crescent-shaped acoustic shadow.16-22 However, there is little information available on sonographic visualization of fecal loading in adults. The aim of this study was to compare ultrasonographic assessment of fecal loading in adults with that of CT and to determine whether US assessment of stool retention is useful for identifying adults with chronic constipation.
Patients and Methods
Patients
Between April 2011 and April 2013, 85 consecutive adult patients presenting with abdominal distension and pain were examined by US immediately after they had undergone abdominal CT. Of this group, 43 consecutive patients (16 men and 27 women; mean age, 69.93 years; range, 35-92 years) whose CT images had shown fecal loading in the ascending and descending colons over a cross-sectional (luminal) area of greater than 10 cm2 were enrolled in a prospective study. Ten patients who only had dilated transverse and sigmoid colon and rectums were excluded because of the difficulty in precisely matching US and CT images. Informed consent for the study was obtained from all patients or from their guardians, as approved by the Ethics Committee of the hospital. All sonographic examinations were performed by a certified sonographer with ten years of experience and the static images interpreted by two gastroenterologists experienced in gastrointestinal sonography.
Technique
The patients were first assessed by CT imaging, the standard reference method for accurate detection of fecal loading,2,11-13 as it can clearly visualize stool properties inside the colon with few artifacts. Immediately after fecal loading had been identified in the colon by CT, US images were acquired with the patient in an identical position and using anatomical landmarks (the iliac crest for ascending and descending colon) to ensure the transducer was accurately placed to correspond with the relevant CT image. The transverse and sigmoid colon and rectum were not assessed by US because of the difficulty in precisely matching the CT images. Transverse and longitudinal sonographic scans were performed in all cases.
Data Analysis
The US images were allocated to one of the following two groups: (1) fecal loading detected as crescent-shaped acoustic shadows with haustrations, the sac-like foldings of the large intestine (haustrations-visualized cases; HV), and (2) evidence of fecal loading without detection of haustrations (haustrations-not-visualized cases; HNV). The HNV group was further subdivided into cases with weak high echoes of the colon lumen (HNV-weak) and those with strong high echoes of the colon lumen (HNV-strong), thus creating three groups altogether.
The HV and HNV groups were compared regarding the effects of the shape of the colon walls and brightness of the outer boundaries of the colon walls in longitudinal sections and quality of the colon lumens and posterior echoes (acoustic shadows) in transverse sections (Figure 1). The large bowel gas per cross-sectional area to fecal loading (colon-gas) ratio was calculated on CT images. Knowing this ratio is helpful because it is believed that the hardness of the fecal loading is related to the amount of gas in the colon. 9 Image J software (National Institutes of Health freeware; downloadable at http://imagej.nih.gov/ij/download.html) was used for image analysis and processing. US images, the combination of brightness of the colon wall, and strength of the posterior echoes were assessed using the following visual rating scale: 1, weak with high echogenicity; 2, intermediate with high echogenicity; and 3, strong with high echogenicity. The US images were assessed by five certified sonographers, and the average value allocated was used for analysis.
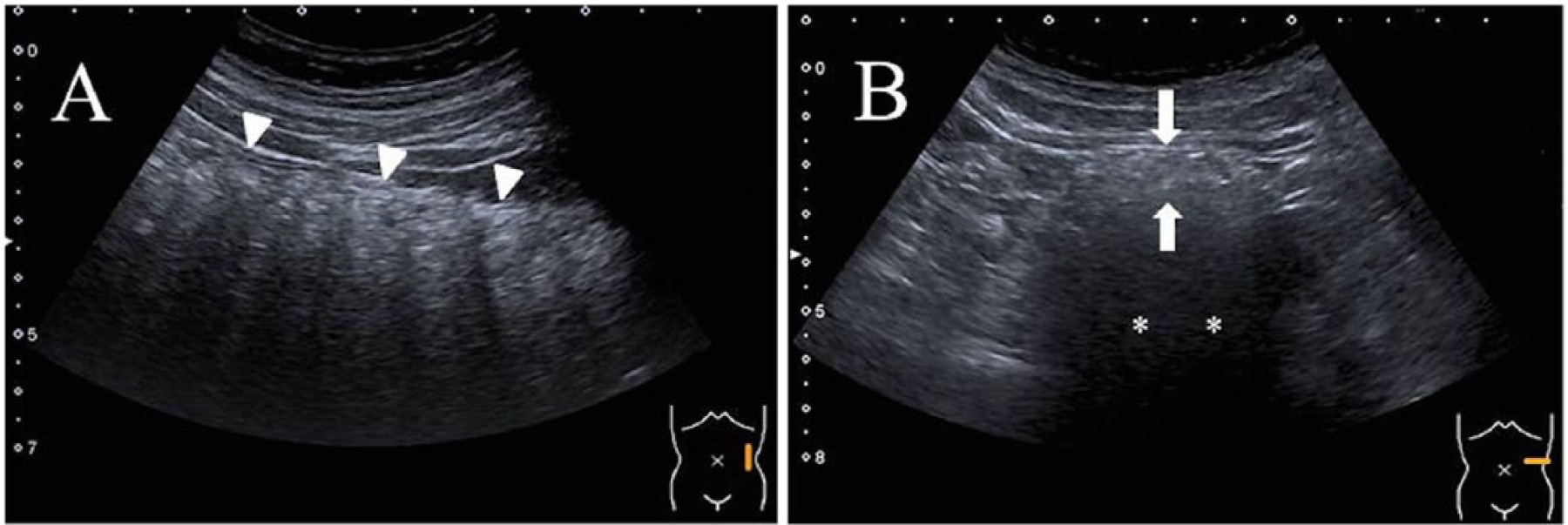
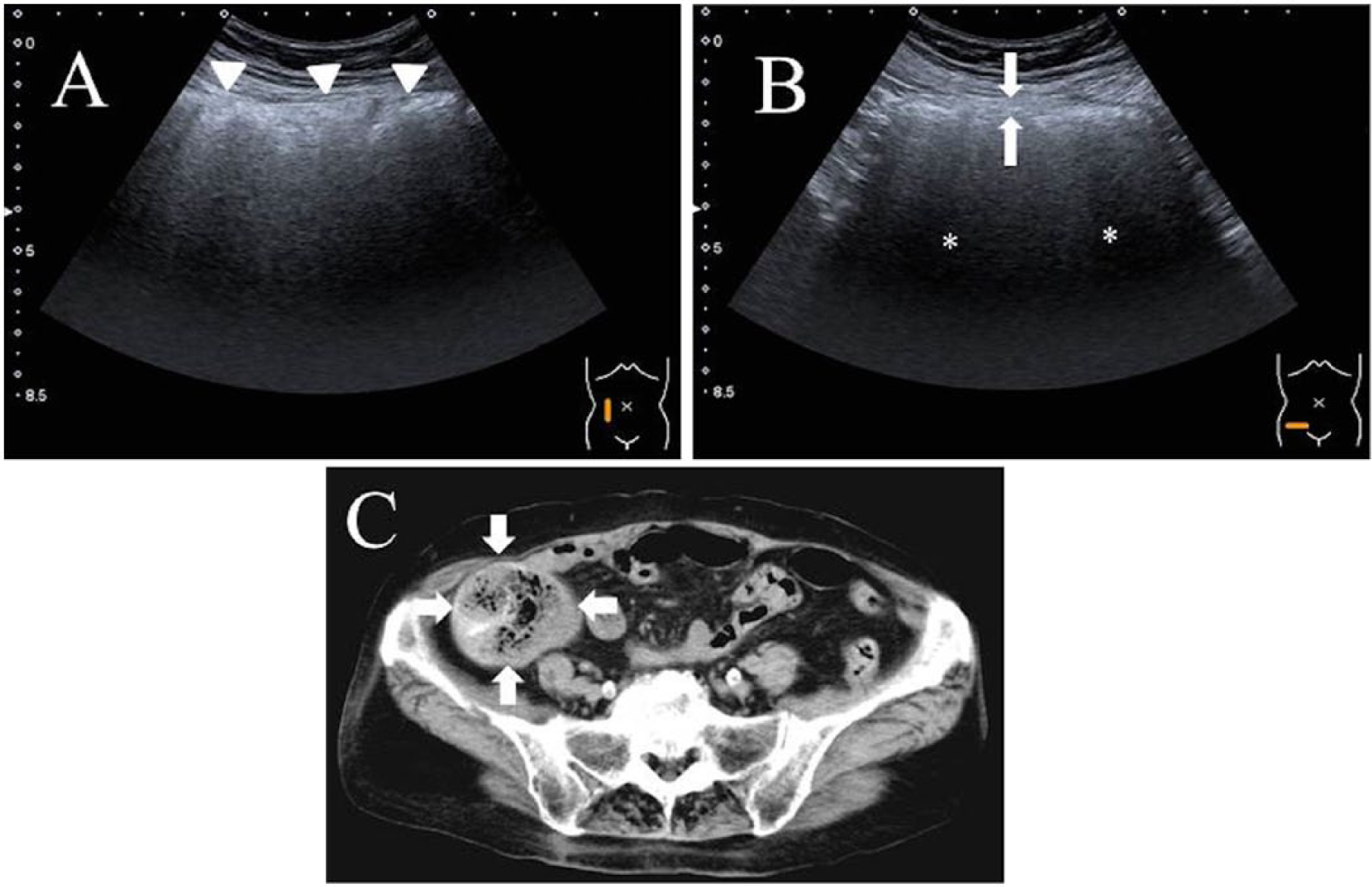
Ultrasonographic images from a 50-year-old man with normal bowel movements. (A) Longitudinal scan showing a flattened outer boundary wall and high echoes off the descending colon wall (arrowheads). (B) Transverse scan showing a marginally high echo of the colon lumen (arrows) and posterior echo behind the descending colon (asterisks).
The CT systems used were Asteion super 4 edition (Toshiba Medical Systems, Tokyo, Japan) and Xario and Aplio ultrasound systems with curved-array (5.0 MHz) transducers (Toshiba Medical Systems). For ultrasonographic imaging, the focal range used was 4 cm and the image depth 6 to 8 cm.
Statistical Analysis
Data are presented as the mean ± standard deviation (SD). One-way analysis of variance (ANOVA) was used for comparison of the mean colon-gas ratios among the groups. Statistical analyses were performed with SPSS 18.0 software (SPSS, Chicago, Illinois, USA), and values of P < .05 were considered to indicate statistical significance. The relationships between the visual ratings and the quantitative volumetric measurements were assessed using the nonparametric Kendall’s W test (Kendall’s coefficient of concordance).
Results
Table 1 shows fecal loading findings according to US images classified by type. In all 43 patients with fecal loading according to CT (HV group, 18; HNV group, 25), the fecal loading was detected by US as acoustic shadows behind the high echoic signals off the colon wall.
Classification of Fecal Loading in Ultrasonographic Images.
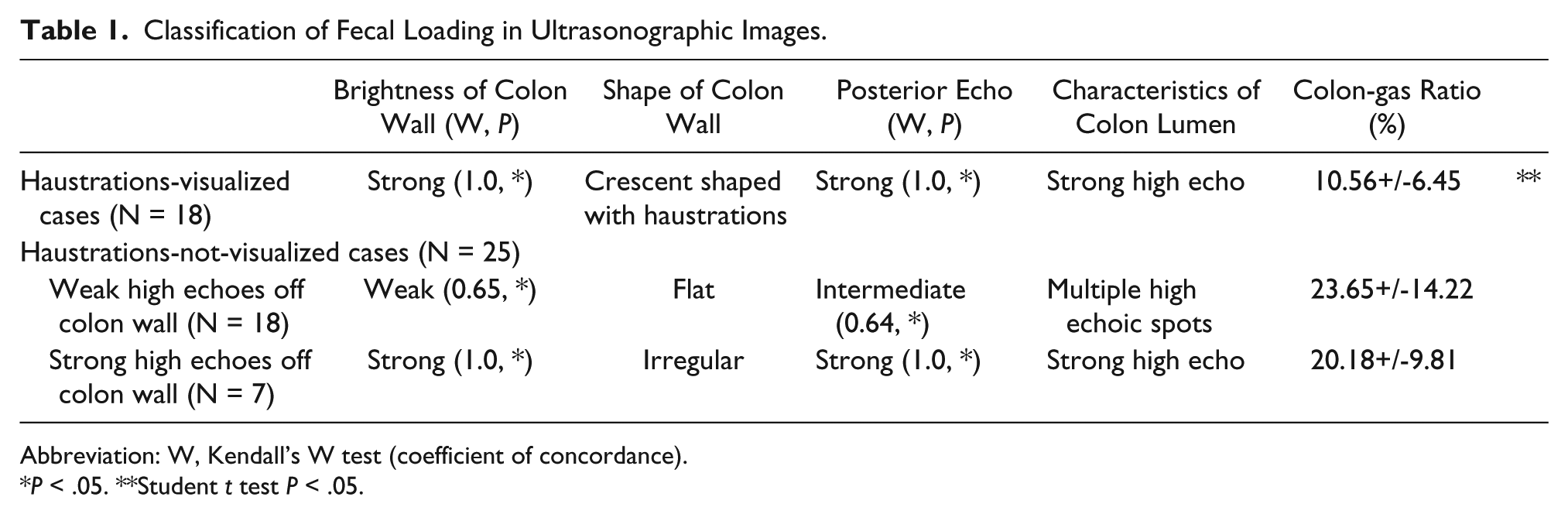
Abbreviation: W, Kendall’s W test (coefficient of concordance).
P < .05. **Student t test P < .05.
Fecal loading was detected as crescent-shaped acoustic shadows associated with haustrations in 18 of 43 patients (the HV group). There were strong high echoes behind the outer surface area of the ascending colon in 6 of 18 patients and of the descending colon in 12 of 18 patients (Figure 2). There were no significant differences in the US images of the ascending and descending colon. In 17 of 25 patients in the HNV-weak group, fecal loading was detected as attenuating echoes with multiple high echoic spots behind the weak high echoes off the outer surface area of the ascending colon in 16 patients and of the descending colon in 1 patient (Figure 3). In 8 of 25 patients in the HNV-strong group, the evidence of fecal loading was similar to that of the HV cases but without detection of haustrations and in all 8 patients involving only the ascending colon (Figure 4). There was a significant difference in colon-gas ratios between the HV and HNV-weak groups (P < .05). There was no significant difference in colon-gas ratios between the HV and HNV-strong groups and between the HNV-weak and HNV-strong groups. The results obtained using the three scales were highly correlated with each other (Kendall W, 0.64-1; P < .01).
Haustrations-visualized (HV) group: Images from a 70-year-old woman with chronic obstipation. (A) Longitudinal ultrasonographic (US) image showing a crescent-shaped acoustic shadow with haustrations and strong high echoes off the descending colon wall (arrowheads). (B) Transverse US image showing strong high echoes of the colon lumen (arrows) and a strong acoustic shadow behind the descending colon (asterisks). (C) Abdominal computed tomographic (CT) scan showing fecal loading in the descending colon with little gas in the colon lumen (arrows) (colon-gas ratio: 4.53%).
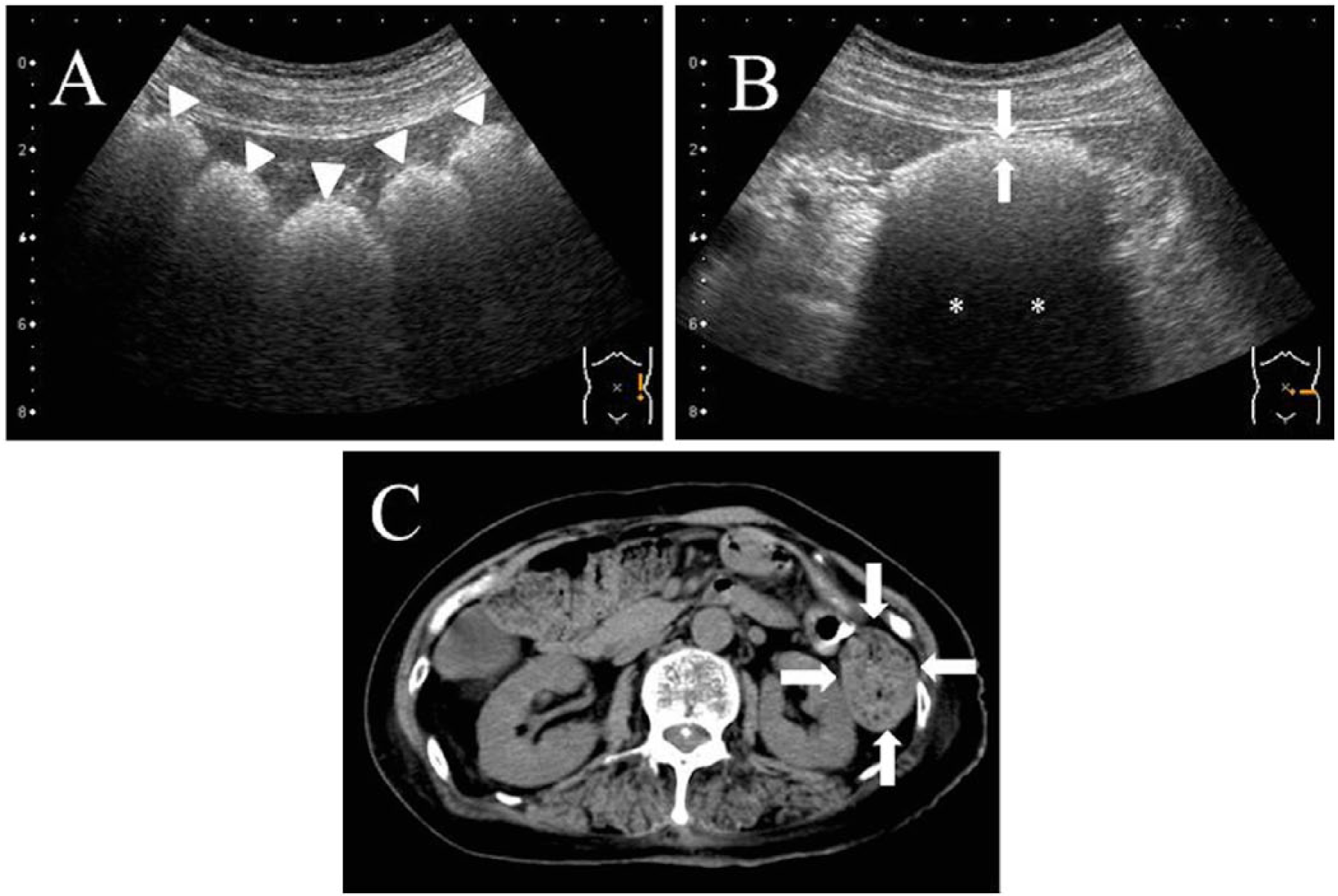
Haustrations-not-visualized (HNV-weak) group: Images from a 76-year-old woman with abdominal distension. (A) Longitudinal ultrasonographic (US) image showing a flat outer surface and weak high echoes off the ascending colon wall (arrowheads). (B) Transverse US image showing multiple high echoic spots of the colon lumen (arrows) and a normal acoustic shadow behind the ascending colon (asterisks). (C) Abdominal computed tomographic (CT) scan showing fecal loading in the ascending colon with abundant gas in the colon lumen (arrows) (colon-gas ratio: 25.42%).
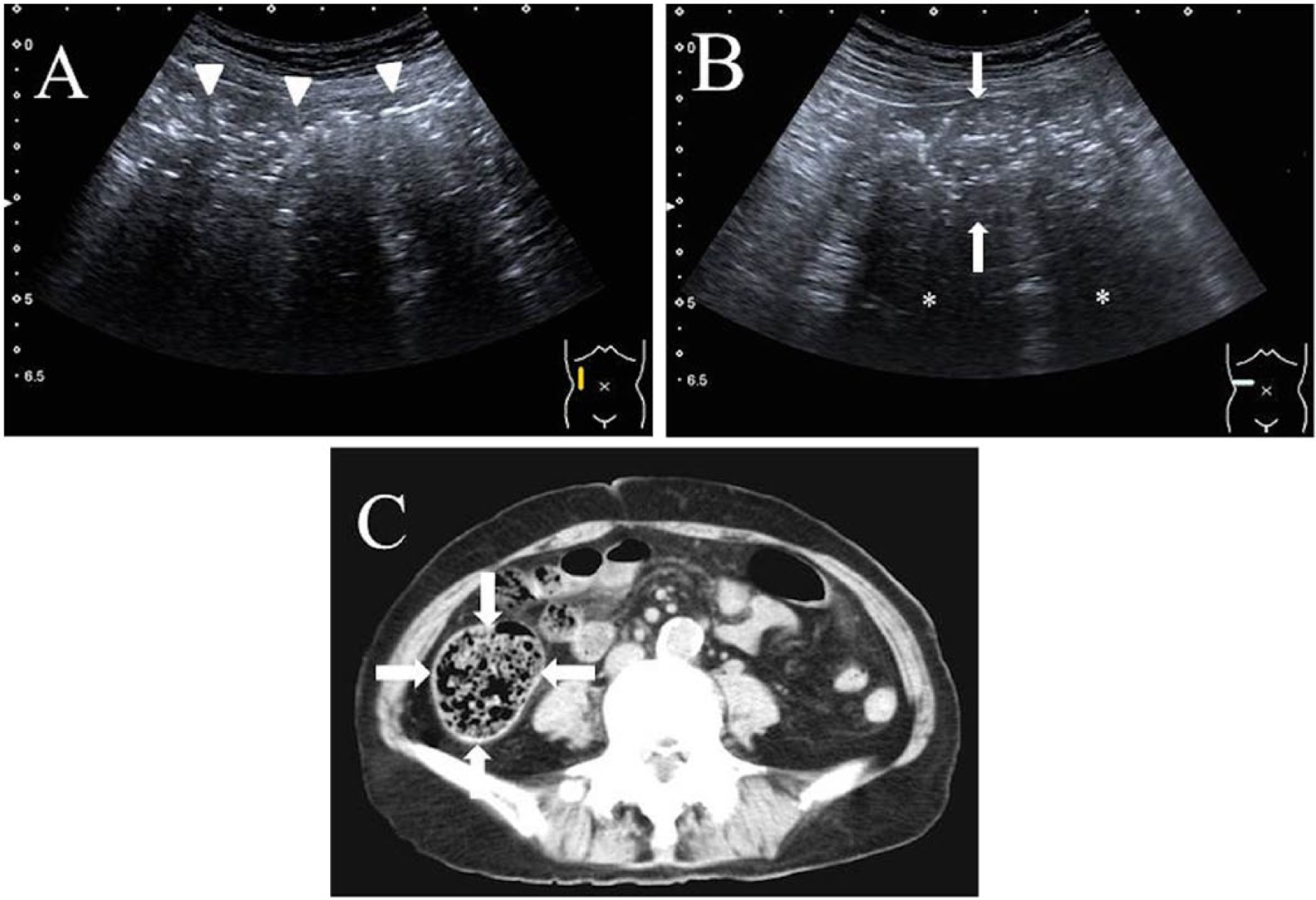
Haustrations-not-visualized (HNV-strong) group: Images from an 82-year-old man with chronic obstipation. (A) Longitudinal ultrasonographic (US) image showing irregularity of the outer surface and strong high echoes off the ascending colon wall (arrowheads). (B) Transverse US image showing strong high echoes of the colon lumen (arrows) and a strong acoustic shadow behind the descending colon (asterisks). (C) Abdominal computed tomographic (CT) scan showing fecal loading in the ascending colon with little gas in the colon lumen (arrows) (colon-gas ratio: 11.26%).
Discussion
Chronic constipation greatly affects patients’ quality of life. However, it is difficult to completely alleviate. Because the symptom of constipation occurs in many diseases, the reference standard varies between studies. 23 Some ambiguities in findings of diagnostic tests are attributable to functional and structural variations in the colon and assessment by too few imaging and too unreliable imaging procedures. To our knowledge, no other studies have documented a correlation between US and CT findings in adults with stool retention. This study describes a new US technique for assessment of stool retention in adults.
In this study, US imaging visualized fecal loading as acoustic shadows behind the high echoic signals of the colon wall. In the HV group, the bright reflection of echoes off the anterior surface with deep acoustic shadowing indicated that loading of hard feces in the colon was very likely. In contrast, in the HNV-weak group, there was a reduced reflection of echoes on the anterior surface because of the attenuating echoes, with multiple high echoic spots in the colon lumen. These high echoic spots were assessed as colonic gas on the CT images. Hence, hardness of fecal loading in adults in the HV-group (detected as crescent-shaped acoustic shadows with haustrations) was indicated because of the lower colon-gas ratios than were found in the HNV groups. Our study thus indicated that US can be used to assess the hardness or softness of fecal loading in adults. Fecal loading was found more frequently in the descending colon in the HV group than in the HNV group. Loaded feces are harder in the descending than in the ascending and transverse colons for physiological reasons.5,6 This may provide an explanation for the development of haustrations in the HV group. We used a US technique in this study that included a 5.0 MHz curved-array transducer and an image depth of 6 to 8 cm. We chose these parameters because the US images should be required to display not only echoes on the anterior surface but also the deep direction in the entire colon lumen. Also, curved-array transducers allow wide-angle observation in the colon lumen.
A few published studies have used pelvic US to evaluate rectal width in children.16,17,19-22 Pelvic US is a simple and reliable noninvasive screening method for evaluating constipation with minimal patient discomfort. However, there is insufficient evidence that the transverse diameter of the rectum is a predictor of constipation and fecal impaction, 14 and these studies only evaluated children’s rectums; they investigated neither the total colon nor adults. Moreover, because there is less attenuation of the ultrasonic beam by subcutaneous fat and muscle, which are both thinner in pediatric subjects, 24 the procedure may be more appropriate for children than for adults. In our study, we found that US, which can clearly visualize colonic disorders throughout the colon,25,26 can adequately evaluate the nature (hardness vs. softness) and location of fecal loading in adults. Therefore, US is a suitable tool for diagnostic screening and follow-up of patients with constipation.
Constipation, a frequent concern in older adults, is responsible for an increase in the number of institutionalized elderly people with impaired mobility.27,28 Constipation is not only a significant burden on health care systems but also an important contributor to decreased quality of life. Complaints of constipation and habitual use of laxatives increase with age. Patients with severe chronic constipation frequently use enemas. Idiopathic perforation of the colon caused by enemas occurs most commonly in elderly patients with chronic constipation.2-4 Thus, one should carefully consider this risk when recommending enemas for patients with constipation. In addition, enemas are minimally effective in patients with fecal retention in the right side of the colon (ascending and transverse colon), and enemas for fecal impaction in the rectum may worsen abdominal pain. Our study suggests that our sonographic technique can locate fecal retention and assess the hardness or softness of fecal loading in adults, which can be helpful in selecting laxatives or enemas to treat the constipation. Furthermore, US can detect organic diseases (e.g., colonic cancer, ileus) that cause constipation. 25
The design of this study has some limitations. First, constipation could not be assessed adequately on US images alone. Because of the physiological phenomenon of fecal retention in the colon, no single test can adequately assess its pathophysiology. Comprehensive diagnostic evaluation is needed based on clinical condition and other examination findings. Second, US remains dependent on operator skill and technique.
Conclusions
This study has shown that transabdominal US can be used for qualitative assessment of fecal loading in the colon and is therefore suitable for follow-up examination. This technique is simple and noninvasive and can be used concomitantly with the physical examination to assess severity of constipation. It may offer an improvement over current assessment techniques.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.