
Abstract
Objective:
This study evaluated the significance of Doppler indices of the fetal aortic isthmus in diagnosing fetal hemodynamic disorders early. The aim was to determine the Doppler values within the fetal aortic isthmus in the third trimester of pregnancy.
Materials and Methods:
Patients who presented with pregnancies between 28 and 40 weeks of gestation were examined for Doppler indices of the fetal aorta and compared with the gestational age. Among these, 325 normal fetuses (mean gestational age, 25 weeks) were included in the study. The correlation between Doppler indices and gestational age was evaluated using regression equations. Linear, quadratic, and cubic models were applied to all the variables.
Results:
Curve estimation analysis showed that peak systolic velocity (R2 = 0.168), end-diastolic velocity (R2 = 0.042), pulsatility index (R2 = 0.101), and time-averaged maximum velocity (R2 = 0.090) correlated with gestational age (cubic model, p < .001). However, S/D, resistance index, and isthmic systolic index were not significantly correlated with gestational age. Notably, the R2 values were low for all variables.
Conclusion:
In this fetal cohort, the suggested normal reference values for Doppler indices based on gestational age in the third trimester of pregnancy were determined.
The fetal aortic isthmus (AoI) is a true arterial shunt that connects blood flow from the superior and inferior halves of the body in parallel circulation. 1 Positioned between the origin of the left subclavian artery and the end of the ductus arteriosus, it is the only connecting point in the parallel fetal circulation system. 2 In fetal circulation, the pulmonary and aortic circulations run in parallel, with the AoI as the sole link between the two circulations. Blood flow through the AoI is influenced by contributions from both ventricles: the left ventricle promotes forward flow, while the right ventricle induces backward flow. The net blood flow direction is influenced by these forces and the vascular impedance of the superior (cerebral) and inferior (systemic) circulation. 3 During gestation, the AoI undergoes dynamic changes owing to varying resistance in different parts of the fetal circulation. For instance, placental resistance stabilizes in the later stages of pregnancy, whereas cerebral resistance increases initially, peaks in mid-pregnancy, and then declines toward the end of pregnancy. 4 Studies of the Doppler pattern of the AoI show that around 25 weeks of pregnancy, a slight reversal in end-systolic flow begins, which gradually increases with gestational age. 5
The vascular properties of AoI make it a critical marker for assessing fetal hemodynamics because alterations in flow patterns may indicate compromised fetal well-being, especially in pathological conditions such as intrauterine growth restriction (IUGR) and congenital heart disease (CHD). 6 The Doppler potential of AoI as an indicator of the progression of fetal hemodynamic deterioration in fetuses afflicted with IUGR has been proposed, particularly as a short-term marker of adverse perinatal outcomes. Placental circulatory insufficiency can be detected earlier through AoI flow indices, 6 facilitating early intervention and delivery to prevent poor neurodevelopmental prognosis. 7 Physiological changes in AoI can be used to evaluate ventricular dysfunction in fetuses with left ventricular outflow obstruction. 3
Despite considerable research on AoIs in pathological pregnancies, limited research has been dedicated to the establishment of normal Doppler parameters for AoIs in healthy fetuses. Reference values for Doppler indices are essential to distinguish normal physiological changes from pathological conditions, particularly in the third trimester, when significant hemodynamic shifts occur. Normal reference ranges for AoI Doppler parameters would provide a valuable baseline for clinicians, allowing accurate assessment of fetal well-being and early detection of abnormalities. This study aimed to determine the Doppler parameters of the AoI and normal reference values of these parameters in healthy fetuses in the third trimester of pregnancy.
Materials and Methods
This cross-sectional study included pregnant patients who were referred to the hospital and training center for obstetrical sonography between April 20, 2020, and July 21, 2021. This study was approved by the Tabriz University of Medical Sciences Ethics Committee (IR.TBZMED.REC.1398.1109). The fetuses included in the study met the following criteria: (1) gestational age confirmed by a first-trimester sonogram; (2) the absence of structural anomalies; (3) normal fetal growth (weight between the 10th and 90th percentiles); and (4) a normal Doppler waveform obtained from the umbilical artery. The gestational age of the fetuses ranged from 28 to 40 weeks, with 25 fetuses evaluated for each gestational age, totaling 325 fetuses in the cohort. This is in accordance with similar studies, sample size, and the number of referred patients.8,9 Pregnant patients referred for sonographic evaluation who did not have medical conditions potentially affecting fetal hemodynamics (i.e., preeclampsia, hypertension, or cyanotic congenital/acquired heart disease) were enrolled and consented to participate in the study. Because the ultrasound equipment system was part of the hospital infrastructure and was approved for research use, the authors performed sonography free of charge. All sonograms were performed by a radiology resident trained in sonography and in recognizing fetal anomalies. The Affiniti 70 ultrasound equipment system (Philips, Amsterdam, The Netherlands) was used for the examination and was equipped with a convex transducer that operated at a frequency range of 2 to 5 MHz. A longitudinal aortic arch view was used to visualize the AoI. The technique used to obtain sonographic images of the fetal isthmus has been previously described. 8 The correct position of the sample volume (a few millimeters after the beginning of the left subclavian artery) was obtained for all fetuses (See Figures 1 and 2). After placing the cursors at proper locations, a spectral waveform was obtained (See Figure 3). The maximum sensitivity for the Doppler flow was adjusted such that the strongest color with the least number of artifacts was obtained. The Doppler insonation angle was maintained between 0° and 30°, and the sample volume was adjusted to a size that fitted within the large vessels of interest. Doppler waveforms deemed the most representative for each of the sonographic views were analyzed and printed.
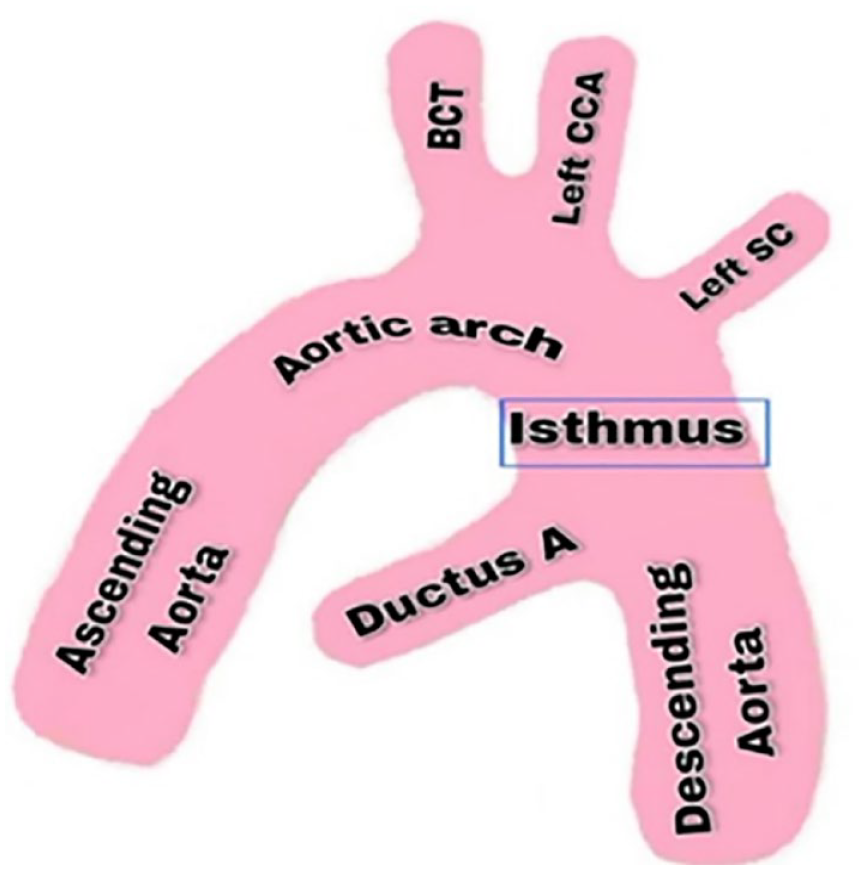
A schematic anatomical illustration to demarcate the aortic segments to record fetal aortic isthmus Doppler parameters.
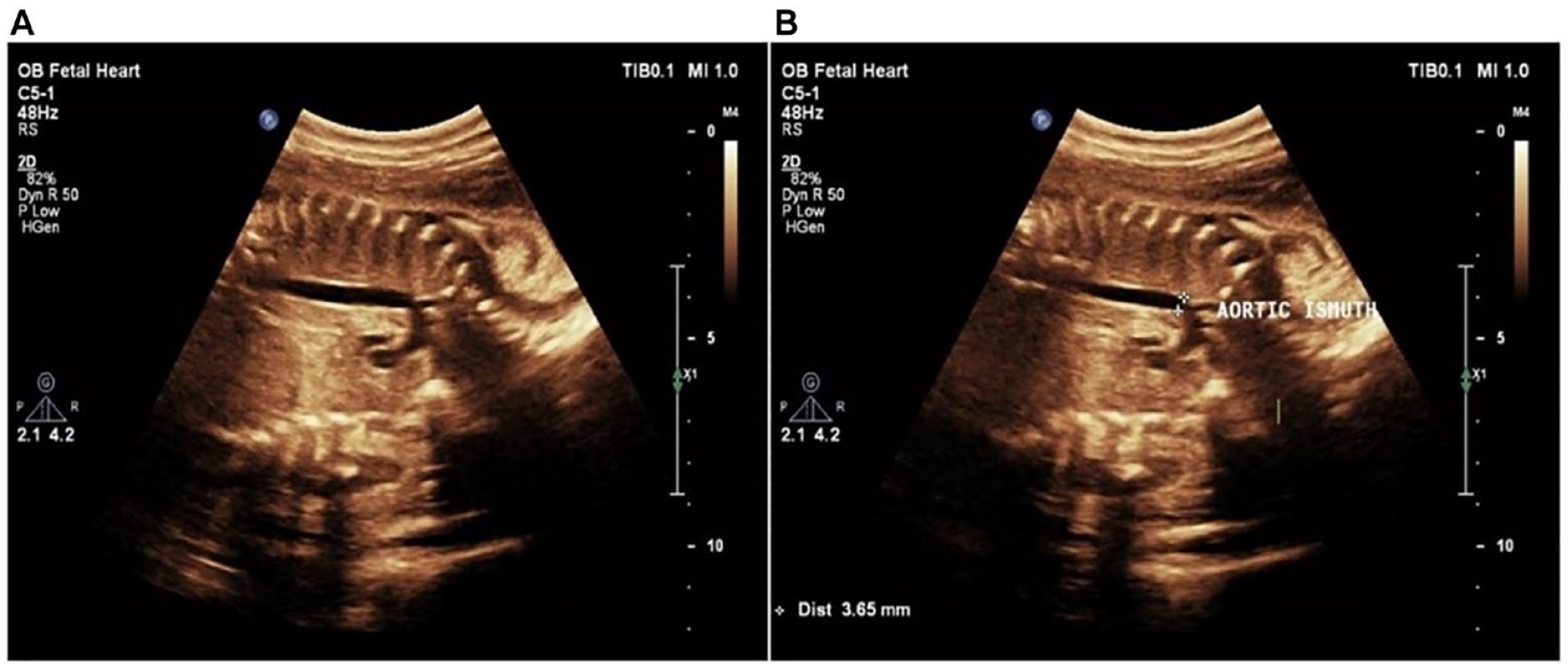
(A) An example sonogram is provided that illustrates the standard view used to check fetal aortic isthmus, along with Doppler parameters. (B) An example sonogram is provided that illustrates the standard view used to check fetal aortic isthmus. The Doppler parameters are recorded a few millimeters after the beginning point of the left subclavian artery (indicated by the cursors).
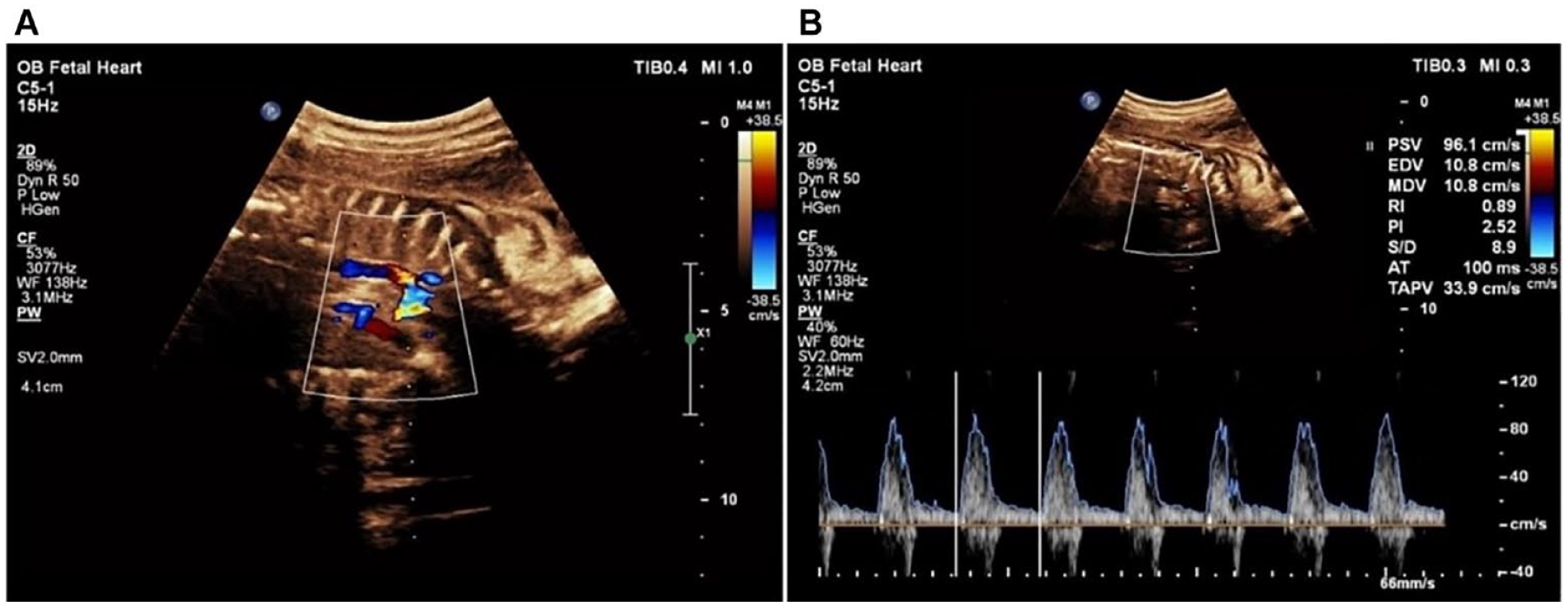
The measurement of Doppler parameters taken within the fetal aortic isthmus is demonstrated with color Doppler (A) and by the spectral Doppler cursor located at the aortic isthmus point (B).
The following parameters were measured for each of the conducted tests: peak systolic velocity (PSV), end-diastolic velocity (EDV), time-averaged maximum velocity (TAMXV), pulsatility index (PI), resistance index (RI), isthmic systolic index (ISI), 10 and systolic/diastolic ratio (S/D).
Royston and Wright’s statistical method 11 was used to evaluate the reference intervals. Linear, cubic, and quadratic regression models were chosen to estimate the association between AoI variables and gestational age, which were adjusted separately. The most appropriate model is selected for each variable. The level of statistical significance was set at p <.05, a priori. IBM SPSS software (v. 26; IBM Corp., Armonk, New York) was used for statistical analysis.
Results
In this cross-sectional study, 325 pregnant patients with a gestational age between 28 and 40 weeks of pregnancy consented to participate. Data for PSV, EDV, TAMXV, PI, RI, ISI, and S/D values across these gestational ages are presented in Table 1. The relationship between each variable and gestational age was studied using the Royston-Wright method. Linear, cubic, and quadratic regression models were drawn separately for each variable in order to determine the best model. Table 2 presents the results of polynomial regression analyses of the variables.
The Doppler Parameters Recorded for All the Fetuses Evaluated as Part of the Research Study.
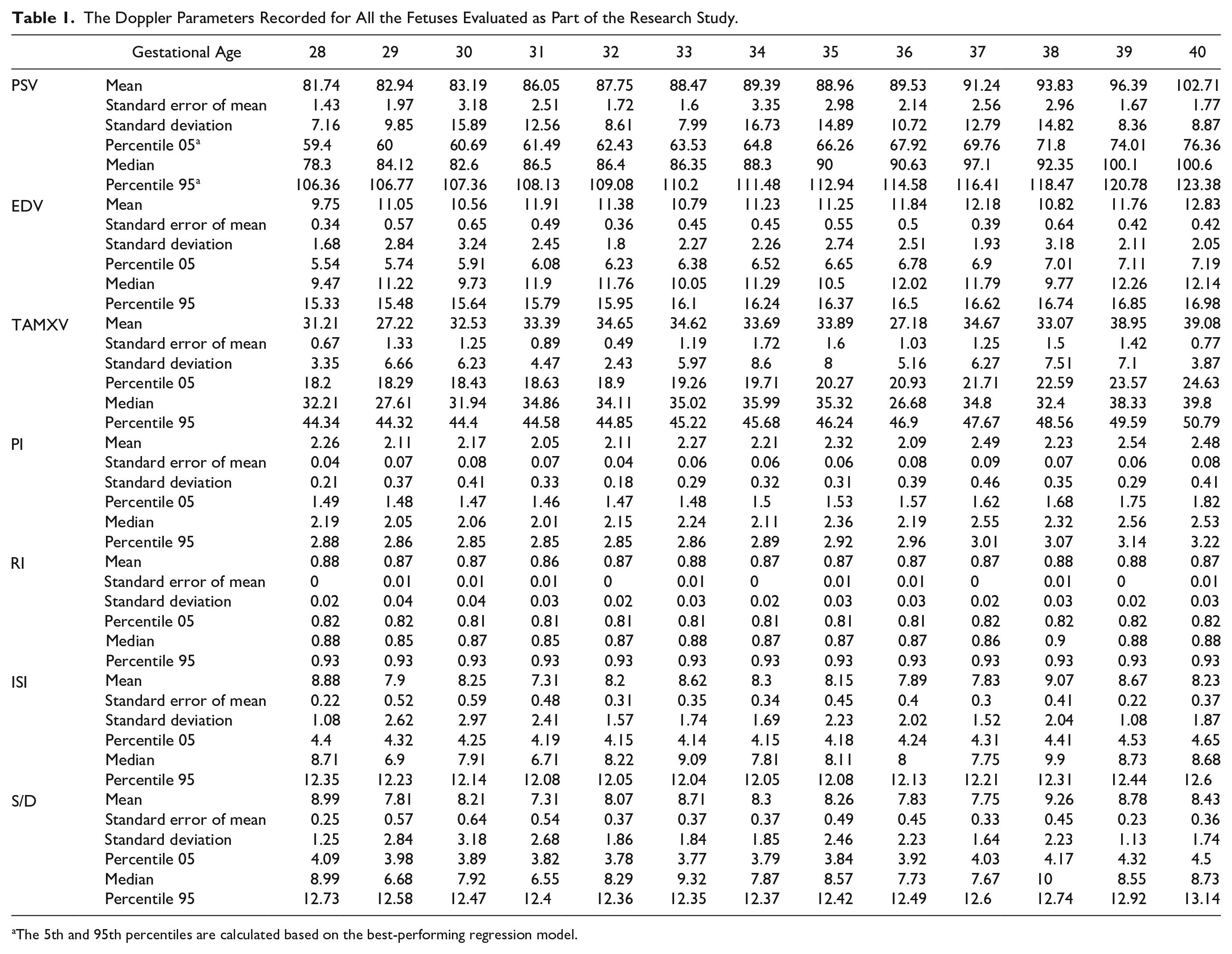
The 5th and 95th percentiles are calculated based on the best-performing regression model.
The Inferential Statistical Models That Were Run Based on the Mean Doppler Parameters Recorded on the Fetuses Evaluated, as Part of the Research Study.
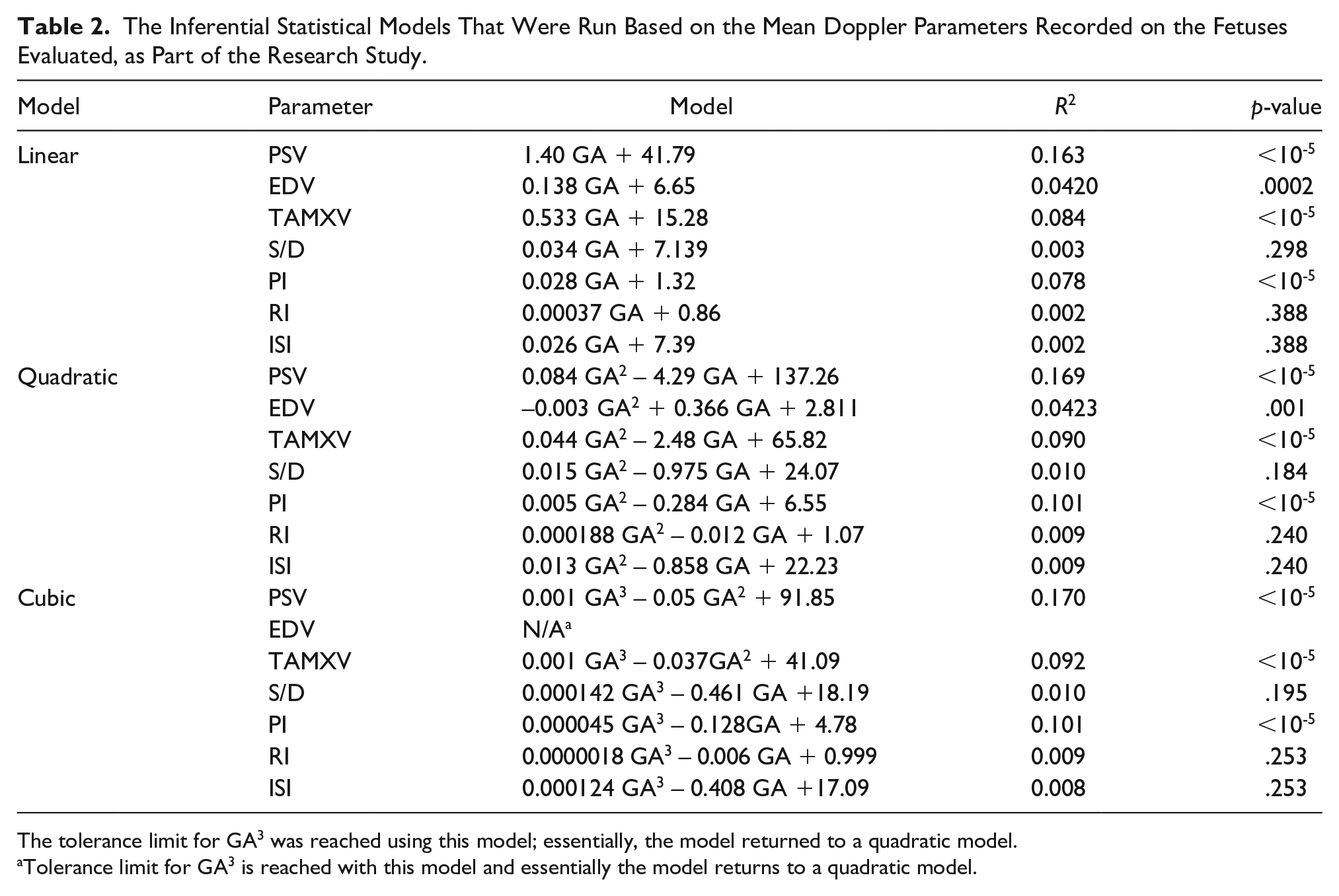
The tolerance limit for GA3 was reached using this model; essentially, the model returned to a quadratic model.
Tolerance limit for GA3 is reached with this model and essentially the model returns to a quadratic model.
As shown in Table 2, the PSV, EDV, TAMXV, and PI parameters were positively and significantly correlated with gestational age, with p-value below .05. Among these parameters, a linear relationship provided the best fit for PSV, EDV, and TAMXV. For the PI parameter, however, the relationship was quadratic, as the linear model was not significant. No significant relationships were observed for the ISI, RI, or S/D parameters.
Using the formulae obtained from each of the significant variables, a scatter plot of these variables was drawn (See Figures 4–10). The black line indicates the linear model, whereas the red and green lines indicate the quadratic and cubic models, respectively.
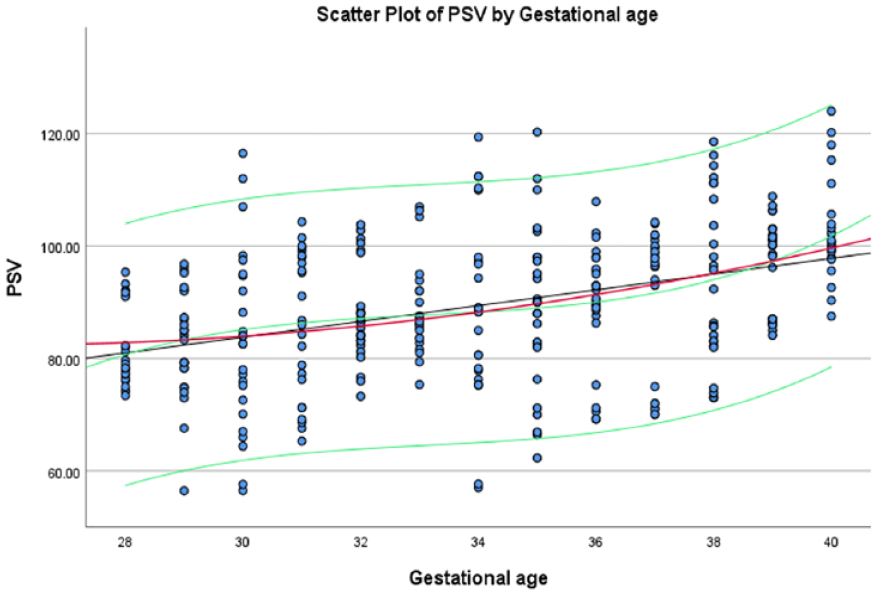
The average amount of PSV, within the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
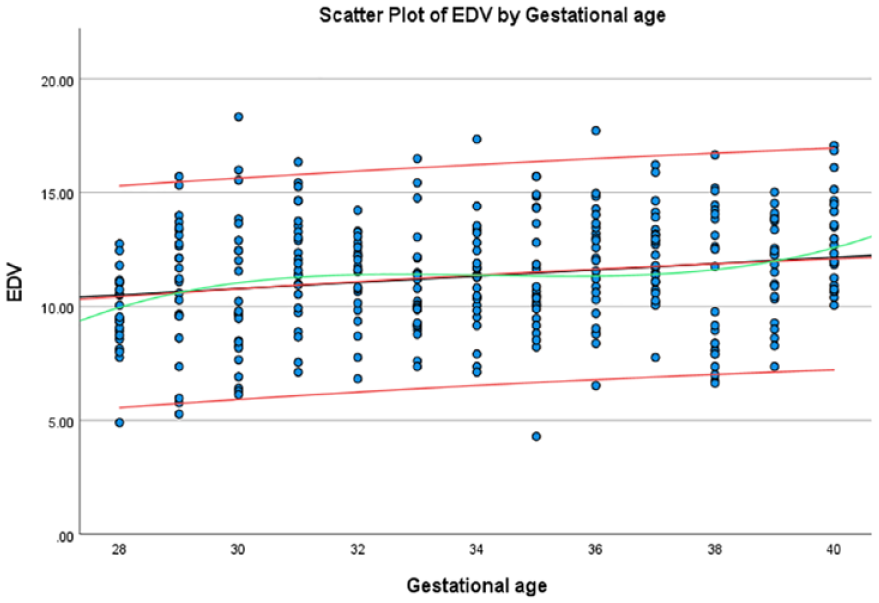
The average EDV, within the fetal aortic isthmus, based on the gestational age, at the estimated 5th and 95th percentiles.
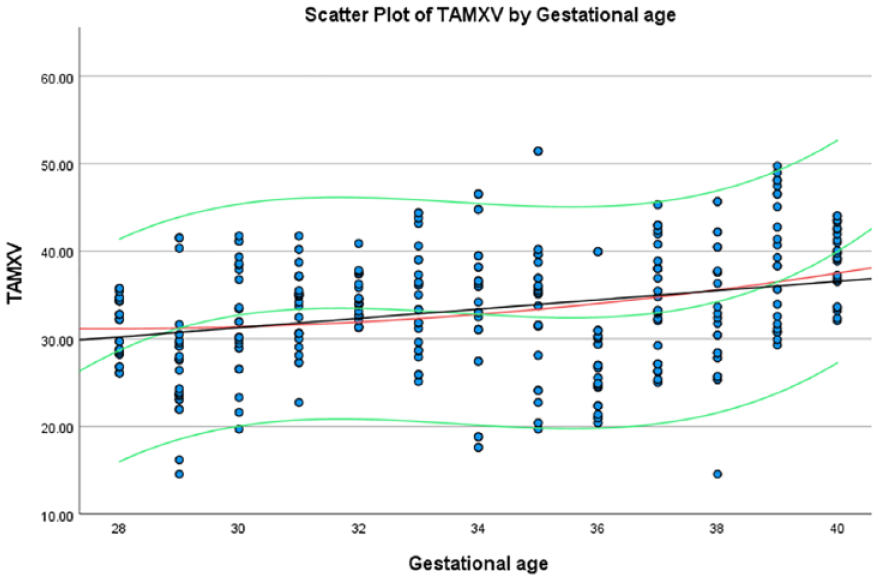
The average TAMXV, within the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
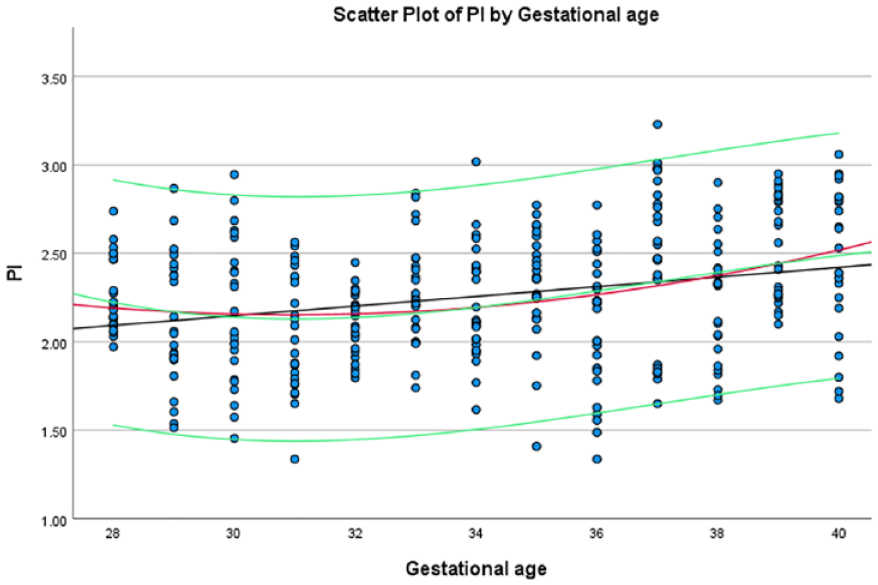
The average PI, within the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
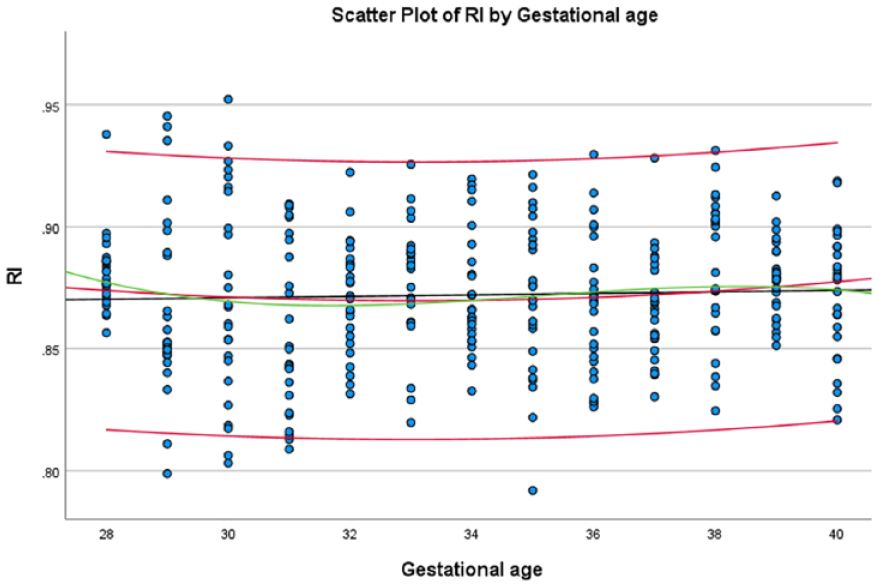
The average RI, within the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
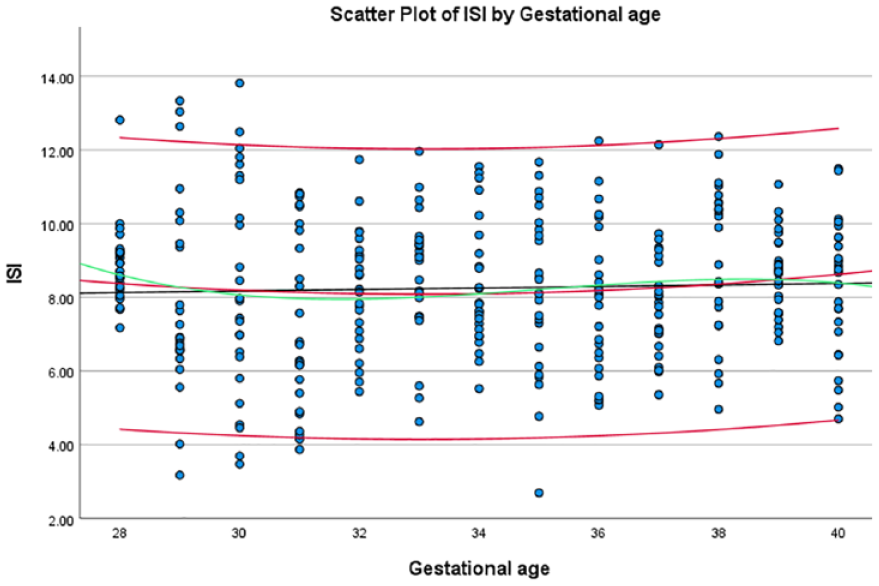
The average ISI, with the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
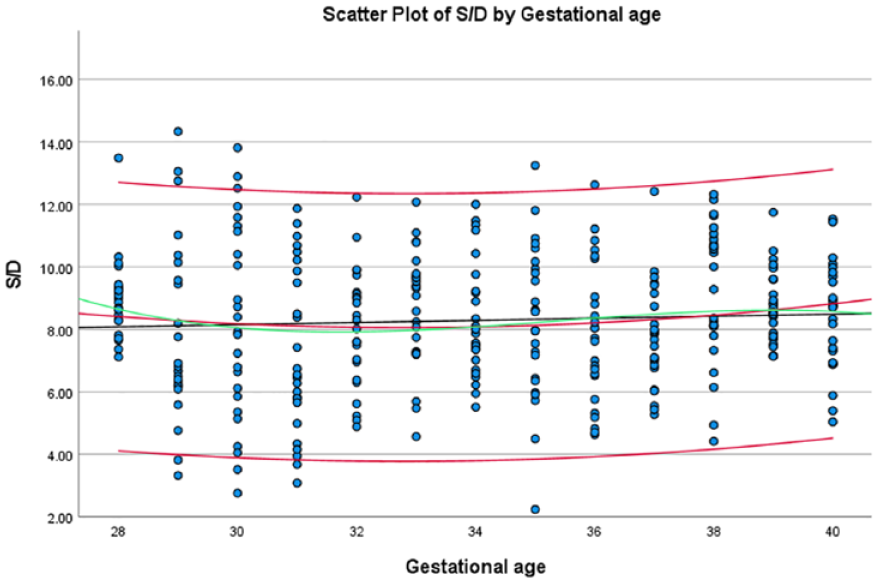
The average S/D, within the fetal aortic isthmus, based on gestational age, at the estimated 5th and 95th percentiles.
Discussion
This study examined the Doppler findings of AoI indices in healthy pregnancies to establish reference values.
Animal studies have also investigated the role of the AoI.12 –14 Despite the limitations of these studies, they demonstrated a strong positive relationship between the umbilical artery flow and AoI values when gradual pressure was applied to the umbilical vein. Studies in animal models have shown that, under conditions of reduced oxygenation, there is an increase in vascular resistance, which is observed in the form of different degrees of retrograde flow in the AoI. Studies on human samples have also demonstrated the utility of AoI Doppler for placental insufficiency.15,16 Several studies have shown that the AoI acts not only as a marker of fetal health but also as a predictor of perinatal outcomes. A strong association has been observed between reverse diastolic flow in the AoI and adverse pregnancy outcomes.7,17 –19 Studies have shown that retrograde flow of AoI is correlated with an increased risk of long-term neurodevelopmental deficit. 18
The Doppler pattern in the AoI is similar to that in other large arteries, in that a strong pulsating and forward systolic flow and a weak diastolic flow are observed. Interestingly, sustained diastolic flow was observed in the Doppler patterns of a significant number of fetuses in our study. Fouron et al. reported a short region of negativity at the beginning of diastole in patterns drawn from the aorta. However, this was rarely observed in this study. In addition, this finding was rarely seen in the 3VT view and mostly in the sagittal view, indicating that the 3VT view is more acceptable for examining the fetal aorta, as emphasized in previous studies. 5 A summary comparison of previous research and our results in terms of correlation is presented in Table 3.
A Comparison Table of the Current Research Parameters, Compared With Previous Research, in Terms of Correlation of Doppler Indices to Fetal Gestational Age.
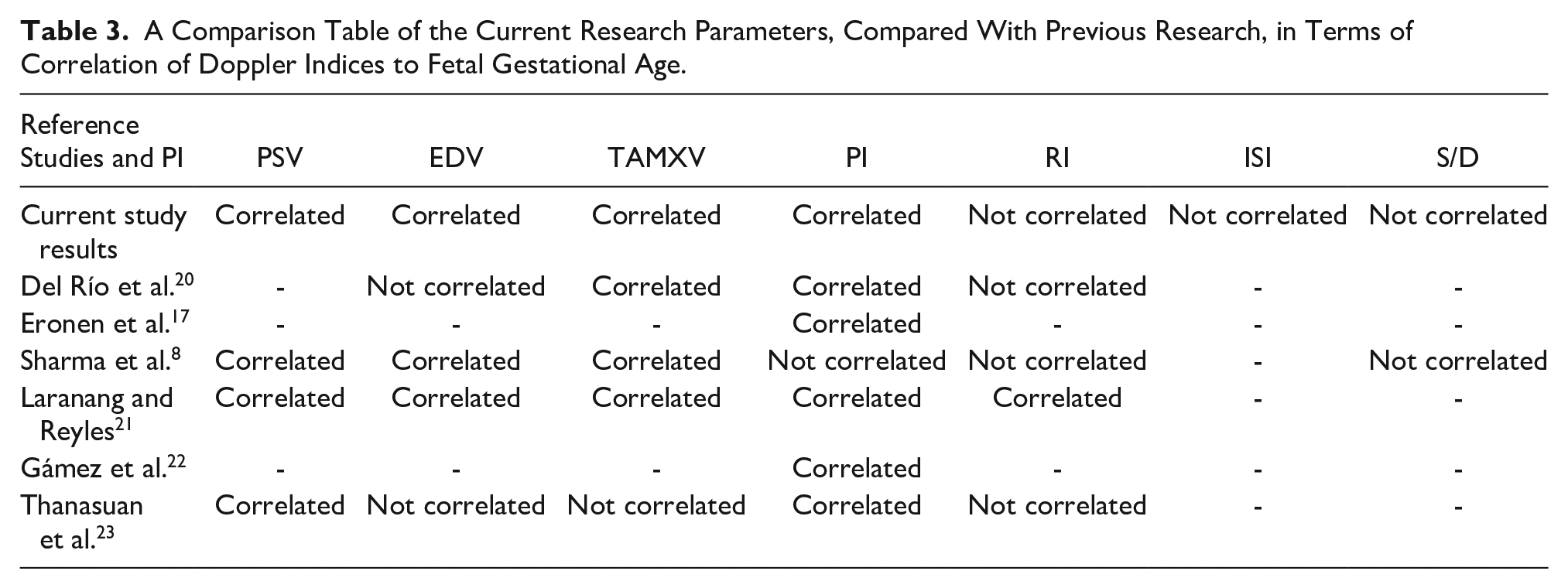
According to the regression calculations, PSV, EDV, TAMXV, and PI were significantly related to gestational age, whereas ISI, RI, and S/D were not. In a study by Del Río et al., 20 PSV, TAMXV, and PI demonstrated a significant correlation with gestational age, whereas RI did not, which is consistent with the current study results. However, they did not find a relationship between EDV and gestational age, which is inconsistent with our findings.
Eronen et al. 17 suggested that a slight increase in the PI with increasing gestational age can be explained by a decrease in the indices of the middle cerebral artery, which in turn can increase the PI in the AoI. By comparing the PI of the AoI and umbilical artery, no special correlation was observed between the two under fetal physiological conditions. This indicates that the physiological conditions of pregnancy do not affect fetal aortic indices, and both parameters can be used independently and together to monitor pregnancy.
Sharma et al.’s study of fetal aorta, Doppler between 27 and 40 weeks of pregnancy, revealed an upward trend and a significant positive linear relationship between gestational age and PSV, EDV, and TAMXV. However, there was no significant relationship between the RI, PI, and S/D findings and gestational age. These results regarding the non-significance of RI and S/D are similar to the findings of our study. However, unlike the current study, PI did not show a significant relationship in Sharma’s research. 8
In a study by Laranang and Reyles, 21 a significant positive relationship between PI and gestational age was observed, with an average PI of 2.4. PSV, EDV, TAMAXV, and RI also have positive but weak relationships with gestational age.
In a study by Gámez et al., 22 only the PI was measured. The amount of PI significantly correlated with gestational age in both singleton and twin fetuses. These findings are consistent with our results.
In a study by Thanasuan et al., 23 PI and PSV were significantly correlated with gestational age, which is consistent with the results of the present study, and no significant changes were observed in the RI, EDV, and TAMXV values.
This cross-sectional study provided normal reference values for fetal aortic Doppler parameters in healthy fetuses at 28 and 40 weeks of gestation. Physicians used a longitudinal view of the fetal aorta to obtain the Doppler parameters in the current study. In the literature, these values were successfully measured using any of the 3VV (3 Vessel View), 3VT (3 Vessel and Trachea view), or longitudinal views of the fetal aorta. Previous studies have also shown no significant differences between the values obtained from the aforementioned views. 22 However, in a study by Thanasuan et al., 23 the subclavian artery was more difficult to view in the 3VT view. In addition, the time required to measure the parameters in the longitudinal view of the aorta was shorter. In this study, a significant number of fetuses in late pregnancy had short-term reverse flow at the end of systole. 23 In the present study, reverse flow was observed in several fetuses at the end of systole, although this was not statistically significant.
During the fetal period, the AoI plays an important role in balancing blood flow between the brachiocephalic circulation, which supplies the head and neck, and the subdiaphragmatic circulation, which supplies the lower body and placenta. 23 Right and left ventricular systolic function, along with downstream vascular resistance, are key factors influencing the amount and direction of blood flow through the fetal AoI. The increase in circulating blood volume and gradual decrease in resistance in the middle cerebral arteries cause a gradual rise in the PI in the AoI as gestational age increases. 4
Conversely, PI is a continuous variable which according to the studies is also related to the consequences of pregnancy. 19 In advanced fetal and placental insufficiency, a change in the Doppler waveform of the fetal aorta occurs after a change in the waveform of the umbilical artery. Therefore, perinatal complications, including developmental and brain problems, cannot be prevented by simply using the Doppler waveform of the fetal aorta. 7 In this situation, the measurement of quantitative values such as PI and PSV can help prevent potential complications of fetal asphyxia at the time of birth. However, further studies are needed to compare quantitative and qualitative values.
Limitations
The major limitations of this study are attributed to its research design and the convenience-based patient sample, which pose threats to both internal and external validity. In addition, while the fetal isthmic flow index (IFI) has been used in some studies for semi-quantitative assessment of isthmic shunts, it was not routinely applied clinically in the host medical centers. Future studies should include investigations of IUGR fetuses and IFI. The results are based on patients from specific geographic area, meaning that ethnic and racial factors could impact findings. A larger, more diverse sample may provide more generalizable results across different populations. The results of the present study were comparable with the results of related research, but in some cases, there were discrepancies; therefore, repeating studies with larger statistical samples are recommended. Studies on fetuses with IUGR or other medical complications can help clarify the benefits of this type of sonographic evaluation in evaluating and predicting the prognosis of these fetuses.
Conclusion
The findings of the present study showed that fetal AoI Doppler parameters, including PSV, EDV, TAMXV, and PI, were significantly correlated with gestational age. Therefore, by using tables related to the upper and lower normal percentiles drawn for each of the variables, it is possible to compare the values measured in the patients so that effective steps can be taken toward the early diagnosis of uterine-placental blood supply disorders. Furthermore, considering that the present data were obtained from Iranian patients, they may be better matched to patients of the same race.
Footnotes
Acknowledgements
We would like to thank the Clinical Research Development Unit of Tabriz Valiasr Hospital, Tabriz University of Medical Sciences, Tabriz, Iran, for their assistance with this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1398.1109).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.