
Abstract
Low back pain is common during pregnancy, but symptomatic lumbar disc herniation in this period is particularly rare. We report a case of lumbar disc herniation in a 35-year-old woman at 32 weeks of pregnancy, who experienced persistent symptoms despite 6 weeks of rest and medication. Muscle strength in the right L5 nerve root declined to grade 4, and intravenous analgesia was ineffective. After thorough discussions with the patient and her family, a discectomy was performed under spinal anesthesia. Following surgery, the patient’s pain decreased, the Lasegue test became negative, and muscular strength returned to normal 2 weeks post-operation. At 39 weeks of gestation, a cesarean section was performed due to functional dystocia.
Teaching points
Challenges of spinal anesthesia in pregnancy: Spinal anesthesia was successfully utilized for discectomy in the third trimester of pregnancy.
Maternal and fetal monitoring: Careful monitoring of maternal and fetal health during and after surgery was essential to prevent complications.
Advantages of spinal anesthesia: This approach minimizes risks associated with general anesthesia, such as potential adverse effects on the fetus.
Treatment success: Discectomy under spinal anesthesia relieved the mother’s neurological symptoms without causing harm to the fetus.
Evidence review: This case, along with a review of the literature, serves as a model for safely managing similar conditions during pregnancy.
Introduction
Low back pain (LBP) is very common during pregnancy, reported in 56% of pregnant women, affecting one in two women. 1 Hormonal changes during pregnancy, such as increased secretion of progesterone and estrogen, along with the release of relaxin from the corpus luteum, lead to joint laxity, particularly in the sacroiliac and pubic symphysis joints. 2 These joints, along with the increased mechanical load of the uterus on the abdominal and paraspinal muscles, are recognized as the primary causes of LBP during pregnancy. 3 In addition, biomechanical changes, sagittal imbalance, and weight gain are also potential contributing factors. 4 Radiculopathy resulting from disk herniation during pregnancy is rare, occurring in ~1 in 10,000 pregnant women. 5 Surgical indications in pregnant women are similar to those in other patients. In cases where severe unilateral or bilateral radiculopathy, failed conservative treatments, or cauda equina syndrome (CES) are present, a surgical approach should be considered. 6 Therefore, the prompt recognition of certain emergency conditions during pregnancy is of high importance for physicians, and treatment should be initiated immediately, regardless of the stage of pregnancy. 7 Misdiagnosis or delay in treatment may lead to permanent neurological consequences. 8 Surgery in pregnant women requires more comprehensive management by a multidisciplinary team consisting of obstetric specialists, anesthesiologists, and specialized surgeons. 9 The main issue when operating on pregnant women is that the physician must care for two patients simultaneously: the mother and the developing child. 10 Therefore, any decision to intervene must balance the benefits and risks for both the mother and the fetus. 11 Performing spinal surgery during pregnancy is a significant challenge for physicians and must be carefully planned to achieve optimal outcomes with minimal risk to both the mother and the fetus. 12 There are important considerations that must be taken into account for pregnant women with lumbar disc herniation, particularly in situations where surgery is required. 13 These considerations include identifying which diagnostic tests and medications are safe during pregnancy, determining the ideal timing for surgery, evaluating surgical indications and techniques, selecting appropriate anesthesia, and managing the continuation of pregnancy following spinal surgery. 7 There are few reports in the scientific literature regarding these considerations, and currently, there is no established protocol for this condition. We present a case of a pregnant woman who underwent spinal anesthesia and discectomy in the left lateral position at 32 weeks of gestation.
Case report
A 35-year-old woman with a history of one vaginal delivery and one cesarean section presented with severe lower back pain accompanied by right-sided radicular pain starting at 25 weeks of gestation (Figure 1). She had experienced mild lower back pain during her previous pregnancies, which resolved without medical intervention or medication. Initially, she was treated with an analgesic (Tab sodium diclofenac 100) and bed rest at home. At this stage, a comprehensive baseline neurological examination was performed, including assessment of muscle strength using the Medical Research Council scale, which revealed mild muscle weakness graded 4 out of 5 in muscles innervated by the L4 and L5 nerve roots. Deep tendon reflexes, including the patellar and Achilles reflexes, were also evaluated. Sensory examination involved a detailed assessment of responses to light touch, pain, and temperature changes within the corresponding dermatomal distributions. In addition, the Lasegue test (straight leg raise) was utilized to assess sciatic nerve tension and irritation. The examination findings indicated mild neurological deficits, including slight muscle weakness and diminished light touch sensation in the L5 dermatome distribution. At 29 weeks of gestation, her pain worsened and did not respond to oral medications. The patient visited the emergency department several times, requesting intravenous analgesia (paracetamol 1 g), but her symptoms did not improve. Due to the severity of the pain and lack of response to medication, physiotherapy was not pursued at the patient’s request, as she preferred surgical intervention. Therefore, no physiotherapy was performed prior to surgery. Two weeks later, she presented to medical facilities with a positive Lasegue test and more pronounced neurological deficits, including reduced muscle strength (grade 4) in the right L5 nerve root. The Lasegue test was positive at 30°, and a 40% reduction in muscle strength was noted during right leg extension. 14 The Visual Analog Scale (VAS) score was reported as 10. 15 Magnetic resonance imaging (MRI) revealed a right-sided L4–L5 disk herniation. At the patient’s request, surgery was deferred until after delivery. However, due to the persistence of symptoms despite conservative treatments and severe, intolerable pain affecting the patient’s daily activities, surgery was scheduled. After consulting with the patient and her family, a discectomy was performed at 32 weeks of gestation. The patient was transferred to the operating room and positioned in the left lateral decubitus position to prevent abdominal compression. Special pads were placed under the chest area, around the abdomen, and under the legs. Using anatomical landmarks (iliac crest), the L4–L5 level was identified without fluoroscopy to avoid ionizing radiation exposure. The surgery was performed under spinal anesthesia with a 3.5 cm Whitacre needle at the L3–L4 interspace and the injection of 150 mg of bupivacaine. Fifteen minutes after the induction of anesthesia, the surgery began and lasted ~1 h and 20 min. A right-sided discectomy at the L4–L5 level was performed, and the extruded disk fragment was successfully removed. Throughout the surgery, all hemodynamic parameters were closely monitored, and no instability was observed in either the mother’s or the fetus’s condition. Fetal monitoring was conducted using Doppler ultrasound every 15 min during the procedure, with no changes in heart rate (140–160 beats/min) noted. After surgery, the patient was repositioned in the supine position, and heart rate and blood pressure were reassessed. If any signs of hypotension occurred, ephedrine was administered. Post-surgery, fetal heart rate (FHR) monitoring and ultrasound were normal. The patient was discharged on the fourth day postoperatively without pain in the right lower extremity. Following discectomy at 32 weeks of gestation and the patient’s full recovery, there was no need for postoperative physiotherapy, and the patient achieved a satisfactory level of functional status. Two weeks after surgery, the patient’s muscle strength returned to normal (Lasegue test negative), and the VAS score for pain was 1. Due to the sensitivity of the patient’s condition after surgery, only diclofenac 100 mg was used for severe pain. At 39 weeks of gestation, the patient underwent a cesarean section due to functional dystocia and delivered a healthy newborn weighing 3500 g. The Apgar score at 1 and 5 min was 10/10, and no complications were observed. Postpartum follow-up for back pain was conducted, and the VAS score was 0 at the second week and 1 month after delivery.

MRI showed a large disk herniation at L4/L5 expanded to the spinal canal more at 32 weeks of gestation. MRI: magnetic resonance imaging.
Discussion
This case report describes the management of lumbar disc herniation during pregnancy. Lumbar disc herniation in pregnancy is a rare phenomenon that has been reported in only a limited number of studies. Previous research has shown that performing a discectomy immediately after cesarean section in the third trimester can result in favorable outcomes without major complications.5,16 Surgical decision-making in pregnant women should be made with careful consideration of the patient’s clinical condition and the gestational age. 17 In addition, timely diagnosis and appropriate treatment selection are essential for improving maternal and fetal outcomes. 18 It is also recommended that anesthesia management aim to minimize risks to both the mother and the fetus. 19 Surgery should be reserved for urgent and severe cases and performed by a multidisciplinary team. 20 Microdiscectomy under local anesthesia and spinal block has been identified as a minimally invasive and safe approach for treating lumbar disc herniation in pregnant women. 21 Moreover, close collaboration among specialists and precise surgical timing are crucial to ensuring the safety of both the mother and the baby. 16 While most of these studies focus on diagnostic challenges and general management strategies for this condition during pregnancy, the present report specifically highlights lumbar discectomy under spinal anesthesia in the third trimester. In addition to presenting a unique case report, it also provides a comprehensive review of the existing literature on the subject.
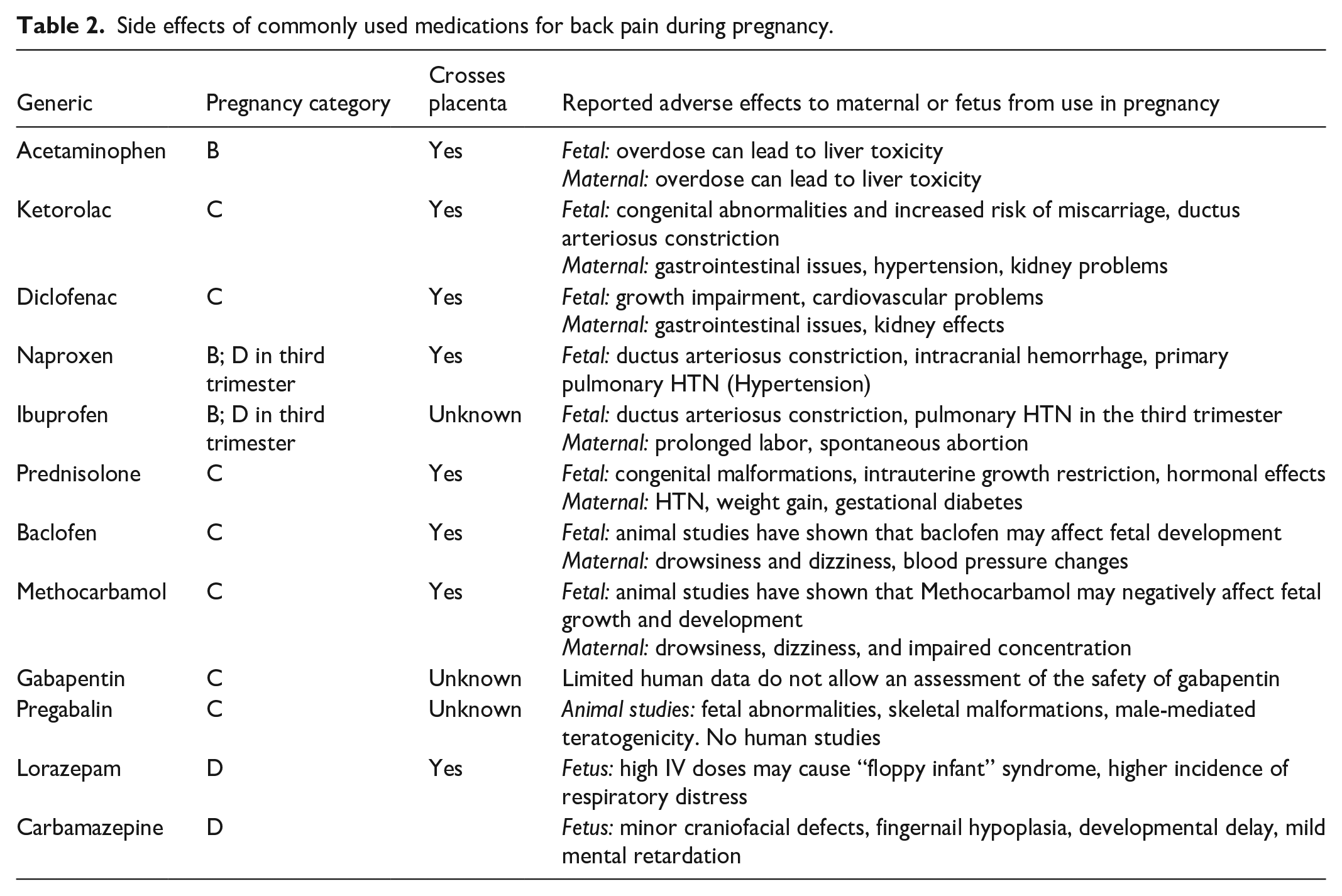
The decision-making process for managing lumbar disc herniation in pregnant and nonpregnant populations is generally similar when considering surgical versus nonsurgical treatment options. In both populations, the initial approach involves at least 6 weeks of conservative treatment, including physiotherapy, analgesics, and epidural steroid injections.3,7 The U.S. Food and Drug Administration classifies medications used during pregnancy into five categories: A, B, C, D, and X. This classification includes analgesics (non-opioid and opioid), anti-inflammatory drugs (steroidal and non-steroidal), muscle relaxants, and anticonvulsants (Table 1). Specifically, the categorization of commonly used drugs for the treatment of back pain during pregnancy is detailed in Table 2. 22 Although epidural steroid injections are effective in temporarily relieving symptoms and delaying surgery, there is insufficient evidence regarding their long-term benefits, and no clear consensus exists on their use for chronic LBP. 23 In pregnant women, physiotherapy interventions such as Pilates, yoga, walking, and movement control exercises have played an effective role in reducing LBP and pelvic girdle pain, as well as preventing work absenteeism. In addition, the use of approaches like technology-supported exercise therapy and the McKenzie method has expanded the scope of physiotherapy in managing these chronic conditions. 24
FDA risk classification for drug use in pregnancy.
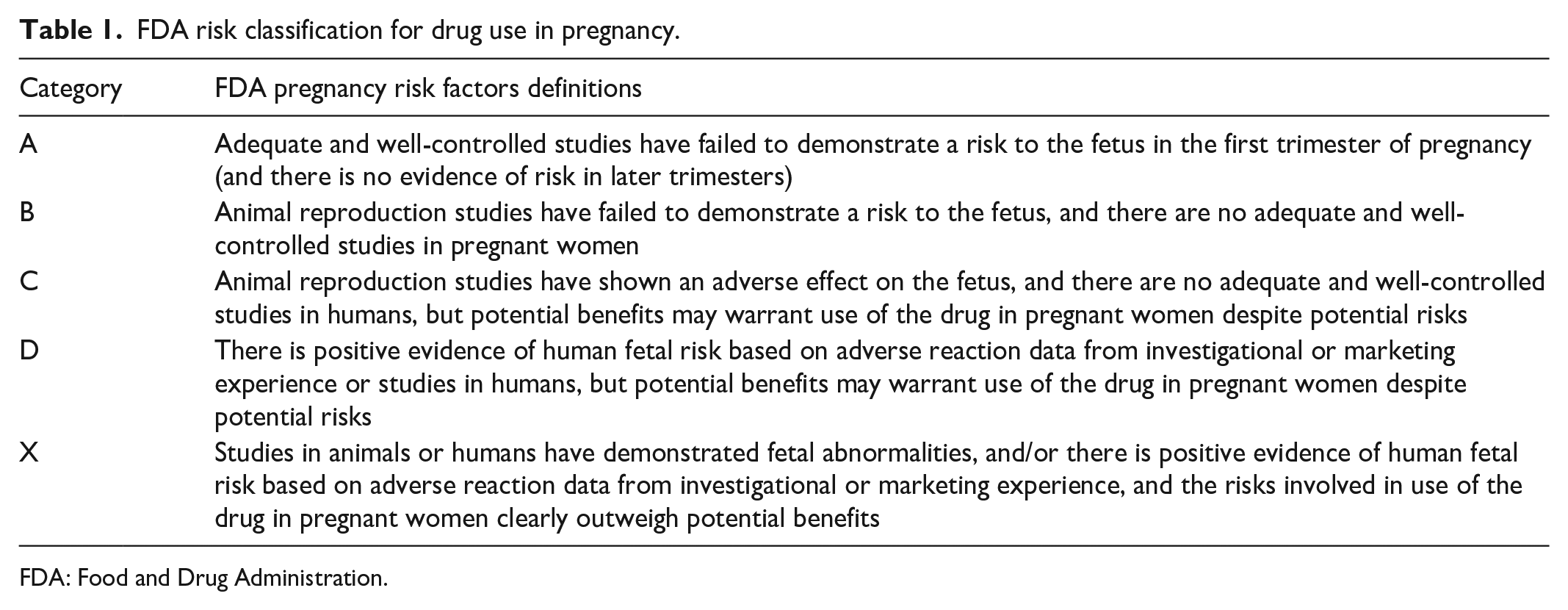
FDA: Food and Drug Administration.
Side effects of commonly used medications for back pain during pregnancy.
In addition, low-intensity aerobic exercises may be beneficial in symptom relief. 25 However, given the increased levels of the hormone relaxin during pregnancy, which can lead to increased joint flexibility, physiotherapists should avoid exercises involving wide ranges of motion. 26 Electrical stimulation and pulsed or continuous ultrasound should not be applied to the abdomen or lower back. 27
Differentiating physiological pregnancy-related back pain from lumbar radicular pain
Physiological back pain during pregnancy (caused by lumbar lordosis and ligament tension) typically presents as a dull or pulling pain in the lower back or pelvic region. This type of pain is often bilateral and ranges from mild to moderate in intensity. It usually improves with changes in position, rest, or movement. Neurological symptoms such as tingling, numbness, or weakness are not typically associated with this pain, and it most commonly occurs during the second and third trimesters. It is generally localized to the lumbar and pelvic areas and does not radiate to the legs.
In contrast, lumbar radicular pain is characterized by sharp, severe, and shooting pain that usually radiates from the lower back down to one leg. It is often unilateral and may be accompanied by neurological symptoms such as numbness, tingling, muscle weakness, or decreased reflexes. This type of pain may worsen with coughing, sneezing, or changes in posture, and can significantly limit mobility.28,29
Red flags
In pregnant patients presenting with back pain or radicular symptoms, the presence of certain warning signs may indicate serious neural compromise or other high-risk conditions. In such cases, immediate specialized evaluation and appropriate intervention are essential. These red flags include:
Significant weakness or numbness in the legs or genital area: This may indicate lumbar nerve root involvement or neurological dysfunction.
Loss of bladder or bowel control: This could be a sign of CES, a serious condition requiring urgent intervention.
Severe, persistent, and sudden-onset pain that does not improve with rest or position changes: This may point to serious compressive or inflammatory pathology.
Fever or other signs of infection: May suggest spinal or paraspinal infections, especially if accompanied by localized tenderness or pain.
Unexplained weight loss or a history of cancer: These signs may raise concern for metastatic lesions or systemic disease affecting the spine.
If any of these warning signs are present, it is critical to avoid delays in referral and diagnosis and to promptly refer the patient to a specialist center for further assessment and management.3,30
Diagnosis
One of the major concerns in managing pregnant women with spinal disorders is the exposure to ionizing radiation and its potential effects on the fetus. Ionizing radiation, which can be produced from sources such as radiography and tomography, can cause damage to DNA in cells, leading to fetal malformations. The teratogenic risk threshold for ionizing radiation is set at >0.05 Gy, with the highest risk observed during the first trimester of pregnancy. 31 MRI is recognized as the gold standard in diagnosing disc disorders for all patients (both pregnant and nonpregnant). 32 To date, no studies have confirmed the harmful effects of MRI during pregnancy. However, the American College of Radiology recommends avoiding this examination during the first trimester and abstaining from the use of contrast agents (such as gadolinium). 33 In cases where MRI is deemed essential in the first trimester, healthcare providers should conduct a thorough assessment of its risks and benefits, communicating this information transparently to the pregnant patient. Since decision-making in this context can significantly impact both maternal and fetal health, providing precise and reliable information is crucial.34,35 Given the critical role of neurological examination in diagnosing radiculopathy, careful and regular neurological monitoring should be emphasized. 36 Assessing motor strength, sensory changes, and reflexes aids in identifying nerve involvement and guiding treatment decisions. 37 This is especially important during pregnancy when imaging options are limited. Early detection through clinical exams can improve outcomes and prevent irreversible damage. 38 Historically, myelography and computed tomography were used for diagnostic purposes. However, both of these methods pose significant risks to the developing fetus due to exposure to ionizing radiation. 39 Currently, MRI and ultrasound are preferred imaging techniques for physicians. Nonetheless, the implications of using contrast agents must be carefully evaluated, especially when their use is deemed necessary. 40 Animal studies have shown an increased rate of miscarriage, skeletal abnormalities, and visceral malformations, particularly when dosages administered are two to seven times higher than the recommended dose for humans. 41 Furthermore, it remains unclear whether these compounds are excreted in human breast milk. If secreted, the infant may be exposed to unwanted side effects such as developmental disorders, gastrointestinal problems, or neurotoxic effects, which could jeopardize the infant’s health and normal growth. 42 Overall, the use of these agents should only be permitted during pregnancy in situations where their benefits significantly outweigh the potential risks. 4 Evidence from animal studies indicates that if there is a need for exposure to higher doses of radiation through fluoroscopy during a procedure, it is advisable to consider pregnancy termination before the procedure in the first trimester and early second trimester or to opt for cesarean delivery before the procedure in the late second and third trimesters. 32
Surgical indication
Management of spinal disorders during pregnancy is of paramount importance, particularly in cases of persistent LBP and radicular pain that do not respond to conservative treatments. In such instances, surgical intervention may be deemed necessary. Scientific evidence indicates that pregnancy at any stage does not preclude the possibility of surgical interventions. However, special attention must be given during surgery to safeguard the health of both the fetus and the mother from potential risks. 11 Common surgical methods for treating lumbar disc herniation in pregnant patients include laminectomy and/or microdiscectomy. In addition, endoscopic discectomy has been reported during pregnancy; however, the use of fluoroscopy and ionizing radiation in this procedure may pose greater risks to the fetus. 3 The absolute indications for discectomy during pregnancy are similar to those for other patients, and in cases such as CES or progressive neurological dysfunction, delays in performing surgery can lead to serious and irreversible consequences. 43 Common surgical procedures performed during pregnancy include ovarian cyst removal, breast biopsy, appendectomy, and trauma-related surgeries. 13 A study conducted by Okeagu et al. indicates that the rates of congenital anomalies and stillbirths in pregnant patients undergoing nonobstetric surgery are comparable to those in patients who have not undergone any surgical procedures. 44 In general, elective surgeries during pregnancy are not recommended, especially in the first trimester. However, the second trimester may be a more appropriate time for such surgeries. In emergency cases, such as acute abdomen, malignancies, or neurological and cardiovascular surgeries, the preservation of the mother’s life should take precedence.
Follow-up strategy for pregnant patients undergoing discectomy
Visit frequency
Based on clinical experience and current expert opinion, follow-up visits may be scheduled every 2–4 weeks during the first and second trimesters after surgery, depending on symptom severity and obstetric risk factors. As the third trimester approaches, visits could become more frequent (every 1–2 weeks) to allow for closer monitoring of maternal and fetal well-being. However, specific visit intervals should be individualized as evidence-based guidelines are currently lacking.
Maternal evaluation
Each visit is suggested to include a thorough neurological examination to assess muscle strength, sensory deficits, and reflexes, although standardized protocols are not yet established. Pain severity can be evaluated using validated scales, and the patient should be observed for signs suggestive of surgical complications, such as infection or neurological deterioration. These recommendations are primarily informed by clinical practice rather than high-level evidence.
Fetal monitoring
Routine ultrasound assessments are generally considered appropriate to monitor fetal growth and amniotic fluid volume. In the third trimester, or if concerning maternal or fetal symptoms arise, the use of non-stress tests or cardiotocography may be considered based on obstetric judgment. In addition, Doppler studies could be utilized when indicated to assess placental and fetal circulation. These recommendations are aligned with current obstetric practice, though specific evidence in post-discectomy pregnant patients remains limited.
Additional imaging
In cases of worsening neurological symptoms, MRI is regarded as a safe imaging modality for both mother and fetus, offering detailed anatomical assessment without ionizing radiation. While MRI safety during pregnancy is well-established, the decision to perform imaging should always consider the clinical context.
Medication and multidisciplinary management
All medications should be prescribed cautiously, with consideration of available safety data in pregnancy. Close collaboration among obstetricians, neurologists, anesthesiologists, and spine surgeons is strongly recommended, as multidisciplinary care appears to provide the best outcomes in complex cases like these. However, formal evidence supporting specific management algorithms remains scarce.
Delivery planning
Delivery planning for women who have undergone a discectomy during pregnancy requires individualized assessment, as there is currently no consensus or standardized guideline for such cases. A comprehensive evaluation of the mother’s neurological and physical status may assist in determining whether vaginal delivery is feasible or if cesarean section might be a safer alternative. Factors such as pain control, muscle strength, spinal stability, and risk of neurological exacerbation during labor should be carefully weighed. In instances of significant neurological deficits, cesarean delivery could be considered to minimize mechanical stress on the spine. Nonetheless, for patients with stable neurological function, vaginal delivery may be pursued under close monitoring by an experienced multidisciplinary team.
General role of physiotherapy during pregnancy
Physiotherapy is commonly recognized as an important supportive treatment for pregnancy-related LBP. Interventions such as gentle stretching, muscle strengthening exercises, hydrotherapy, and postural education may help alleviate symptoms and improve functional capacity, although high-quality studies in this subgroup are limited.
Types of physiotherapy and appropriate positions
Physiotherapy approaches typically include gentle stretching, strengthening exercises, hydrotherapy, and posture correction.
Positions such as left lateral decubitus (lying on the left side), supported sitting, and standing are generally considered safe during pregnancy.
Supine positioning (lying on the back), especially after the first trimester, is generally avoided to minimize pressure on the inferior vena cava.
In addition, wide-range or intense movements should be avoided due to pregnancy-associated ligament laxity, though further research is needed to define precise activity limitations.
Positioning
The selection of an appropriate position during lumbar disc surgery in pregnant patients is of paramount importance. The prone position is generally suitable for all trimesters of pregnancy and is predominantly utilized during the first and second trimesters. In the third trimester, specialized cushions are recommended to alleviate any abdominal pressure. 45 The American College of Obstetricians and Gynecologists emphasizes that the prone position provides optimal surgical access while minimizing venous epidural pressure, thereby reducing blood loss. However, extra caution is required when employing the prone position for pregnant women during surgical procedures, as excessive pressure may lead to preterm labor. During the first trimester and early second trimester, discectomy can be performed in the prone position, as there is reduced pressure from the gravid uterus on the aorta and inferior vena cava. 46 After 12 weeks of gestation, the left lateral decubitus position is advised to prevent compression of the aorta and inferior vena cava. Achieving the prone position in the third trimester becomes challenging due to the anatomical changes associated with pregnancy. 47 When performing surgery during this stage, it is crucial to determine whether the pregnancy will continue, leading to discectomy in the left lateral position, or whether the pregnancy will conclude with delivery, allowing for discectomy in the prone position 45 (Figure 2). If the first option is chosen, the pregnancy may continue, and delivery can occur until term. However, this surgical approach may become technically more complex, potentially increasing the burden on both the fetus and the mother. Conversely, if the latter option is selected, there is no need to consider the impact of the procedure on the fetus during surgery, permitting the use of the prone position. Nonetheless, in cases of preterm labor, there is an elevated risk of complications, including those related to respiratory system dysfunction. 48

Surgical protocol for lumbar disc herniation during pregnancy, showing recommended patient positioning according to different gestational weeks to optimize surgical access and maternal–fetal safety.
Anesthesia
Anesthesia management during pregnancy requires a different approach due to the specific anatomical and physiological changes occurring during this period. General anesthesia can disrupt placental perfusion by increasing catecholamine levels, placing the fetus at risk for hypoxemia or asphyxia due to reduced uterine blood flow. 49 In addition, this type of anesthesia may be associated with side effects such as excessive mechanical ventilation, maternal hypoxia, cardiovascular depression, and exposure to teratogenic drugs. 50 Research indicates that nearly every medication used in this context may have teratogenic properties. Due to ethical considerations, studies on drug transfer through the placenta in humans are challenging, and animal models also have limitations due to anatomical differences. 51 Airway management in pregnant women can be complicated due to increased thoracic wall diameter and breast enlargement. These patients generally require less anesthetic medication, as the minimum alveolar concentration in this population is reduced, and hormonal changes make them more sensitive to local anesthetics. Furthermore, due to anatomical changes, pregnant women are at greater risk for aspiration of gastric acid during anesthesia induction, as the tone of the lower esophageal sphincter is decreased.50,52
Spinal anesthesia is an effective method in obstetric surgery, significantly reducing the potential risks of failed intubation and aspiration, particularly in the third trimester of pregnancy. This prevention is attributed to the anatomical changes that occur during pregnancy, necessitating specific considerations in anesthesia management.45,53 Furthermore, spinal anesthesia can largely mitigate the teratogenic effects of anesthetic drugs on the fetus. This technique allows the mother to maintain her airway and, through spontaneous breathing, provides a clearer field of view due to reduced bleeding. 54 In fact, spinal anesthesia leads to a decrease in intrathoracic pressure, resulting in less dilation of epidural veins, which in turn reduces the overall blood loss. Both general anesthesia and spinal anesthesia have been successfully employed in obstetric surgeries; however, previous studies have not demonstrated a clear superiority of one technique over the other. 55 The choice of the appropriate anesthesia method depends on the specific conditions of each patient and the recommendations of the medical team. Therefore, thorough clinical assessment and consultation with anesthesia specialists are essential for informed decision-making. 49
Fetal monitoring
Lumbar disc surgery, particularly in pregnant women, requires special attention to the health of both the mother and the fetus. Fetal monitoring during such surgical procedures is of paramount importance, as any changes in the mother’s condition can directly affect fetal well-being. Fetal monitoring during lumbar disc surgery allows healthcare providers to closely observe the status of the fetus and promptly identify any abnormalities or changes.4,56 Utilizing electronic monitoring systems, healthcare providers can continuously track fetal vital signs, including heart rate, movements, and responses during surgery. 57
Monitoring methods
Cardiovascular monitoring: The use of Doppler ultrasound and FHR monitors enables healthcare providers to continuously assess the fetal heart status. These methods can indicate any stress or risks to the fetus.
Echocardiography: In some cases, echocardiography is employed for a more detailed evaluation of the fetal heart and to identify potential abnormalities.
Response to anesthetic agents: Monitoring changes in FHR and responses to anesthetic drugs is another critical aspect of fetal monitoring in this context. Some anesthetic agents can affect fetal heart function; therefore, they must be used with caution. 58
Specific conditions and challenges of this period. When these surgeries are performed by experienced multidisciplinary teams, the safety profile is very high, and complications in pregnant women are generally comparable to those in other patients. 59 With the use of advanced surgical and anesthetic techniques, maintaining pregnancy is often feasible, even in the third trimester. Therefore, delaying surgery for disc herniation in pregnant women experiencing severe leg pain or neurological deficits due to concerns about negative outcomes is unnecessary. The primary focus should be on ensuring the safety of both the mother and the fetus during surgery. 4
Recommendations and key considerations for pregnant women who undergo discectomy during pregnancy
Before delivery
Close monitoring of maternal and fetal well-being throughout the remainder of the pregnancy may be beneficial, particularly in patients with ongoing neurological symptoms or obstetric risk factors.
During rest and medical procedures, it is generally recommended to avoid excessive abdominal pressure; positioning in the left lateral decubitus position appears to be a safe approach based on clinical experience.
Pain management should be carefully individualized, with a focus on using medications that are considered safe during pregnancy, although treatment plans must be tailored to the patient’s specific needs and under specialist supervision.
Gradual resumption of physical activity may be considered, depending on the patient’s tolerance, while avoiding strenuous exercises or wide-range movements until medically cleared.
Routine prenatal visits and fetal monitoring are important to ensure early detection of potential complications as part of standard obstetric care protocols.
After delivery
Early postpartum follow-up is recommended to assess surgical recovery and pain status, although the exact timing and frequency should be individualized.
If no contraindications are present, initiating physiotherapy may assist in muscle strengthening, posture correction, and functional recovery.
Breastfeeding is generally considered safe after discectomy; however, all medications should be reviewed for lactation safety on a case-by-case basis.
A gradual return to daily activities could be advised, while heavy lifting and sudden movements should be avoided during the early recovery period.
Providing psychological support might also be beneficial in helping patients manage stress related to surgery and pregnancy, although further research is needed to establish formal recommendations in this context.
Conclusions
According to existing evidence in the literature, spinal surgery during pregnancy may be a safe option with minimal risk for both the mother and the fetus under specific conditions. Decisions in this regard should be made through careful consultation and comprehensive clinical evaluation by multidisciplinary medical teams to achieve the best possible outcomes. This approach not only enhances safety during pregnancy but can also help improve the patient’s quality of life.
Strengths and limitations
One of the strengths of this case report is the detailed presentation of the diagnostic process, clinical decision-making, and management of lumbar discectomy performed under spinal anesthesia during the third trimester of pregnancy. This report also highlights the importance of choosing spinal anesthesia and placing the patient in the left lateral position, which is crucial for ensuring the safety of both mother and fetus during pregnancy. Furthermore, the accompanying literature review provides a comprehensive framework for better understanding similar treatment options in pregnancy.
However, as a case report, the findings presented here cannot be generalized to the broader population, and definitive conclusions for all pregnant patients with lumbar disc herniation cannot be drawn. In addition, the lack of long-term follow-up after delivery is a major limitation in evaluating the extended outcomes for both the mother and the newborn.
Footnotes
Ethical Considerations
Ethical approval was obtained from the Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1404.115). This case report was conducted in accordance with ethical standards and relevant institutional guidelines.
Consent to Participate
Written informed consent was also obtained from the patient for participation in the study.
Consent for Publication
Written and informed consent was obtained from the patient for publication of this case report and accompanying images. No personally identifiable information has been included in the article.
Author Contributions
P.H. contributed to patient examination and drafting of the initial manuscript. A.M. is responsible for data collection and literature review. F.S. contributed to the interpretation of clinical findings and critical revision of the manuscript. All authors read and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Vice-chancellor for Research and Technology, Hamadan University of Medical Sciences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.