
Abstract
Impetigo herpetiformis is a rare skin disease that most often occurs in the third trimester of pregnancy. It is currently considered as a form of generalized pustular psoriasis and the typical skin lesions comprise small sterile pustules. Here, a case of impetigo herpetiformis in the second trimester of pregnancy after 7 weeks of hydroxychloroquine administration for suspected Sjogren's syndrome is reported. Treatment with anti-infective, anti-inflammatory and immunosuppressive medication did not improve the patient’s condition. Following delivery of a live male by emergency caesarean section at 29 weeks’ gestation, the rash was reported to be completely resolved by 3 months postpartum. Previously published cases of impetigo herpetiformis in the second trimester of pregnancy that were retrieved from a search of the PubMed database are also reviewed and discussed.
Keywords
Introduction
Impetigo herpetiformis is a rare skin disease that usually occurs in the third trimester of pregnancy and may resolve spontaneously after termination of pregnancy. It is currently considered to be a form of generalized pustular psoriasis, despite the previous opinion illustrating impetigo herpetiformis to be a separate entity. 1 Kamiya et al. 2 reported 15 287 cases of psoriasis during 2013–2018 in patients enrolled into the Japanese Society for Psoriasis Research (JSPR) annual epidemiological survey, and 291 cases of pustular psoriasis during 2017–2021 in patients enrolled into the JSPR annual epidemiological survey. 3 An epidemiological study in China, based on Urban Basic Medical Insurance data (2012–2016), found that the prevalence of generalized pustular psoriasis in 2016 was approximately 1.4/100 000 person-years. 4 Sporadic cases and limited systematic data are reported elsewhere. Typical skin lesions appear as clusters of small aseptic pustules on the basis of erythema, and systemic symptoms are severe, potentially involving heart and kidney failure. Secondary sepsis may also occur. Impetigo herpetiformis may cause placental insufficiency, resulting in fetal intrauterine growth retardation, and may also cause premature rupture of fetal membrane, premature birth, stillbirth and other factors endangering the life of mother and fetus. 5 No treatment guidelines currently exist. Here, a case of impetigo herpetiformis after hydroxychloroquine administration, with disease onset at the 26th week of gestation, is reported. In addition, cases of impetigo herpetiformis in the second trimester of pregnancy that were previously published in the PubMed database have been reviewed and summarised.
Case report
Written informed consent to treatment and to publication of the case was obtained from the patient. All patient details have been de-identified and the reporting of this study conforms to CARE guidelines. 6
A multiparous woman in her early 30 s (gravidity 2, parity 1), at 27 weeks of pregnancy, was admitted to hospital in October 2022, due to a rash with itching all over her body for 9 days (onset at week 26 of gestation). Large erythematous and maculopapular rash appeared on her abdomen, which was scaly and itchy, and then rapidly spread to her chest, back, and limbs. She had no fever, palpitation, chest tightness or other discomfort. At 2 days after admission, fever started at 38.1 °C, the rash developed further, turned a deeper purple colour, and small clusters of pustules began to form, with multi-ring damage on the limbs. By day 13 of hospital admission, the fever continued and the rash continued to develop. Systemic skin lesions exceeded 95%, there were new small pustules, some of which gathered into pus-filled lakes, and some of the skin was broken with increased swelling and pain (Figure 1).

Images from a patient in her early 30 s who presented after developing rash with itching all over the body at the end of the second trimester of pregnancy, showing: (a and b) erythema and maculopapular rash with large scales on admission; (c, d and e) small clusters of pustules, multiring damage and pus-filled lakes on the limbs after admission; (f and g) pinpoint-sized clusters of small pustules located on the abdomen and back; and (h and i) areas of broken skin with increased swelling and pain before caesarean section.
A local hospital suspected the patient of having Sjogren's syndrome during the first trimester of her pregnancy, and she was prescribed 200 mg hydroxychloroquine, orally, daily, starting from 19 weeks of pregnancy. However, a rash appeared, and hydroxychloroquine was discontinued on the third day after rash onset. She had a medical history of two pregnancies and one delivery, and her last menstrual period was in April 2022. She reported no history of food or drug allergies, or psoriasis, and no family history of diseases. After hospital admission in October 2022 (week 27 of gestation), her inflammatory markers were significantly increased above normal range, including erythrocyte sedimentation rate (108 mm/h), C-reactive protein (43.84 mg/L), white blood cell count (11.22 × 109/L [neutrophils, 90.30%]) indicating leucocytosis, and procalcitonin (0.13 ng/ml). Other laboratory parameters revealed hypokalaemia and hypocalcaemia (serum calcium, 2.05 mmol/L), positive rheumatoid factor (72.0 kU/L), positive antinuclear antibody (ANA) reaction (+) with a titer of 1: 640 and nuclear granular type karyotype, positive anti-Sjogren's syndrome-related antigen A (SSA)/Ro antibody (+++), positive anti-Ro-52 (+++), and increased levels of immunoglobulin (Ig)G and IgA. Obstetrics colour Doppler ultrasound showed a single live fetus and low-lying placenta. Fetal heart colour Doppler ultrasound revealed a slight regurgitation of the fetal tricuspid valve. Skin biopsy showed pustules mainly composed of neutrophils in the stratum corneum and spinosum (Figure 2).
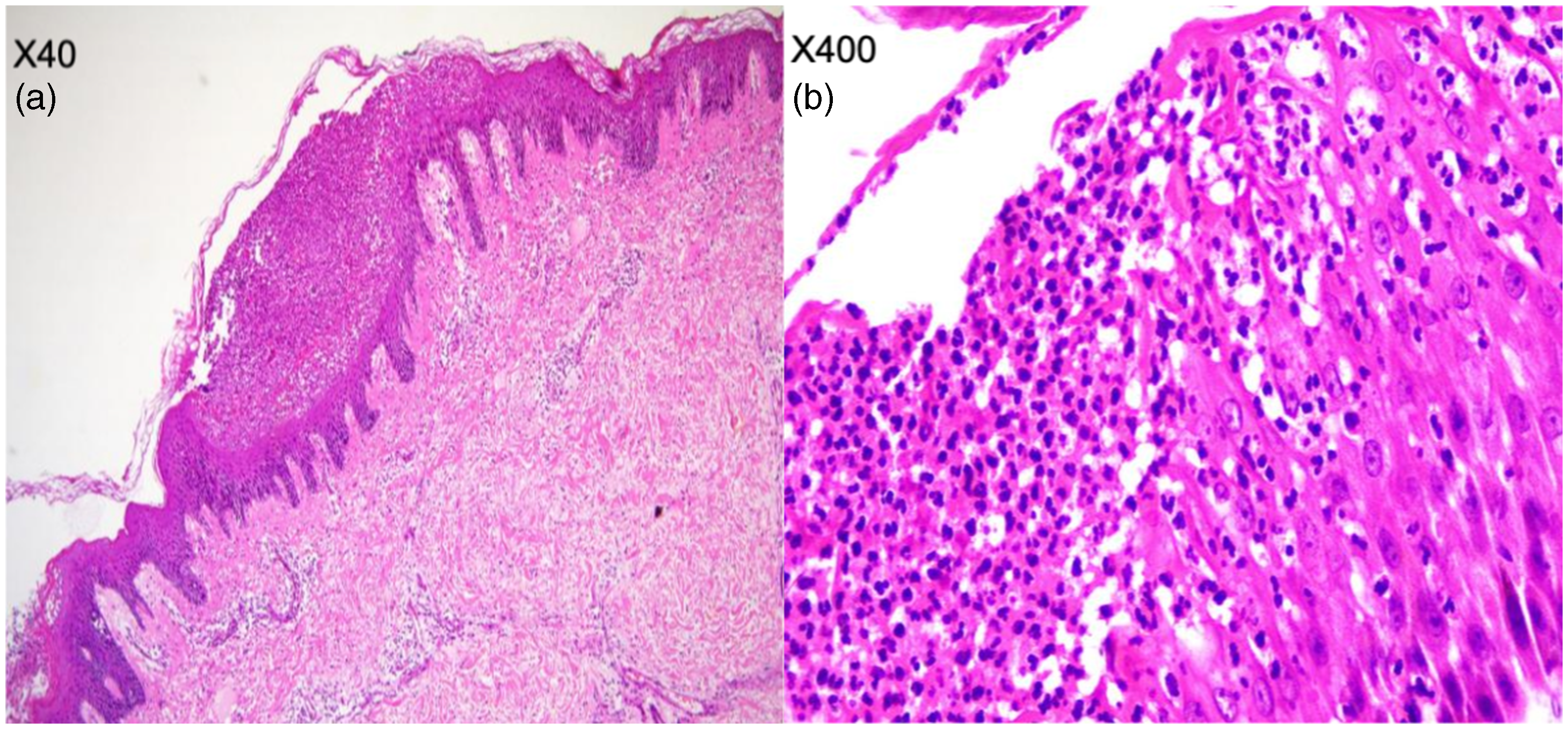
Representative haematoxylin and eosin-stained skin biopsy sections from a patient in her early 30 s who presented after developing rash with itching all over the body at the end of the second trimester of pregnancy, showing: (a and b) pustules mainly composed of neutrophils in the stratum corneum and spinosum. Original magnification, (a) × 40 and (b) × 400.
After admission, the patient was treated with anti-infection (1.5 g cefuroxime sodium by intravenous [i.v.] drip, twice daily) and anti-allergy medication (30 mg acetate prednisone, orally, daily), along with 2 g calcium gluconate and 2 g vitamin C by i.v. infusion, daily, and external application of calamine lotion, twice daily. Over the course of 5 days, the patient’s condition deteriorated, so the antibiotic was upgraded to 500 mg imipenem cilastatin sodium (i.v. drip, every 6 h), with 20 mg methylprednisolone (i.v. drip, every 12 h) and human Ig pulse shock treatment (20 mg human Ig, daily for 3 days) added to the regimen. In addition, the patient was administered 6 mg dexamethasone by intramuscular injection every 12 h, to promote fetal lung maturation. At 29+1 weeks of pregnancy (after 13 days of hospital treatment), an emergency caesarean section and skin biopsy were performed, because fetal movement was reduced, and fetal heart monitoring did not show a response. Consequently, a live male baby was delivered with an Apgar score of 6 at 1 min, 7 at 5 min, and 10 at 10 min, and the patient's body temperature gradually returned to normal (36.5 °C). The pathology report of pustules mainly composed of neutrophils in the stratum corneum and spinosum led to a comprehensive diagnosis of impetigo herpetiformis and 50 mg cyclosporine, orally, twice daily, was added to the treatment regimen. The rash gradually improved and inflammatory markers decreased significantly after surgery. The patient was discharged after 21 days of hospital treatment with instructions for self-administration of cyclosporine. Following discharge, the patient chose to discontinue cyclosporine treatment after 1 week, and the rash completely subsided after 3 months postpartum. In the patient’s view, suffering from this disease was extremely painful and dangerous, and she expressed great gratitude for the treatment she received.
Discussion
In the present case, impetigo herpetiformis was considered based on the following: (1) typical signs, comprising clusters of pinpoint-sized sterile pustules or pus lakes distributed throughout the body; (2) systemic symptoms, comprising fever, pain and fatigue; (3) laboratory tests showing significantly increased inflammatory markers, and pustular test and blood culture showing aseptic result; (4) pathological results showing neutrophil-based pustules in the stratum corneum and stratum spinosum; (5) ineffectiveness of various treatments; and (6) rapid relief of symptoms after termination of pregnancy.
Impetigo herpetiformis usually occurs in the third trimester of pregnancy, but there are sporadic reports of onset in early pregnancy. 7 A review of the PubMed database revealed only five previously reported cases of impetigo herpetiformis in the second trimester of pregnancy, and these are summarised, along with the present case, in Table 1. Two cases resulted in stillbirths,8,9 while the other four delivered live infants,10–12 of which two were healthy. The two cases of stillbirth occurred when the rash began before 21 weeks and there was a long disease course before medical treatment. In two of the patients,10,11 the total disease duration was short, with neither lasting more than 1 month, and with no serious systemic symptoms, although the patient reported by Fiboumi et al. 11 was febrile, which may have been a transient fever with a short duration. The remaining two patients, including the present case, exhibited systemic symptoms, such as fever, and a relatively long disease course. 12 This seems to indicate that fetal prognosis may be related to time of onset, duration of impetigo herpetiformis, presence of fever, and the duration of fever. Therefore, early detection, diagnosis, and treatment are vital to avoid serious complications. However, these findings need to be further investigated to fully understand the prognostic factors.
Cases of impetigo herpetiformis in the second trimester of pregnancy.
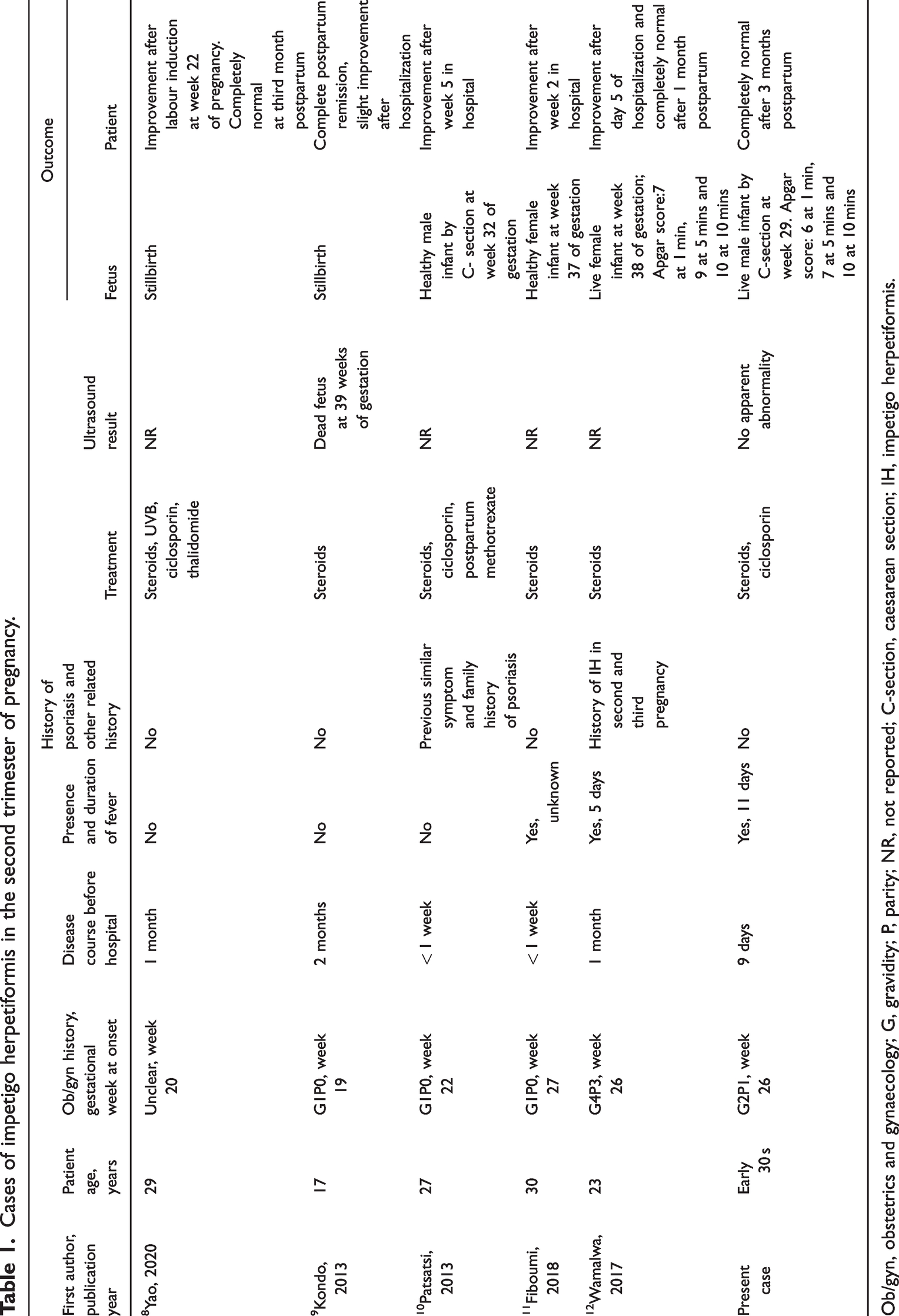
Ob/gyn, obstetrics and gynaecology; G, gravidity; P, parity; NR, not reported; C-section, caesarean section; IH, impetigo herpetiformis.
Acute generalized exanthematous pustulosis (AGEP) induced by hydroxychloroquine has been reported in recent years, and the patient in the present case had a medication history of hydroxychloroquine. The clinical characteristics and histopathology of AGEP are similar to impetigo herpetiformis, so our initial diagnosis was AGEP. However, after a comprehensive analysis of the entire pathogenesis in the present case, we believe that the diagnosis of AGEP is not supported.
The evidence not supporting AGEP includes: (1) medication history: the patient had taken only hydroxychloroquine for 7 weeks before disease onset, but the time to AGEP occurrence after initiating hydroxychloroquine is typically 3–30 days; 13 (2) long disease course: drug-induced AGEP usually subsides 2 weeks after drug withdrawal, but in the present case, it took nearly 1 month from disease onset to improvement; and (3) no obvious treatment effect: AGEP can be significantly improved after active anti-infection, anti-allergy, hormone and immunoglobulin shock treatment, while the present patient did not respond to the above treatments. The disease only began to improve rapidly after termination of the pregnancy. Thus, based on the above evidence, we believe it is unlikely that hydroxychloroquine caused AGEP. Interestingly, the patient in the present case was a pregnant female, and the diagnosis of Sjogren's syndrome was doubtful (no evidence for diagnosis). The autoantibody test showed ANA (+), so differentiation from systemic lupus erythematosus (SLE) was required. SLE occurs in women of childbearing age and may be induced and aggravated by infection, pregnancy, and drugs. Its clinical manifestations are complex, and the disease is often more serious. However, based on the clinical manifestations, laboratory examination, and pathological results, the diagnosis of SLE was excluded.
Drug-induced impetigo herpetiformis has been reported previously, 14 including a case of impetigo herpetiformis possibly caused by hydroxychloroquine. 15 In the present case, the patient had a history of hydroxychloroquine prior to onset, no history of psoriasis or related family history, and no medication or similar episodes in her first pregnancy. Therefore, we believe this patient experienced hydroxychloroquine-induced impetigo herpetiformis. Synthetic antimalarial drugs have been shown to aggravate or induce psoriasis, 16 and previous studies have provided some basis to support the claim that impetigo herpetiformis is a subtype of psoriasis.15,16 The pathogenesis of impetigo herpetiformis is currently unknown, and may be related to genetic factors, 17 endocrine disorders (hypoparathyroidism), and inflammation in the interleukin (IL)-36 pathway. 18 To date, there are no treatment guidelines and current treatment is mainly based on case reports, reviews, and a few studies.17,19–21 Corticosteroids, cyclosporine and infliximab have been recommended as first-line therapy, and phototherapy as second-line. Ustekinumab, an IL-12/23 antagonist, 22 and secukinumab, an IL-17A antagonist, 23 have also been used in recalcitrant cases with good results. In the absence of response to drug therapy, second and third trimester pregnancy termination has been shown to be effective.8,24
Interestingly, the current patient's condition upon admission was confusing and likely to be misdiagnosed as AGEP, which was indeed the diagnosis that was initially considered, but the corresponding treatment did not significantly improve the patient's symptoms and the disease continued to develop. We began to suspect impetigo herpetiformis (which was confirmed upon subsequent review of the patient's entire course and examination data) and promptly improved the relevant tests. At the same time, conventional treatments previously described in the published literature were attempted, including the use of corticosteroids, antibiotics and an immunosuppressive drug, but with little effect. Thanks to close cooperation between dermatologists and obstetricians, the correct diagnosis was made early, the fetal condition was closely monitored, and fetal lung maturation was promoted early. In the end, the pregnancy was terminated in a timely manner when the fetus reached 29 weeks of development (optimising survival after delivery), and a good outcome was achieved for both mother and child.
Conclusions
The present study suggests that hydroxychloroquine might trigger impetigo herpetiformis. Early identification, early diagnosis, early treatment, close fetal monitoring to ensure normal fetal development and smooth birth, and timely termination of pregnancy, are vital for patient and fetal outcomes.
Footnotes
Acknowledgements
We thank the participants of the study.
Author contributions
Yingcai Wan wrote the manuscript. Lei Zhang collected case data. Jianbo Wu edited and corrected the paper and provided article ideas. Boyu Xie edited the article for language. Mengjie Zhao contributed to pathological analysis. Juanjuan Guo was responsible for obstetrical evaluation. Juan Ding provided epidemiologic data and made revisions according to the recommendation. All authors commented on and approved the manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.