
Abstract
Objective:
The aim of this study was to suggest a new sonographic sign, which could be helpful in the determination of chorionicity in twin pregnancies, during the second and third trimesters.
Materials and Methods:
This was a retrospective study evaluating the sonographic images of 50 women with twin pregnancy. Out of 50 twin pregnancy case reviewed, only 27 were included. Those patient cases that were included were scanned by a single radiologist. The presence of a hypoechoic cleft, in the thickness of placental bulk, could be detected in all of the dichorionic pregnancy cases. This sonographic appearance was referred to as the “cleft sign.”
Results:
The “cleft sign” was present in all the dichorionic diamniotic (DC-DA) twin pregnancy cases, but no similar appearance was seen in the monochorionic diamniotic (MC-DA) twins. Considering this sign, the radiologist was able to correctly diagnose the chorionicity of all 24 patients in the second and third trimester.
Conclusion:
The findings of the present study suggest a possible role for this newly identified “cleft sign.” This sonographic appearance is a hypoechoic cleft in the thickness of placenta, of dichorionic pregnancies, as an indicator of DC twin pregnancy. In this retrospective case analysis, the “cleft sign” was diagnostically significant in the second and third trimesters.
The 2019 birth rate of twins, in the United States, was 32.1 per 1000 total births. 1 Twin pregnancies can be monozygotic or dizygotic in nature. Dizygotic twinning results from two separate fertilizations, while monozygotic twinning occurs when a single fertilization morula divides and develops to two embryos. Early division, up to 1 to 3 days after fertilization, results in two complete cell lines and dichorionic (DC) twinning. If the morula splits after 4 days or later, the post-fertilization cells are already committed to form the chorion, resulting in monochorionic (MC) twins. Based on time between fertilization and division, MC twins can be diamniotic (DA) (4–8 days after fertilization) or monoamniotic (MA) (8–13 days after fertilization) and can even result in conjoined twins with late splitting (after 13 days). 2 All twin pregnancies have a higher risk of preterm labor, maternal hypertensive disorders, diabetes, and premature rupture of membranes than those of singleton pregnancies; however, chorionicity determines the prognosis of multiple gestations, more accurately.1,2 MC pregnancies have significantly higher risk of intrauterine morbidity and mortality compared with dichorionic ones.3,4 The type of chorionicity can affect routine monitoring of the twin pregnancies 5 as well as the management of twins with abnormalities, including selective fetocide.6,7 Therefore, every attempt should be made to determine the chorionicity of a twin pregnancy.
First Trimester of Pregnancy
Chorionicity should be determined between 11+0 and 13+6 weeks of gestation using the membrane thickness at the site of insertion of the amniotic membrane into the placenta, identifying the T-sign or lambda sign, and the number of placental masses visualized using sonography.8,9 It is important to examine the dividing membrane carefully; in DC-DA twin pregnancy, the twins are separated by a thick layer of fused chorionic membranes with two thin amniotic layers, one on each side, giving the appearance of a “full lambda,” compared with only two thin amniotic layers separating the two fetuses in monochorionic diamniotic twin pregnancy (the T-sign).9 In a large study by Dias et al, chorionicity was correctly assigned by sonography at 11–14 weeks. In 612 of 613 pregnancies (using the placental number, as well as T, and λ-signs) this represented a 99.8% accuracy rate, and the sensitivity and specificity for determining MC were 100% and 99.8%, respectively. 10 Several studies have confirmed the accuracy of “lambda” and “T” signs in predicting chorionicity in the first trimester, comparing the sonographic diagnosis with the postpartum placental evaluation. The sensitivity reported in those studies ranged from 89.8% to 100%; the specificity ranged from 97.4% to 99.8%.11-13
Second and Third Trimester of Pregnancy
In women referring after 14 weeks of gestation, chorionicity is best determined using the same sonographic signs, in particular by counting the membrane layers, and noting discordant fetal sex. 9 However, the reliability of the number of placental masses is questionable, as DC placentas are commonly adjacent to each other, appearing as a single mass, and 3% of MC twin pregnancies have two placental masses on sonography, the presence of which does not preclude vascular anastomoses. It is likely that using a combination of sonographic features, rather than a single one, would be more accurate. 5
Determination of chorionicity in the second and third trimester is more problematic and the diagnostic accuracy is lower compared with the first trimester.14,15 The diagnosis relies on the evaluation of fetal sex, number of the placental masses, and characteristics of the inter-twin membrane. The identification of discordant fetal sex indicates dichorionic twinning. The positive predictive value of discordant sex (when correctly identified) is 100%.14,15 However, it should be considered that the same-sex twin pregnancies include only around 50% of DC pregnancies, so the diagnosis of the chorionicity status needs further sonographic signs.14,15 Similarly, if there are two separate placentas, the pregnancy is DC, but in the majority of cases in the final weeks of second trimester, as well as the third trimester, the two placentas are adjacent to each other and there are often difficulties in distinguishing between fused DC and MC placentas.14,15 This can create confusion when the chorionicity is not elucidated, according to the previous sonograms.
The aim of this study was to suggest a new sonographic sign, which could be indicative of DC twin pregnancy, in the second and third trimesters. In this study, when the radiologist was searching for the twin peak sign, in order to determine the chorionicity, the twins seemed to have a shared placental bulk. It was then that she realized that there was a linear hypoechoic area which looked like a cleft that apparently divided the shared placenta into two parts. This sign was located along where the membranes were attached to chorionic plate. The presence of this cleft-like hypoechogenic appearance was referred to as “cleft sign” and might be indicative of DC, in the second and third trimesters.
Materials and Methods
The present study was conducted in the radiology department of an educational obstetric hospital. An estimated average of 300 pregnancy sonograms were performed in this hospital, each month. The average number of referred twin pregnancies was 5 to 6, monthly. The recorded video and sonographic images of twin pregnancies, referred to the radiology department, for fetal biometry or as a follow-up sonogram, were retrospectively evaluated, over a 1-year period (January to December 2020). Patients were included only if their previous documents, such as first trimester sonography reports, were available. All of the ultrasound equipment systems and the prenatal centers that provided patients with a sonographic evaluation were verified for quality.
All the sonograms were reviewed by an expert obstetric radiologist with more than 10 years of obstetric sonography experience. The radiologist used a Samsung WS 80 ultrasound equipment system with transducer frequencies ranging from 1 to 7 MHz. There were 50 women with twin pregnancies who had their first trimester sonograms preformed in other centers but were included in this study. The exact type of chorionicity was diagnosed in the first trimester at the other radiology centers and those results were considered a gold standard for the present study. The patients were referred to the hospital in the second and third trimesters and the radiologist was not blinded to their first trimester sonograms.
Sonography Examination Protocol
The radiologist reviewed images from the second trimester anatomic or fetal growth exam and focused on images where the placental surface and amnion/chorion fusion could be visualized. During the sonographic examination, it was important to get an overall view of the fetuses and then focus on the placentas. An attempt was made to find the place where the amnion and chorion were attached to the placenta, while the focus was on the surface of placentas. No extra focal magnification was used and the zoom feature was set at the standard for pregnancy sonography. The gain was also placed in the standard examination mode. The “cleft sign” was reviewed in the available sonograms of twin pregnancies and it was present in all of the DC-DA pregnancies. While in MC-DA pregnancies, the location was smooth with no observable cleft in the membrane-placenta attachment. It is noted that this imaging technique was rather difficult for severely obese patients or those who had low levels of amniotic fluid.
Results
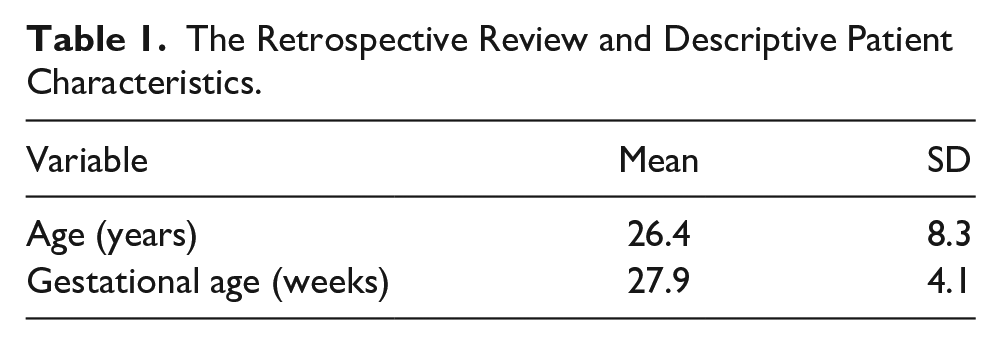
A retrospective review of the stored sonograms from 50 pregnant women with twin pregnancy was carefully evaluated (see Figure 1). There were 15 patient cases that had a separated placenta and were omitted from study. The remaining 35 patient cases, who had single placental bulk, were reviewed. The sonograms of 8 patient cases were deemed to be of poor quality and therefore were excluded from the study. This analysis was based on the remaining 27 patient cases, with a mean age of 26.4 ± 8.3 and a mean gestational of 27.9 ± 4.1 (see Table 1). The “cleft sign,” a hypoechoic linear cleft in continuity of intertwine membranes at the attachment site to chorionic plate, was seen clearly in 24 patients (see Supplemental Video 1). These were characterized as a DC-DA pregnancy, according to first trimester sonogram (see Figures 2–6) and in 3 patients with a MC-DA diagnosis, the sign was absent (see Figures 7–10).
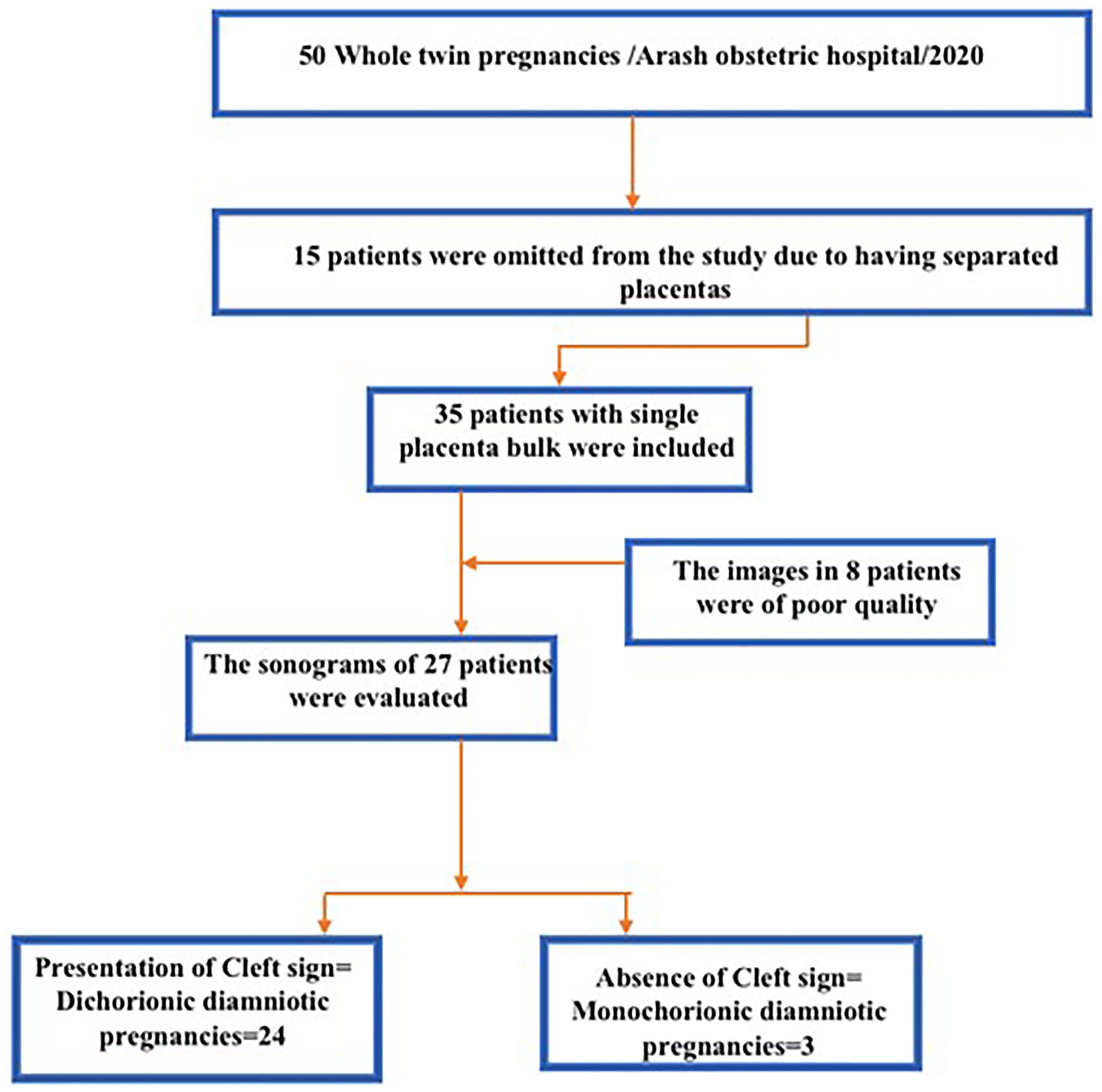
The diagram of patient selection and the sonographic results.
The Retrospective Review and Descriptive Patient Characteristics.

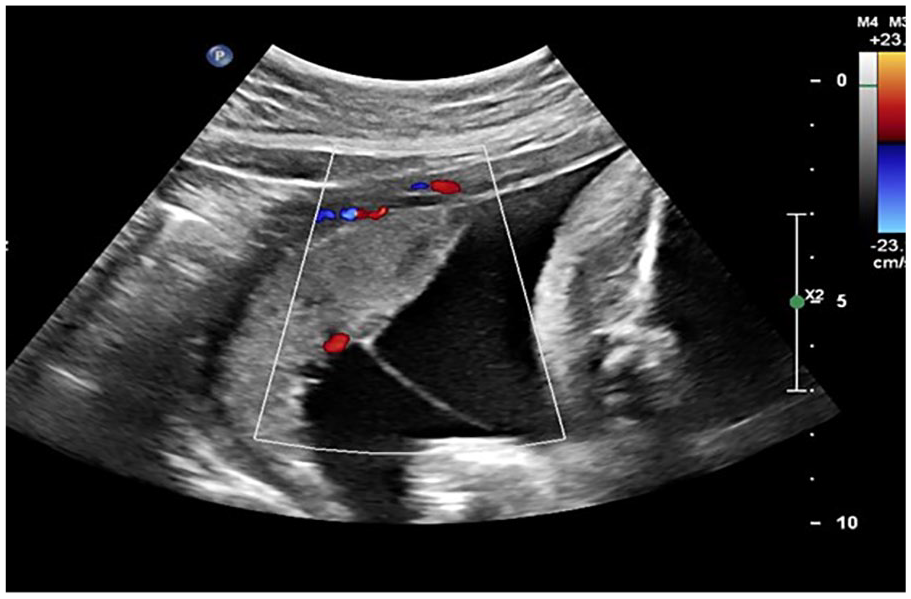
This image demonstrates the “cleft sign” in a 28-week pregnant patient, with a DC-DA twin pregnancy. DC-DA, dichorionic diamniotic.

The arrows demonstrate the “cleft sign” where the amnion attaches to the placenta in a 30-week pregnant patient, with a DC-DA pregnancy . DC-DA, dichorionic diamniotic.

The “cleft sign” is noted in a 27-week pregnant patient, with a DC-DA twin pregnancy. DC-DA, dichorionic diamniotic.

This sonographic image demonstrates the “cleft sign” in a 27-week pregnant patient, with a DC-DA twin pregnancy. DC-DA, dichorionic diamniotic.

The sonographic appearance of the “cleft sign” in a 26-week pregnant patient, with a DC-DA twin pregnancy. DC-DA, dichorionic diamniotic.

This sonogram demonstrates the absence of the “cleft sign” in a 27-week pregnant patient, with MC-DA twin pregnancy. MC-DA, monochorionic diamniotic.

The absence of the “cleft sign” is noted on this sonogram of a 28-week pregnant patient, with MC-DA twin pregnancy. MC-DA, monochorionic diamniotic.
There is a noted absence of the “cleft sign” in this 29-week pregnant patient, with a MC-DA twin pregnancy. MC-DA, monochorionic diamniotic.

A noted absence of the “cleft sign” in this 30-week pregnant patient, with a MC-DA twin pregnancy. MC-DA, monochorionic diamniotic.
Discussion
Determining the exact chorionicity status is the cornerstone for accurate managing of twin gestation. The knowledge of chorionicity helps the clinicians to evaluate the risk of pregnancy complications such as twin-to-twin transfusion syndrome and selective intrauterine growth restriction, as well as managing fetal demise and discordant fetal anomaly. This information even affects the follow-up interval and delivery time. The most accurate diagnosis of chorionicity is achieved in the first trimester, when the diagnostic accuracy approaches 100%. 16 The most reliable sonographic signs are the lambda sign, T-sign, and the number of placental masses evaluated before 14 weeks of gestation. 16 The more advanced a pregnancy becomes, the more difficult it is to correctly determine the chorionicity. The dividing membrane in a DC pregnancy appears thinner as the pregnancy progresses, and the lambda or twin peak sign becomes less prominent.17,18 When the fetuses are the same sex, and there is a single placental mass, it can be very difficult to decide whether a pregnancy is DC or MC. 19
Stenhouse et al in their study evaluated 138 twin pregnancies, regarding the chorionicity status and comparing the results with placental pathology results. 13 They reported that the chorionicity was correctly identified in 131 out of 138 cases. 13 They also mentioned that out of 7 incorrect diagnoses of chorionicity, 5 were due to the late sonographic evaluation (after 14 weeks), leading to a 100% sensitivity for evaluation <14 weeks and a 91% overall sensitivity. 13 In addition, they indicated that in 4 of these incorrectly diagnosed cases, pathologic findings confirmed the incorrect sonographic results. 13 Consistently, Blumenfeld et al demonstrated a higher risk of chorionicity misclassification in patients referring after 14 weeks of their gestation (OR: 0.47). 20 It was also reported that the odds of incorrect chorionicity detection rose by 10% for each week of increase in gestational age. 20
All of the above-mentioned information emphasizes the importance of establishing some other reliable signs for determining the chorionicity, in the second trimester. Despite the widespread diffusion of sonography, as a basic screening test, there is still limited knowledge about the correct diagnosis of chorionicity in the second and third trimester. According to the results of the present study, a thin longitudinal hypoechoic cleft in placental thickness just at the location of membrane attachment to the placental bulk was dubbed the “cleft sign.” It was observable as a consistent finding in DC-DA pregnancies in the thickness of placental bulk. Based on limited information, this sonographic sign has not been introduced before previously. Although the “cleft sign” can be useful in the first trimester sonograms when the placentas are located close to each other, it cannot provide more information than appearances, such as Lambda sign, during this period. The actual benefit of applying the “cleft sign” could be applied during in the second and third trimesters, when other sonographic signs are not as accurate. The results of the present study suggested that it may be possible to determine the chorionicity by sonography in the second and third trimester and trying to detect the presence or absence of a “cleft sign.” The diagnosis for all of the pregnancies in which the “cleft sign” was absent were MD, according to the first trimester sonograms and vice versa.
Limitations
The main limitation of this study was the research design and using a convenient sample for retrospective review. In addition, it was a limitation to consider the first trimester sonographic results as the gold standard, instead of postpartum examination of placenta. In addition, this study was limited by the small number of patients, especially the fact that only three of cases were MC pregnancies. The other limitation was the awareness of the radiologist about the type of chorionicity during evaluation of the recorded images. All of these limitations make these results not generalizable to the larger population. However, the use of the “cleft sign” may have merit, and before it can become widespread diagnostic tool, it would be necessary to be confirmed by larger studies and include all types of twin pregnancies. The introduction of this new sonographic finding needs larger prospective studies in which the patients will be followed up until the delivery for accurate evaluation of sensitivity, specificity, and accuracy.
Conclusion
The potential complications of MC twinning make the accurate determination of chorionicity very important. The findings of the present study suggest a noted use of a new sonographic imaging sign, referred to as the “cleft sign.” This sign, which is a hypoechoic cleft, in the thickness of the placental bulk, in DC pregnancies, may be an indicator of DC twin pregnancy, in the second and third trimesters. This potential sonographic sign might help clinicians to characterize the chorionicity of patients in later periods of pregnancy and for those who do not have reliable documents of their first trimester of pregnancy. So it might be very useful for clinical management, follow–up, and evaluation of related complications and even making decision for delivery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.