
Abstract
Rehabilitative ultrasonography (RUS) has significantly enhanced musculoskeletal care by providing real-time, detailed visualizations of muscle, tendon, and soft tissue structures. This symposium explores the diverse applications of RUS, highlighting its advantages over traditional imaging methods. In muscle rehabilitation, RUS is pivotal for assessing muscle morphology, activation patterns, and providing biofeedback, thereby optimizing personalized rehabilitation programs. For tendon injuries, RUS facilitates precise evaluation of tendon integrity, enabling accurate diagnosis, monitoring, and guiding therapeutic interventions. Beyond muscles and tendons, RUS is invaluable in diagnosing and managing soft tissue pathologies, such as ligament and fascia injuries, allowing for targeted treatment strategies. By offering superior precision, safety, and cost-effectiveness, RUS sets a new benchmark in rehabilitation practices, leading to improved patient outcomes and a deeper understanding of musculoskeletal conditions. The integration of RUS into rehabilitation medicine represents a transformative advancement in patient care and treatment efficacy.
Rehabilitation plays a pivotal role in health care, enabling individuals to recover and regain functional autonomy. Currently, an estimated 2.41 billion people worldwide require rehabilitation services due to a range of conditions, notably musculoskeletal disorders, underscoring the urgent need for expanded services. 1 The field of rehabilitation has been profoundly transformed in recent years through the integration of ultrasonography, or rehabilitative ultrasonography (RUS), specifically. This technology equips clinicians with a dynamic and invaluable diagnostic tool, significantly enhancing patient assessments, treatments, and outcomes.2 –4 RUS offers superior precision, safety, and cost-effectiveness compared with traditional imaging methods, making it an ideal match for modern rehabilitation practices. 5 This review delves into the diverse applications of ultrasonography in rehabilitating various tissues and underscores its benefits over conventional techniques (See Table 1).
The Applications, Benefits, and Imaging Modes of Rehabilitation Ultrasonography Used in the Care of Patients in Rehabilitation.
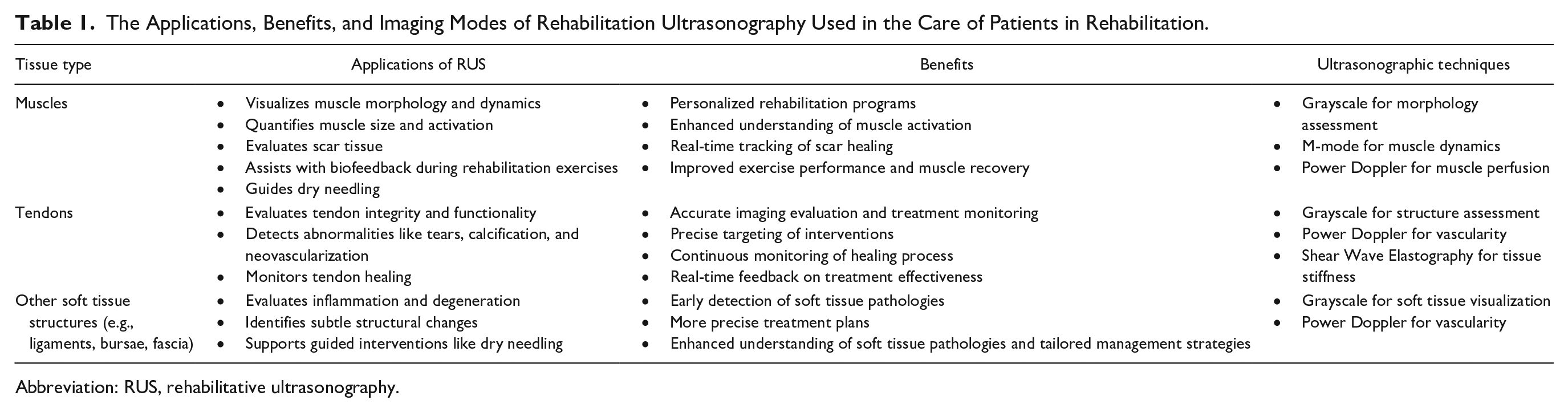
Abbreviation: RUS, rehabilitative ultrasonography.
Muscle Rehabilitative Ultrasonography
The RUS has significantly advanced musculoskeletal treatment strategies by providing real-time, detailed visualizations of muscle morphology and dynamics. Validated over decades as a method for quantifying muscle size, 6 RUS assists in assessing trunk muscle size and activation during isometric sub-maximal contractions. 7 This capability is vital for accurately evaluating muscle activation patterns, recruitment strategies, and detecting fatty infiltration in muscles, which is crucial for designing personalized rehabilitation programs tailored to the unique needs of each patient (See Figure 1). 8 The RUS is also increasingly employed in managing conditions such as low back and pelvic pain, offering both quantitative and qualitative insights into abdominal muscle function. 8 This enriches clinical assessments and supports research endeavors focused on these common yet complex conditions. In addition, RUS provides biofeedback during rehabilitation exercises, enhancing patients’ understanding of muscle activation and movement patterns, thus improving exercise performance and optimizing rehabilitation outcomes.8,9 Another important application of RUS is in assessing scar tissue, as it can help differentiate between scar tissue and healthy tissue in many cases, aiding in the monitoring of the healing process after injury or surgery. 10 While RUS provides valuable insights into the progression of scar tissue, the accuracy of these assessments can depend on factors such as tissue depth and operator expertise. 11 This functionality enables clinicians to adjust treatment plans based on visualized changes, supporting more informed therapeutic interventions. Finally, researchers have found that sonography-guided dry needling significantly enhanced therapeutic outcomes for muscular pain by precisely targeting affected areas, alleviating pain, and promoting muscle recovery in athletes, and in managing myofascial pain, improving muscle function, reducing pain, and enhancing mobility in patients with low back pain.10,12
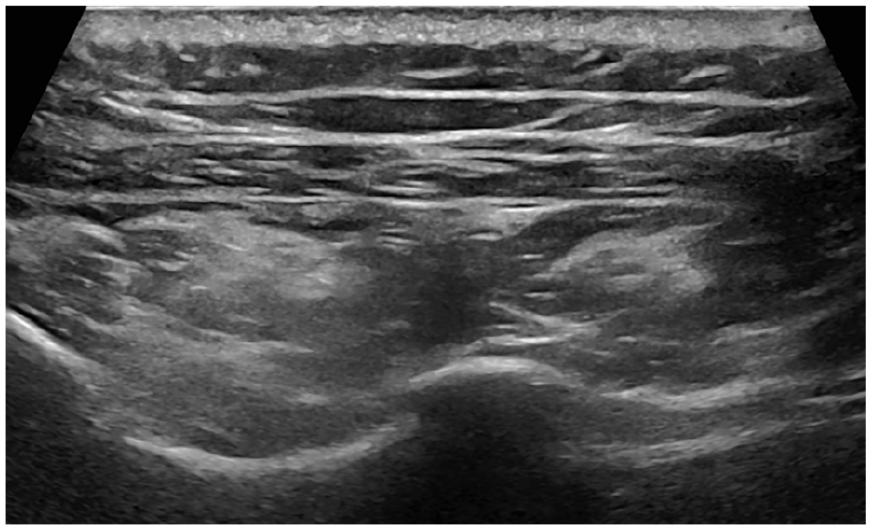
An example sonogram in the short-axis plane of the infraspinatus and teres minor muscles, showing fatty infiltration in the infraspinatus muscle.
Tendon Rehabilitative Sonography
In the management of tendon injuries, ultrasonography is indispensable, providing detailed imagery that enables a comprehensive assessment of tendon integrity and functionality. 13 Ultrasonography allows clinicians to evaluate the structural integrity of tendons—crucial for detecting abnormalities such as tendon calcification, tears, neovascularization, and degenerative changes (See Figure 2).14,15 These evaluations are essential for accurately diagnosing injuries16,17and effectively monitoring the healing process. 18 A study by Ernat et al. 19 underscores the utility of grayscale sonography in conjunction with clinical exams for assessing tendon gaps in acute Achilles tendon tears. The authors pointed out some discrepancies with magnetic resonance imaging (MRI) regarding residual gapping, providing crucial insights for making informed decisions. These insights are crucial for making informed decisions between surgical and non-surgical treatments based on tendon approximation. 20 Furthermore, integrating power Doppler with grayscale sonography enables clinicians to accurately pinpoint the location and severity of tendinopathy, such as insertional vs non-insertional Achilles tendinopathy. 19 This precise localization is vital for crafting targeted exercise rehabilitation plans and closely monitoring responses to interventions. 19 The RUS, along with shear wave elastography, another form of ultrasonography, supports the continuous observation of changes in tendon structure and integrity throughout the healing process,18,21 –23 allowing clinicians to make timely adjustments to treatment strategies or predict future tendon symptoms. It also plays a key role in guiding therapeutic interventions by providing real-time feedback on tendon function and the effectiveness of treatments being administered. This immediate insight significantly can enhance the overall effectiveness of treatment management, ensuring optimal recovery, rehabilitation outcomes, and injury prevention. 24
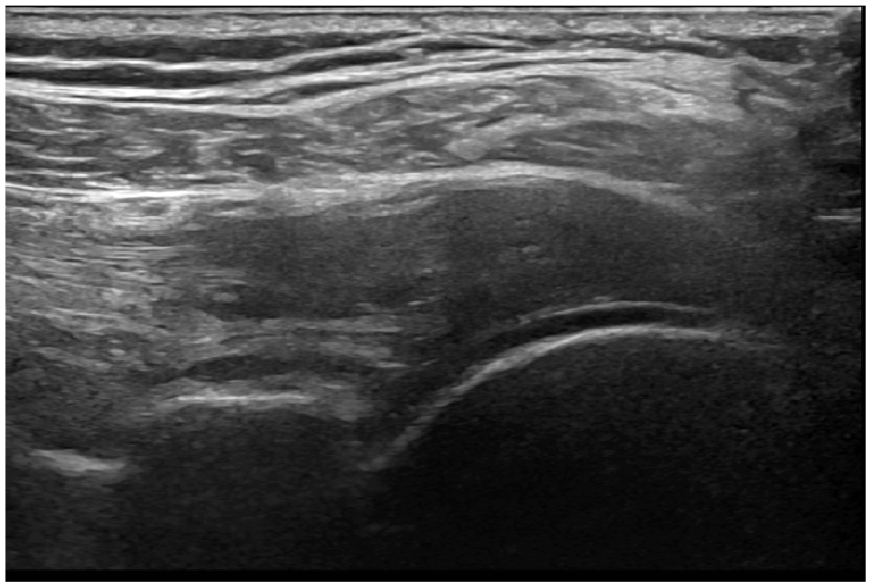
An example sonogram in the long-axis plane of the infraspinatus tendon showing tendinosis with loss of normal fibrillar pattern, reduced echogenicity, and tendon thickening.
Imaging Beyond Muscles and Tendons: Soft Tissue Applications
Beyond its pivotal role in muscle and tendon diagnostics, RUS is equally crucial in examining the severity of damage or ruling out pathologies in other soft tissues such as ligaments, bursae, and fascia, significantly expanding its applicability across a spectrum of conditions (See Figure 3). The RUS supports the process of diagnosing soft tissue inflammation and degeneration by identifying subtle changes indicative of these conditions’ early stages.25,26 This capability may enable the implementation of targeted therapeutic interventions, such as a specific exercise program or the use of modalities, precisely tailored to the patient’s needs based on real-time data. Moreover, the ability to visualize these soft tissues during rehabilitation sessions allows clinicians to adopt a more precise and customized approach to treatments, such as sonography-guided dry needling.10,12 In addition, RUS’s advanced imaging capabilities provide invaluable insights into clinical research, enhancing our understanding of various soft tissue pathologies and their optimal management strategies.
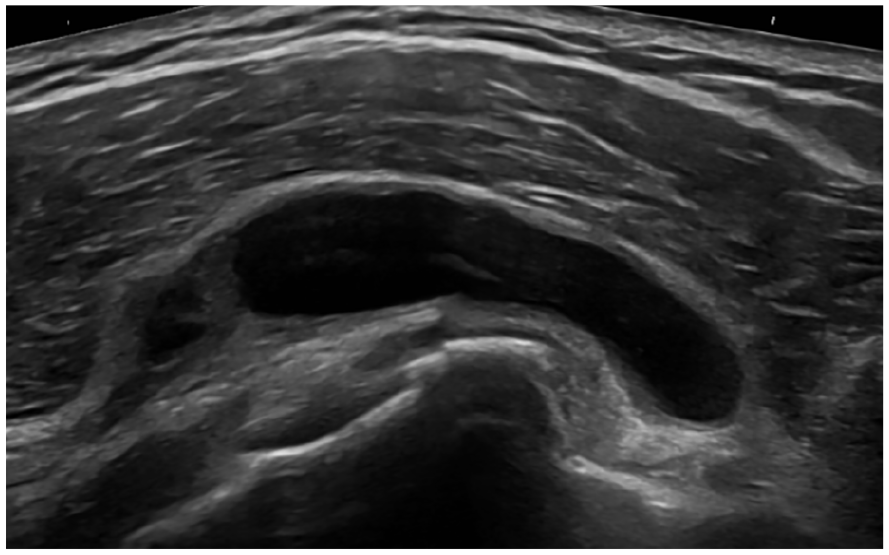
An example sonogram showing subacromial-subdeltoid bursal effusion with anechoic fluid located anterior to the subscapularis and long head of biceps tendons.
Limitations and Future Research
The RUS is a valuable diagnostic tool for assessing soft tissue structures; however, it has notable limitations. The accuracy of RUS is highly dependent on the operator’s proficiency, and while it provides excellent visualization of superficial structures, it is less effective for imaging deeper tissues. The absence of consistent standardized imaging protocols, across the different body regions and structures, contributes to variability in outcomes. Moreover, the cost of the equipment, although lower than other imaging modalities (i.e., MRI, computed tomography, etc.), and the specialized training required for effective use pose barriers, particularly for smaller clinics or those in resource-constrained settings.
Future research should focus on the development of standardized imaging protocols to ensure consistency and reliability in outcomes. In addition, further investigation into the use of ultrasonography by allied health professionals and medical specialists in musculoskeletal disorders is of importance. Evaluating its application based on their specific scope of practice can help expand accessibility and optimize usage in clinical settings. Advancements in automation could also assist operators by enhancing precision and consistency. Finally, making RUS more affordable and accessible will be essential for broadening its application, particularly in low-resource environments.
Conclusion
The integration of RUS into musculoskeletal and rehabilitation medicine represents a significant advancement, enhancing our understanding of the human musculoskeletal system in motion. This deeper insight leads to more precise and effective interventions, markedly improving patient outcomes. As the field continues to embrace advanced diagnostic tools, RUS emerges as a diagnostic technique that not only meets but also surpasses the standards of contemporary health care practice. By fully leveraging the potential of RUS, we anticipate considerable improvements in the quality of life for patients undergoing rehabilitation, setting a new benchmark in treatment efficacy and patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.