
Abstract
Baker cysts are the most common pathologic finding in the sonography of the popliteal fossa. They have a wide range of sonographic appearances. Some of them may need to be recognized and differentiated from other popliteal lesions. Therefore, familiarity with their different imaging appearances is useful for clinical practice. This review summarized different presentations of Baker cysts. They are described in several categories, organized according to their shape and formation: typical Baker cysts and their mild variations, atypical small Baker cysts, ʎ-shaped Baker cysts and their related variations, Baker cysts with extension into nearby muscles, and Baker cysts with complications. The related differentiations are included in each category. The pathogenesis of Baker cysts is also discussed.
A Baker cyst is an abnormal fluid distension in the gastrocnemiosemimembranosus (G-S) bursa of the knee. 1 Adams first generically described these popliteal cysts in 1840. Baker more clearly delineated these in 1877 as synovial cysts that had a connection with knee joint disease. Baker cysts are common disorders of the knee. They are found in about 4% to 7% of asymptomatic adults (mean ages, 45-57 years),2,3 38% of patients (mean age, 39 years) with suspected nonacute knee internal derangements, 4 and 22% to 47% of patients (mean age, 60 years) with osteoarthritis of the knee.5,6 The prevalence of Baker cysts is 2.4% in asymptomatic children 7 and 6.4% in the pediatric population with knee pain. 8 Baker cysts are also the most common pathologic finding in the sonography of the popliteal fossa.9,10 Sonography has been recognized as being as valuable as magnetic resonance imaging in the diagnosis of Baker cysts.11,12 Baker cysts have a wide spectrum of sonographic presentations. Some can be easily identified, whereas some need to be differentiated from other popliteal lesions. Familiarity with their different imaging appearances is useful for proper recognition and diagnosis of Baker cysts. The purpose of this review is to provide comprehensive sonographic information of Baker cysts by presenting a spectrum of the images of Baker cysts.
Pathogenesis of Baker Cysts
G-S bursa is located in the medial aspect of the popliteal fossa of the knee, at the intersection between the semimembranosus tendon (SMT) and the tendon of the medial head of the gastrocnemius (MHG). 1 The bursa consists of proximal and distal portions. 13 The proximal portion consists of deep and superficial parts. The superficial part is located superficial to the MHG, whereas the deep part lies deep to the SMT and the tendinous deep surface of the MHG. The two parts are connected between the outer border of the SMT and the inner border of the tendon of the MHG (Figure 1). On transverse view at the intersection point, the bursa displays as a ʎ shape (Figure 2). The distal portion of the bursa extends downward, forward, and inward deep to the SMT to reach the inner tuberosity of the tibia. In the meantime, its lower third also lines the SMT superficially. The G-S bursa is frequently seen having a septum inside, which sometimes separates the bursa into two independent portions. 13
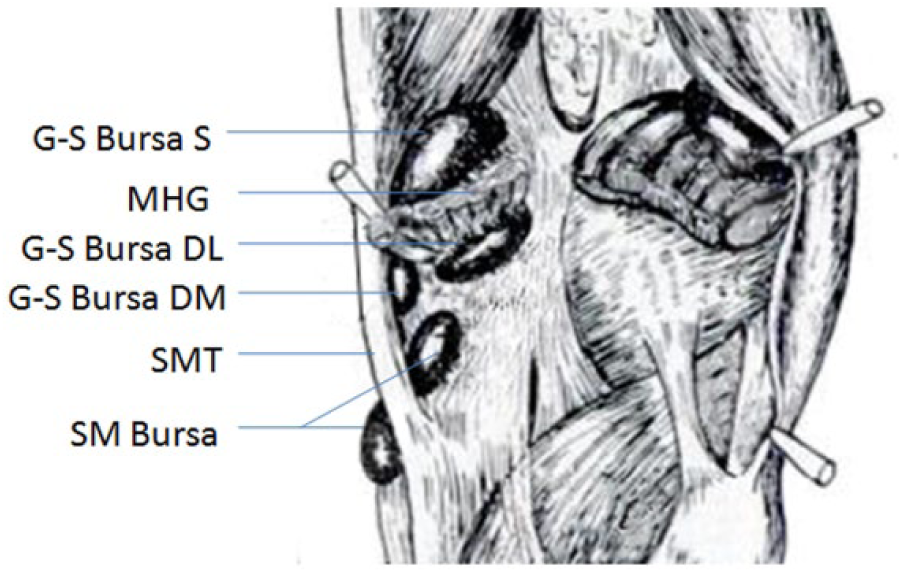
The posterior view of the popliteal fossa: the superficial part of the G-S bursa (S); the deep lateral (DL) part, which is deep to the medial head of the gastrocnemius (MHG); and the deep medial (DM) part, which is deep to the semimembranosus tendon (SMT). The semimembranosus (SM) bursa is at the insertion of the SMT (modified from Wilson et al. 13 ). G-S, gastrocnemiosemimembranosus.
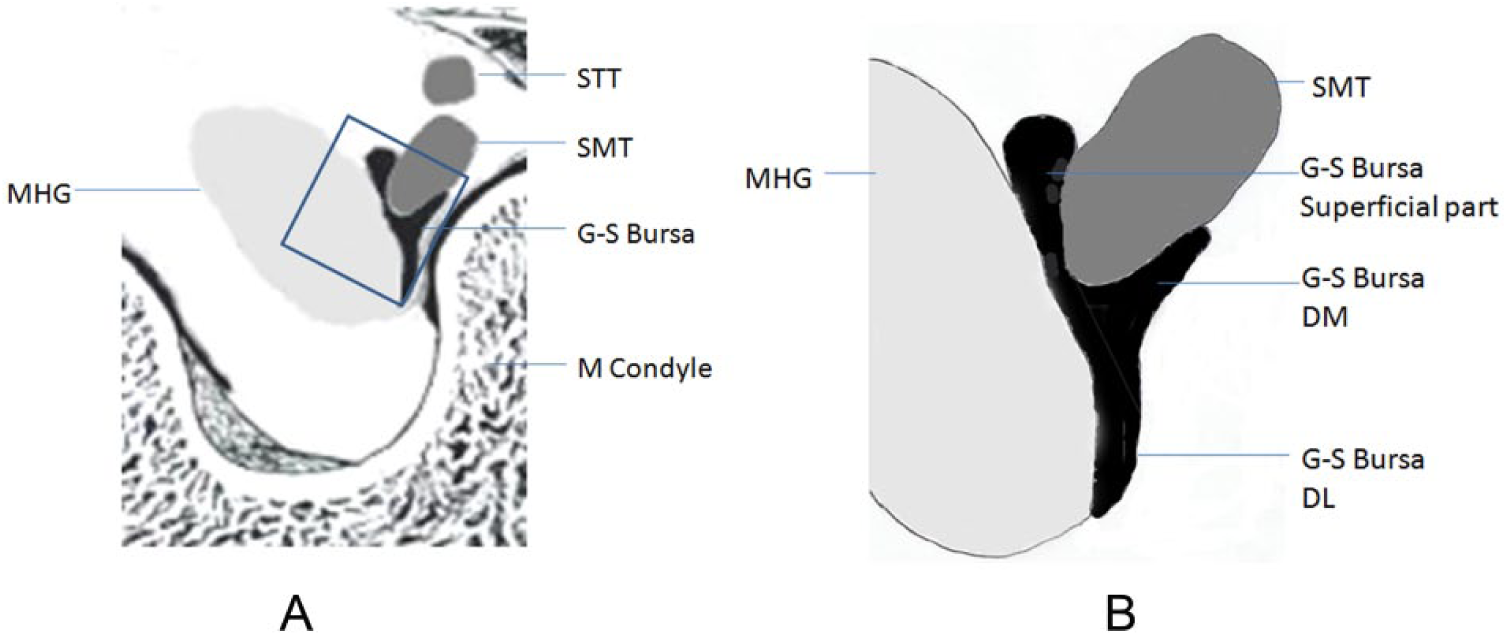
The transverse view of the popliteal fossa: (A) the G-S bursa and its relationship with the semitendinosus tendon (STT), semimembranosus tendon (SMT), medial head of the gastrocnemius (MHG), and medial (M) condyle (modified from Wilson et al. 13 ); (B) the amplification of the square from panel A. The detailed superficial deep lateral (DL) and the deep medial (DM) parts of the G-S bursa. G-S, gastrocnemiosemimembranosus.
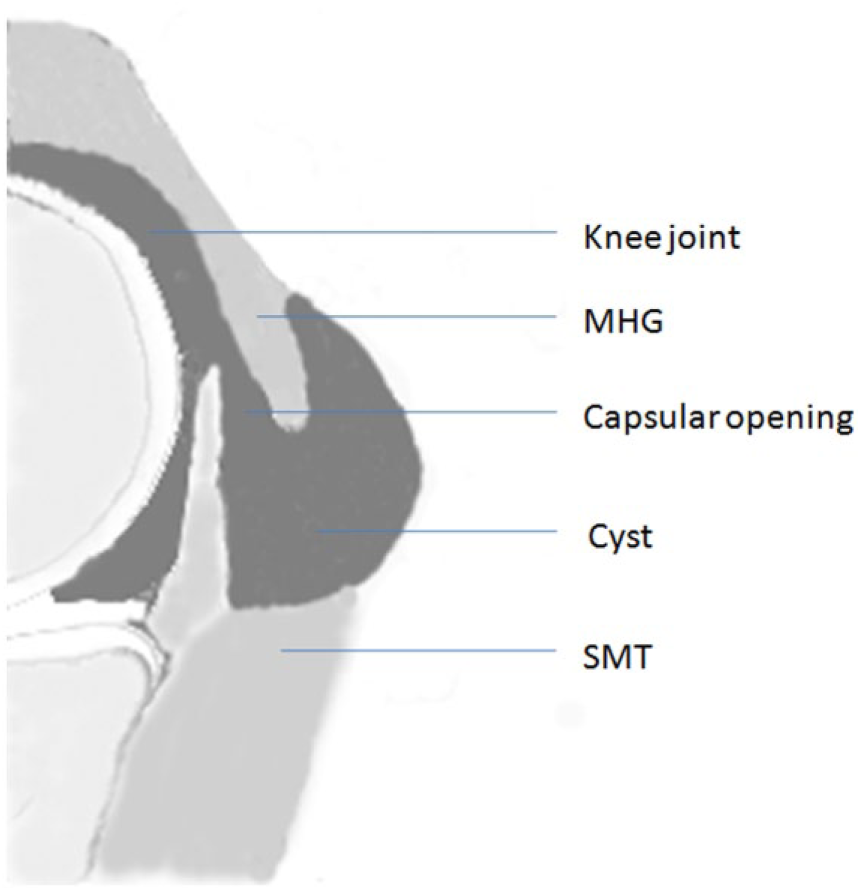
About 57% to 58% of adult G-S bursae were found to communicate with the knee joint through a capsular opening,13,14 but only the proximal part of the bursa deep to the MHG may communicate with the joint. The capsular opening invariably has the shape of a transverse slit opposite the upper lateral circumference of the medial femoral condyle and is near the origin of the MHG (Figure 3).13,14 However, this capsular opening has rarely been found in children. 15 The occurrence of this opening increases in frequency with age. 8 Even without opening, capsular thinning was observed in the same area, and in such a situation, a Baker cyst is simply a herniation of synovium from the knee joint. 14 The capsular thinning or opening may be a degenerative change during aging due to the capsular pulling forces from the meniscus and the SMT. The opening may be the result of the capsular tear.14,15
Baker cyst in sagittal view of the knee. MHG, medial head of the gastrocnemius; SMT, semimembranosus tendon.
Baker cysts have a close relationship with intra-articular disorders of the knee, such as trauma, arthritis, and infection. 8 The most common trauma is meniscal lesions, especially the tear of the posterior horn of the medial meniscus. The next is anterior cruciate ligament tear and chondral lesions. 16 Almost half patients with Baker cysts have osteoarthritis, followed by rheumatoid arthritis, gout, seronegative spondyloarthropathy, and pyrophosphate arthropathy. 17 For infection, it includes tuberculosis, coccidiomycosis, and so on. All these factors have a common pathologic result of a possible knee effusion, which can cause Baker cysts. 3
With knee effusion, during knee bending with weight bearing, the pressure raises high in the joint, which squeezes fluid in the knee joint into the low-pressured bursa through the capsular opening. During extension of the knee, the capsular opening is closed because of the deep part of the bursa being firmly compressed by the cross action of the overlying tendons of the MHG, semimembranosus, and semitendinosus. Therefore, it entraps the fluid in the proximal deep part of the bursa and causes higher intrabursal pressure. This one-way fluid transmission is called a functional valve mechanism. 14 The high pressure in the deep part of the bursa may push the fluid to other parts of the bursa so that the pressure in the deep part of the bursa declines. When the knee flexes again, the cycle repeats.8,14 Thus, Baker cysts expand and become enlarged. It is presumed that if the surrounding tissue of the bursa is weak and cannot sustain the intrabursal pressure, the bursa may extend into the weak area and expand. Since the superficial part of the bursa is in the subcutaneous tissue and usually sustains lowest pressure as compared with other parts of the bursa, the expansion mostly happens in the superficial part. 18
Typical Baker Cysts and Their Mild Variations
A typical Baker cyst usually presents as a crescent-shaped fluid distension on transverse view. It consists of three distinct aspects: the body, the neck, and the base (Figure 4A).1,19 The base is the part lying deep to the tendon of the MHG but superficial to the posterior capsule of the joint. The body is the superficial part of the bursa, located mainly superficial to the MHG. The neck is the connection between the base and the body. In most adult Baker cysts, the fluid may originate from the knee joint through the capsular opening to the part of the bursa deep to the MHG.3,14 The body of a Baker cyst is usually larger than the base, and the reason is as mentioned before. On longitudinal view, only the body and the base can be visualized superficial and deep to the MHG, respectively (Figure 4B).
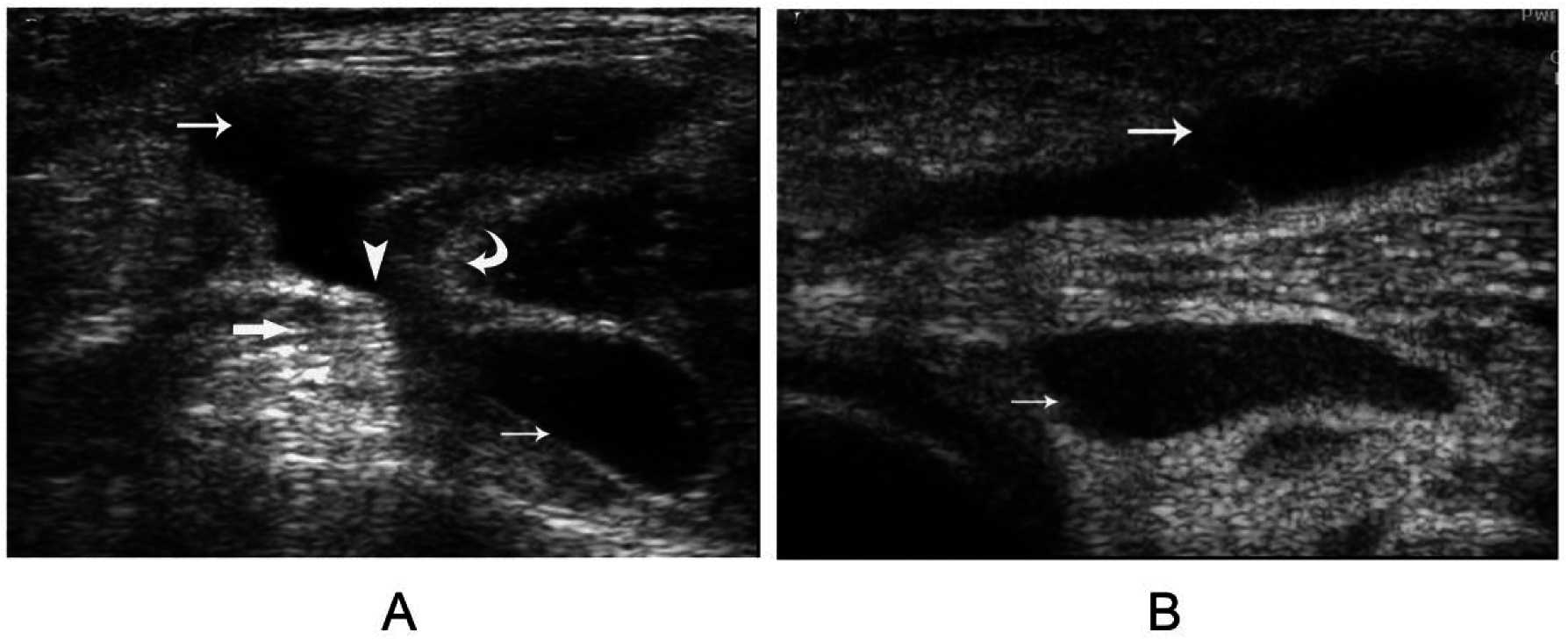
A typical Baker cyst: (A) the base (short arrow), the body (long arrow), and the neck (arrowhead) between the medial head of the gastrocnemius (curved arrow) and the semimembranosus tendon (thick arrow) in transverse image; (B) the base and the body of the cyst in longitudinal image.
These typical Baker cysts may be developed from the effusion of the bursa with a septum, separating the deep medial part from the rest of the G-S bursa, while the deep medial part of the bursa is not involved in effusion.20,21 The fluid in the bursa may originate from the joint instead of from the effusion due to bursitis because most patients with this type of Baker cyst usually present with joint effusion but without symptoms of bursitis. 21 Two reasons may explain that typical Baker cysts are commonly seen. First, G-S bursae containing a septum are frequently seen 13 ; second, more than half of adult bursae have a communication between the deep lateral part in the proximal portion of the bursa and the knee joint through the capsular opening.13,14
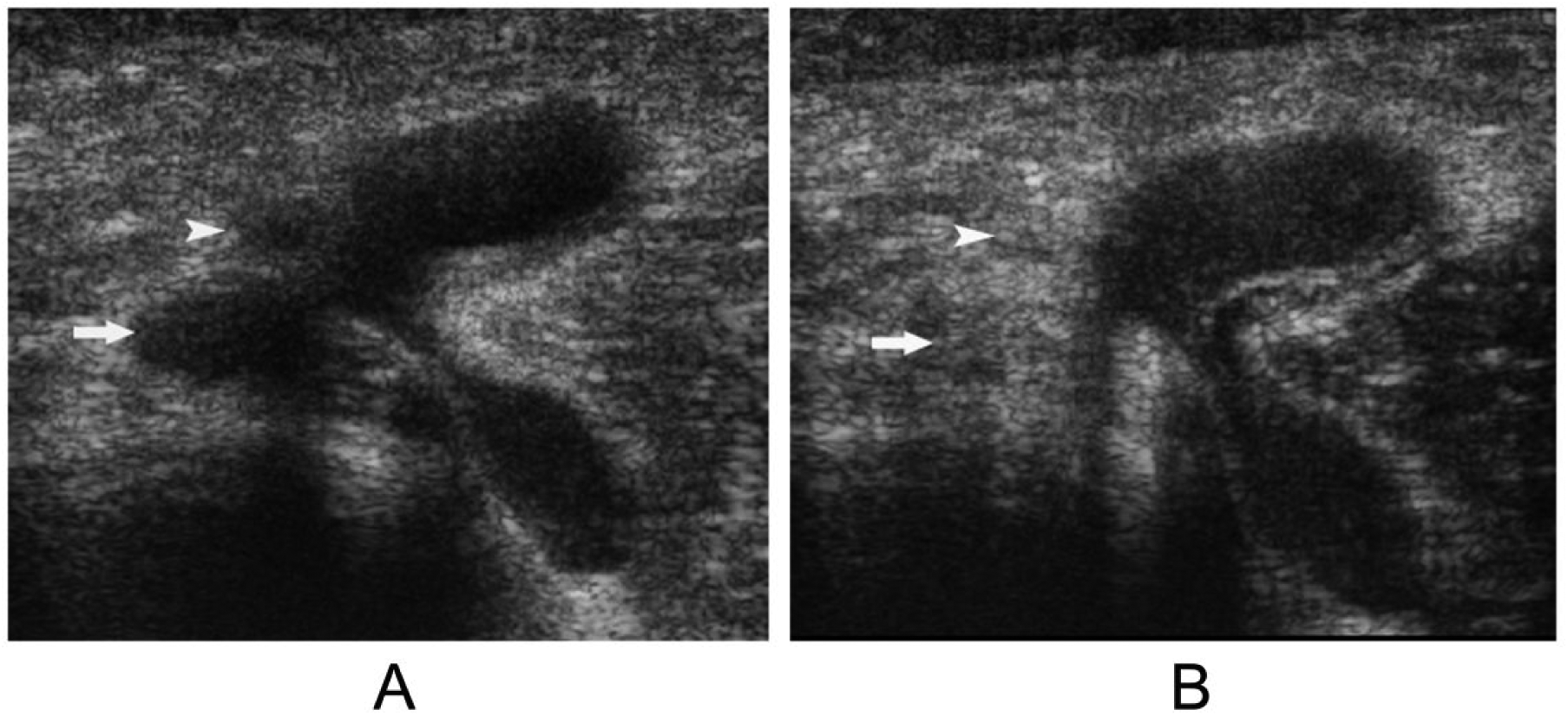
Mild variations of the typical Baker cysts are frequently seen. As previously mentioned, the base is usually much smaller than the body. One mild variation is that the base is much larger than the body (Figure 5A). Sometimes the cyst appears as beak shaped without obvious base. The tip of the beak is the neck of the cyst. This appearance may be that the base is too small to be observed (Figure 5B). Baker cysts with extra septa inside are common. The septa can be complete spanning from one side to the other side of the wall or partially protruding into the cysts (Figure 5C). As we described, the body of the Baker cyst is located mainly superficial to the MHG. One variation is that it is located mainly superficial to the SMT (Figure 5D). This presentation needs to differentiate from semimembranosus bursitis, as will be discussed.
Mild variations of the typical Baker cysts in transverse image. (A) The base (short arrow) is much larger than the body (long arrow). (B) Beak shaped without obvious base. The tip is the neck between the medial head of the gastrocnemius (curved arrow) and the semimembranosus tendon (thick arrow). (C) Extra septa (arrow) inside. (D) The body (thin arrow) is mainly medial to the medial head of the gastrocnemius and superficial to the semimembranosus tendon in transverse image.
Atypical Small Baker Cysts
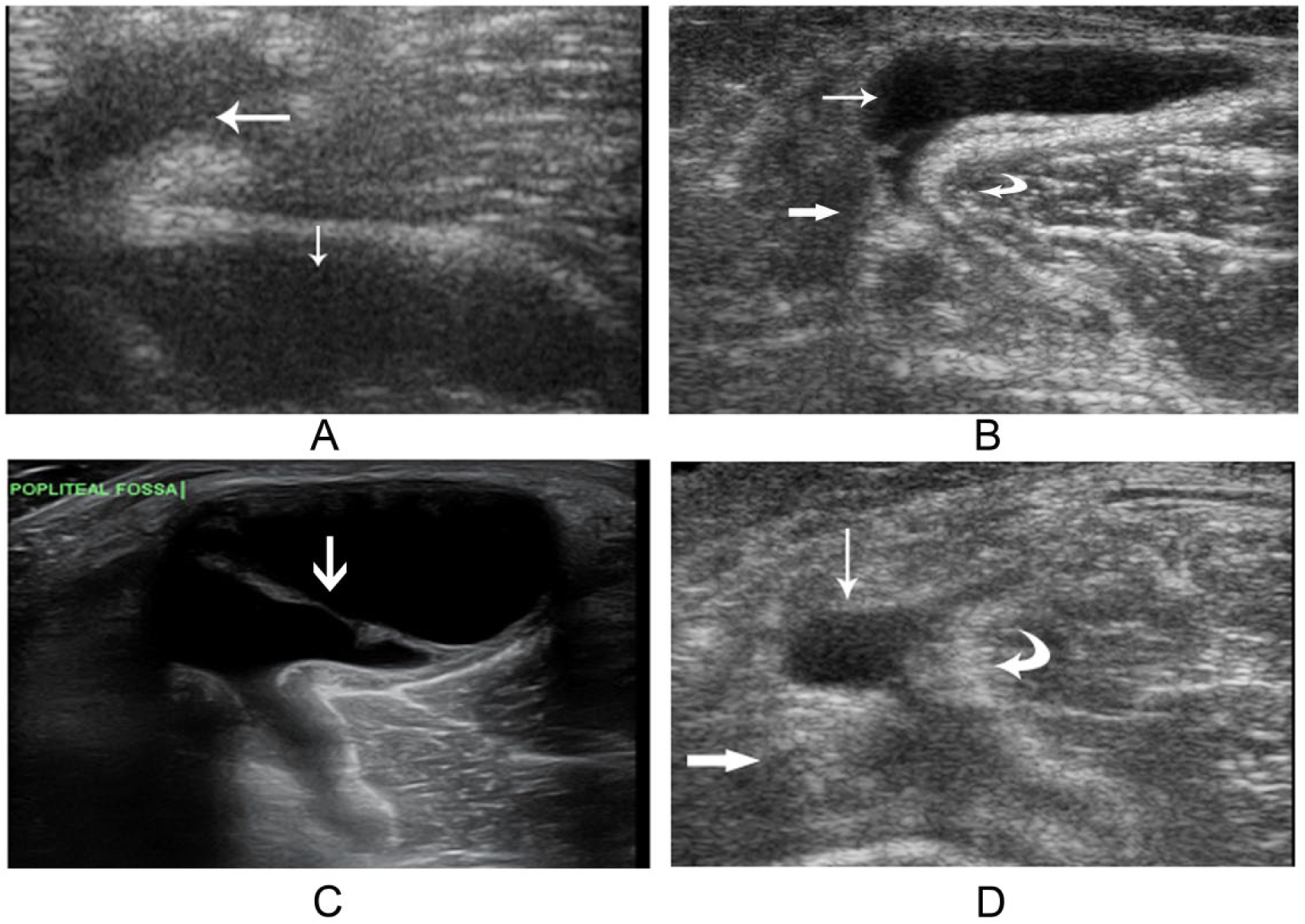
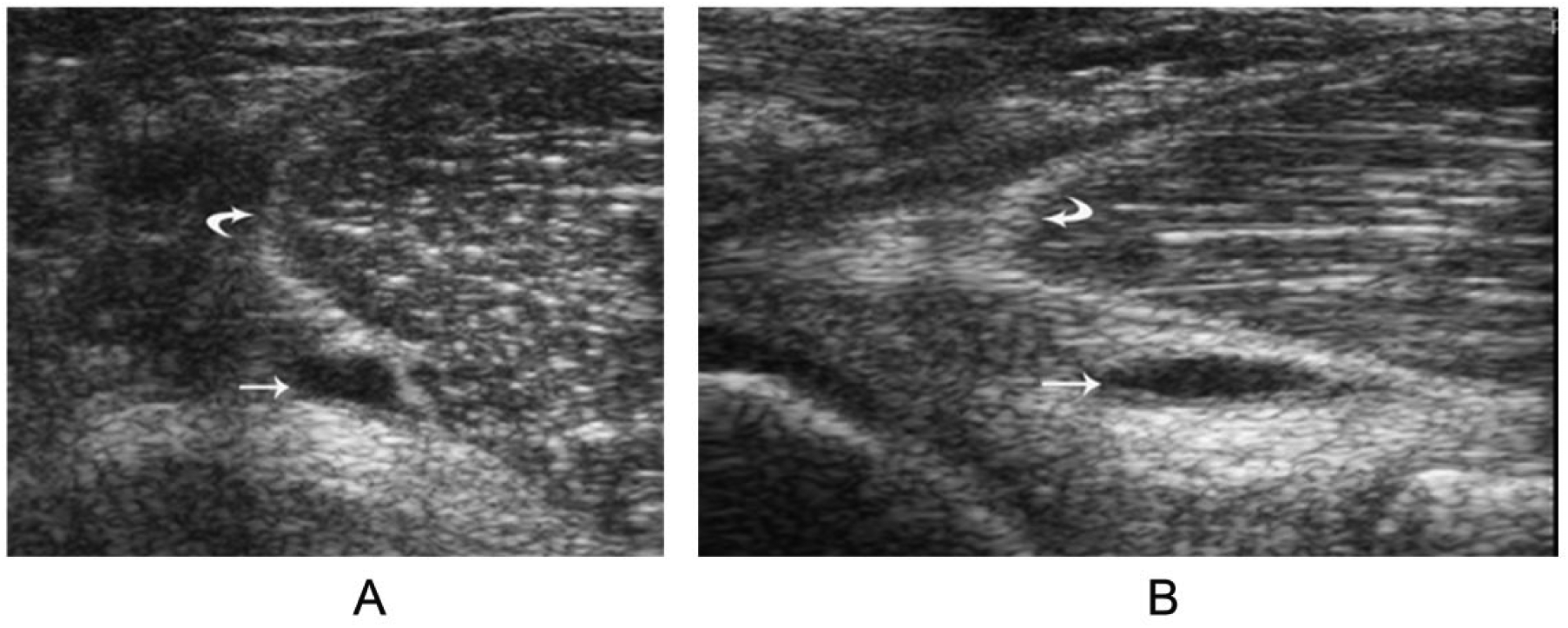
Atypical small Baker cysts refer to the small Baker cysts without the typical appearance. They are usually located at or adjacent to the cross section of the SMT and the MHG. On transverse view, their shape can be eyedrop or slit (Figure 6A, B).21,22 No matter what shape they are on transverse view, their most important anatomic characteristic is that on longitudinal view they are all located just superficial to the MHG. Sometimes these cysts are very small and can be easily overlooked (Figure 6C). These atypical tiny Baker cysts may be the very early development stage of typical Baker cysts.
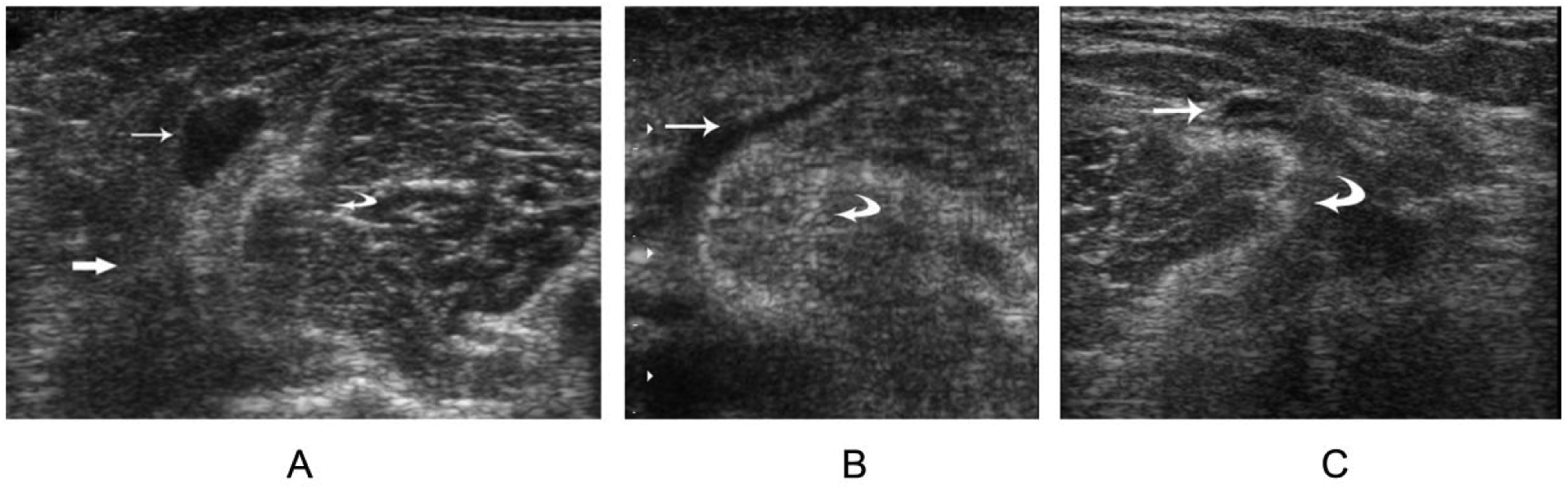
Transverse image: (A) eyedrop shaped, (B) slit shaped, (C) a tiny Baker cyst. Baker cyst (thin arrow), the medial head of the gastrocnemius (curved arrow), and the semimembranosus tendon (thick arrow).
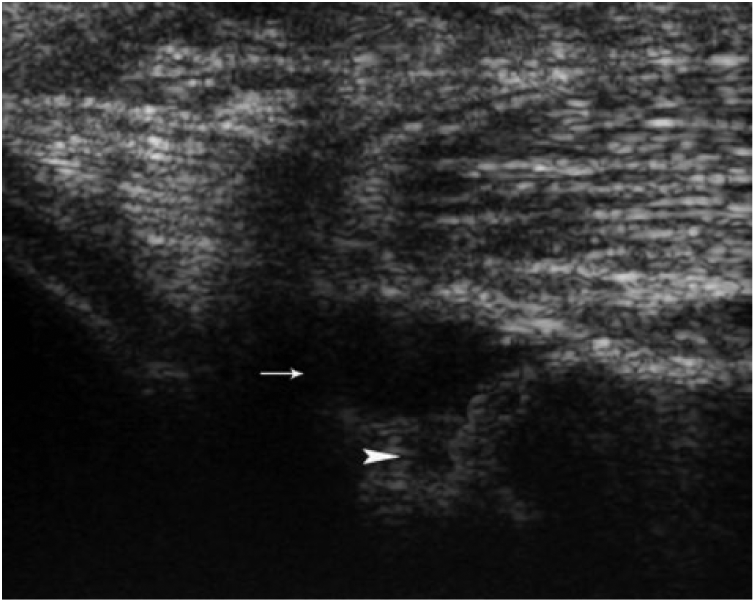
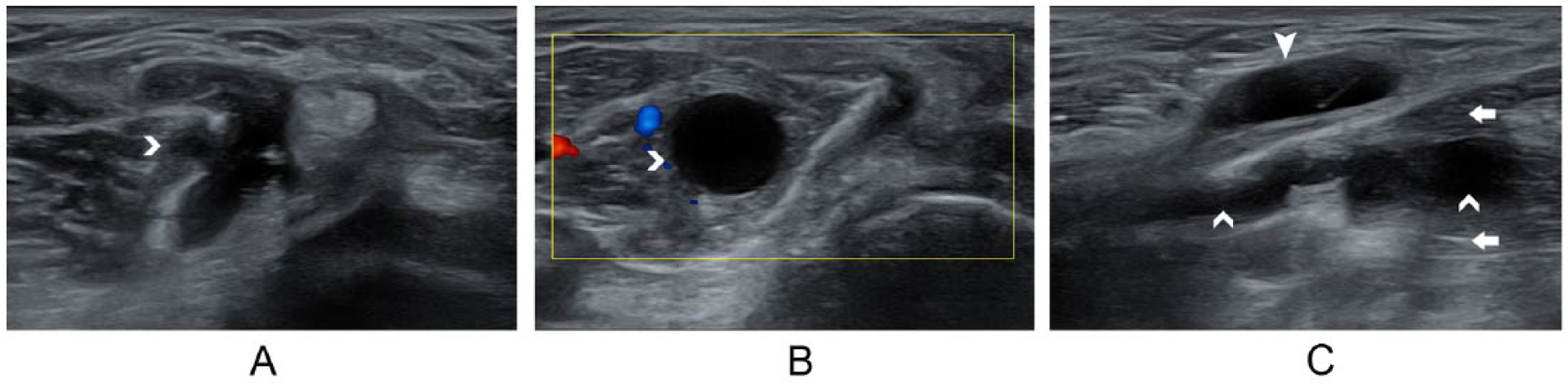
A Baker cyst with a tube shape on longitudinal view is a presentation that needs to be differentiated from a segment of the saphenous vein (Figure 7). 19 The latter is usually more superficially located (Figure 8). Furthermore, in transverse images, the segment of vein cannot be found between the SMT and the tendon of the MHG. Its vascular characteristics can eventually differentiate it from a true cyst: the vein is compressible; color or power Doppler results in color filling of the vein (lack of color filling due to slow blood flow may be reversed by augmenting flow in the calf); length extension can be observed with correct orientation of the probe. 19
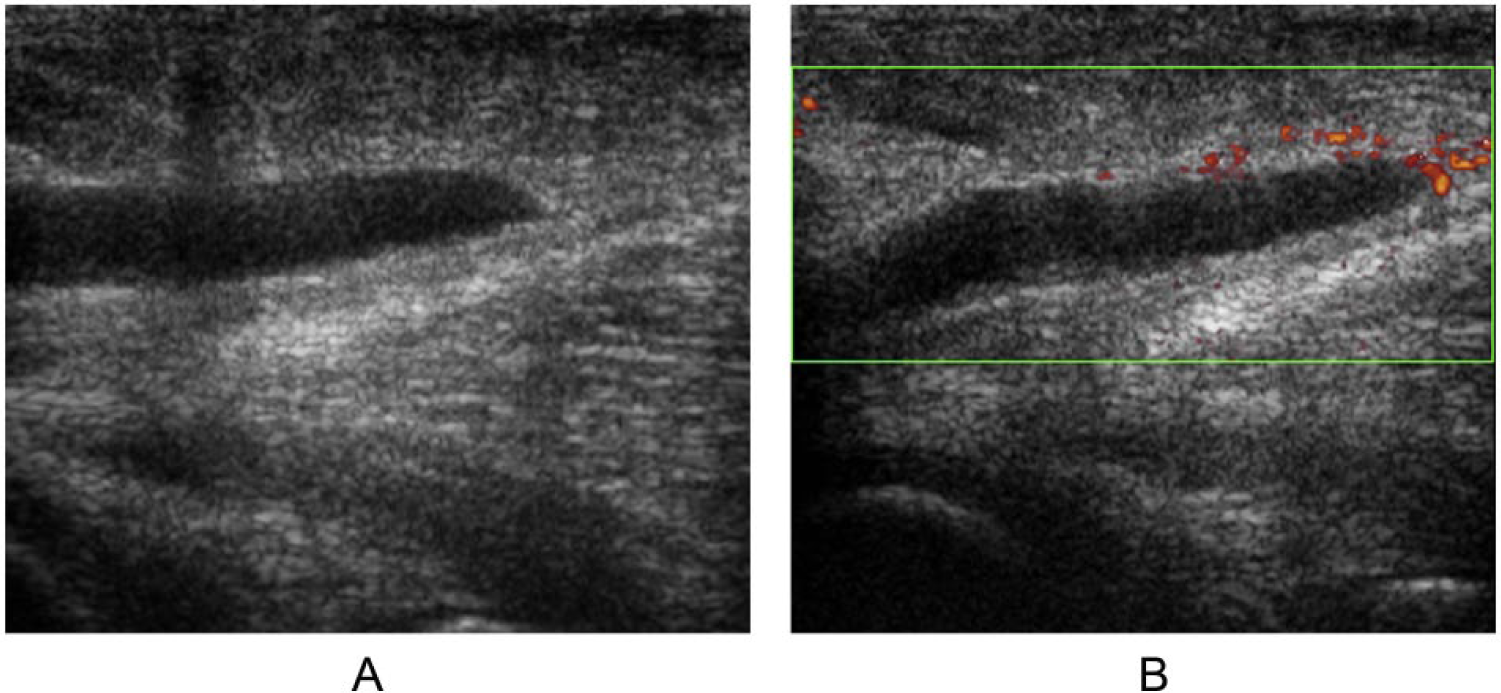
A vessel-like Baker cyst: (A) similar to a segment of vein in longitudinal image; (B) no color filling out the vessel-like cyst with power Doppler.
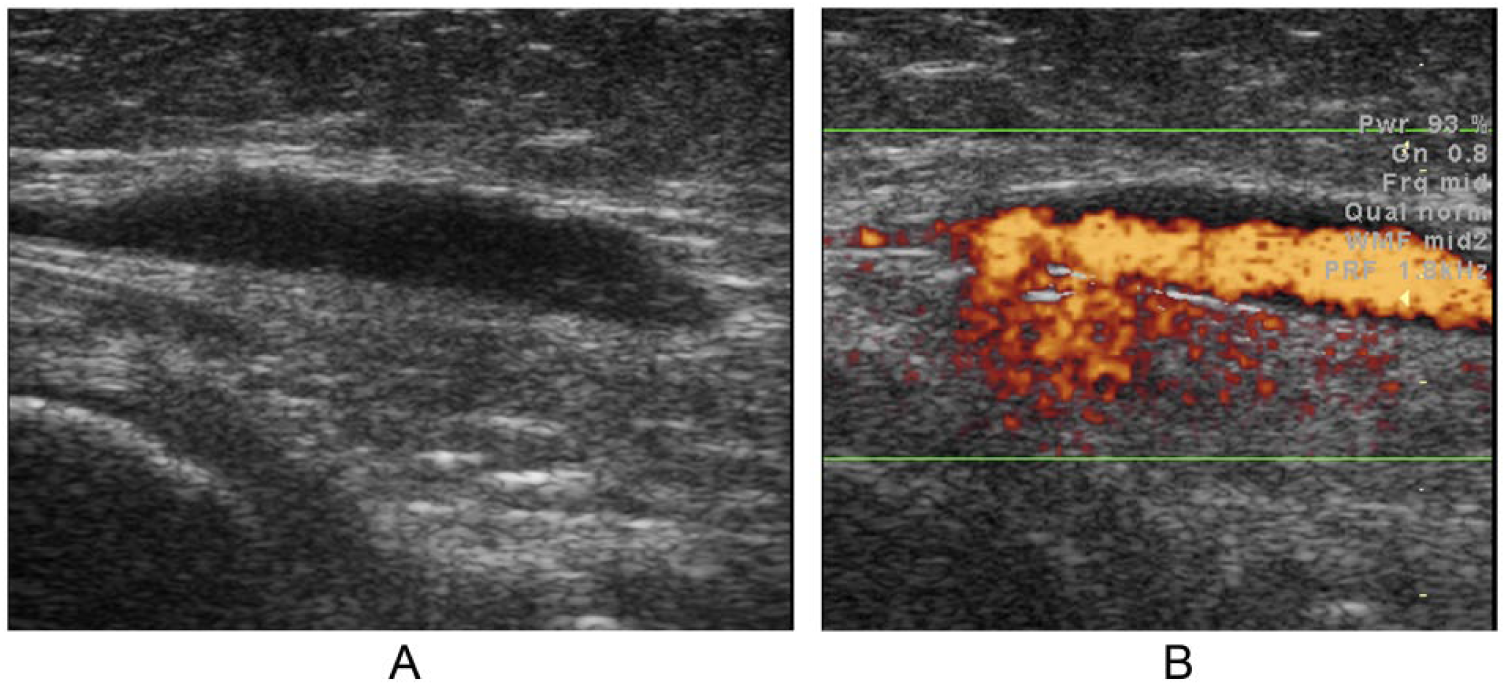
A cyst-like tortuous vein: (A) in longitudinal image; (B) power Doppler confirms its vascular nature.
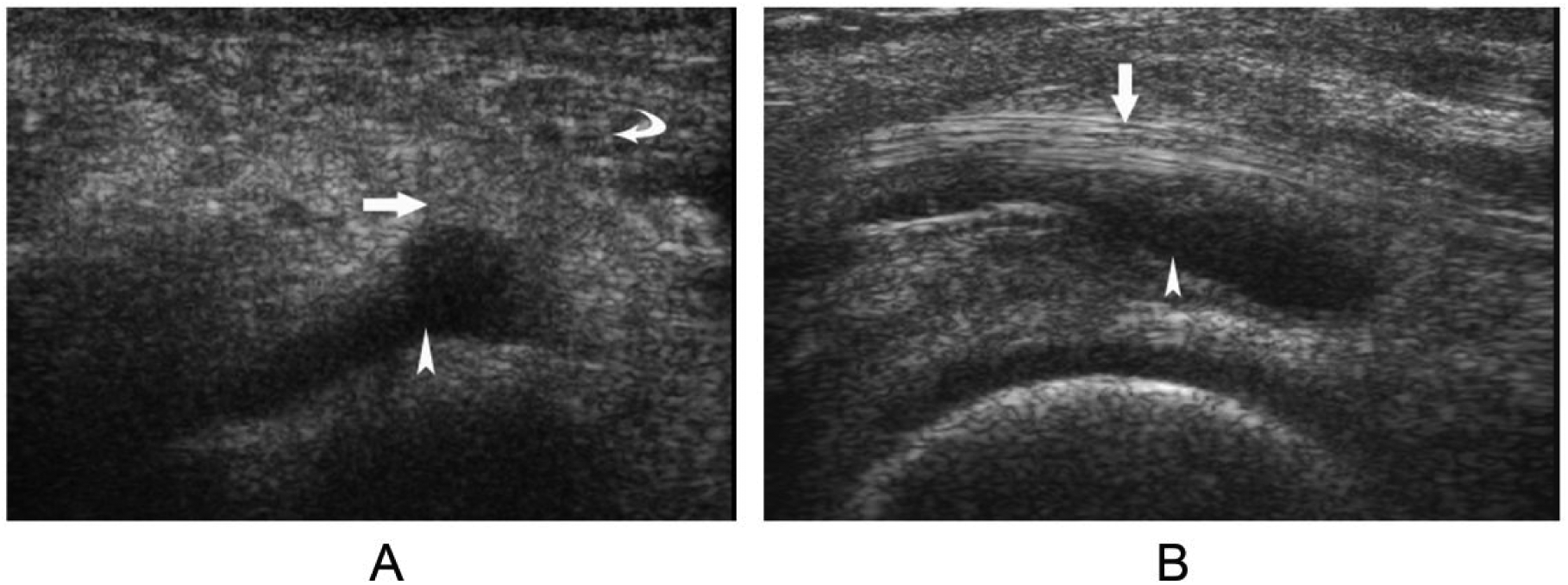
An uncommon variation is a cyst that is located deep to the tendon of the MHG (Figure 9), which is equivalent to the base part of a typical Baker cyst. It may be either the early stage of a Baker cyst or the independent deep lateral part of the G-S bursa separated from the rest of the bursa by a septum in the bursa. 21 The fluid in this kind of Baker cysts may come from the joint through the capsular opening. Since such a cyst is posterior to the medial joint, a meniscal cyst from the posterior horn of the medial meniscus may appear similar.19,23 Meniscal cysts are common disorders of the knee. In general, the shape of a meniscal cyst is irregular or lobular, while a Baker cyst has a smooth border and is oval in shape. Importantly, a meniscal cyst can usually be traced to the source at the posterior horn of the medial meniscus, and possibly a tear of the meniscus can be found (Figure 10). 19
A small cyst deep to medial head of the gastrocnemius: (A) transverse and (B) longitudinal views of the cyst (arrow) and the medial head of the gastrocnemius (curved arrow).
A meniscal cyst of the posterior horn of the medial meniscus in longitudinal images. A meniscal tear (arrowhead) was found connected to the cyst (arrow).
ʎ-Shaped Baker Cysts and Their Related Variations
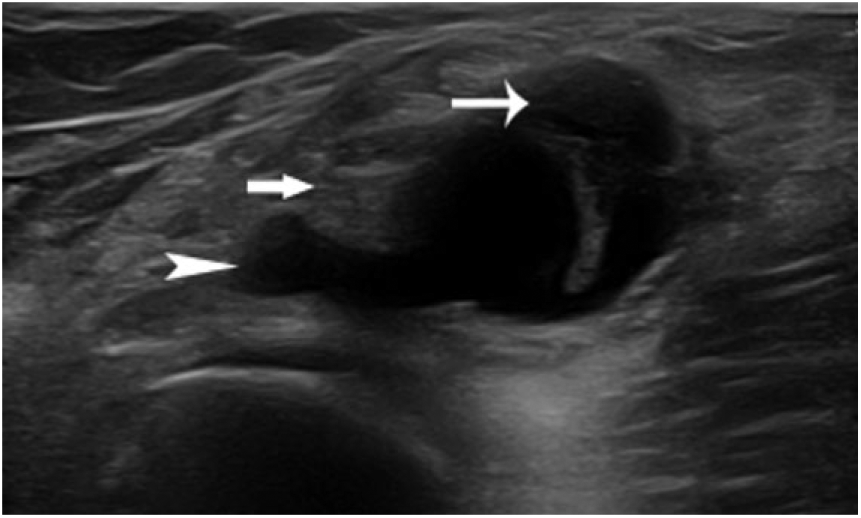
ʎ-Shaped Baker cysts on transverse view are occasionally seen (Figure 11A). This kind of Baker cyst can be viewed as a typical Baker cyst plus a deep medial addition. On longitudinal view, the deep medial part of the cyst should be observed deep to the SMT (Figure 11B). These cysts are also called X shaped because of the large body overlaying both the SMT and the MHG (Figure 12). 22 ʎ-Shaped Baker cysts may be developed from the distension of fluid in a bursa containing no septa; therefore, the distension involves all parts of the bursa: the superficial, deep lateral, and deep medial parts. In some situations, the anisotropy of the SMT can mimic this ʎ-shaped Baker cyst on transverse view (Figure 13A). A clue to indicate that anisotropy might have occurred is that, superficial to the deep medial hypoechoic area, another small hypoechoic area, which is the semitendinosus tendon, can be seen. Rocking the transducer can help to confirm the pair of hypoechoic areas represents the two tendons (Figure 13B). 21
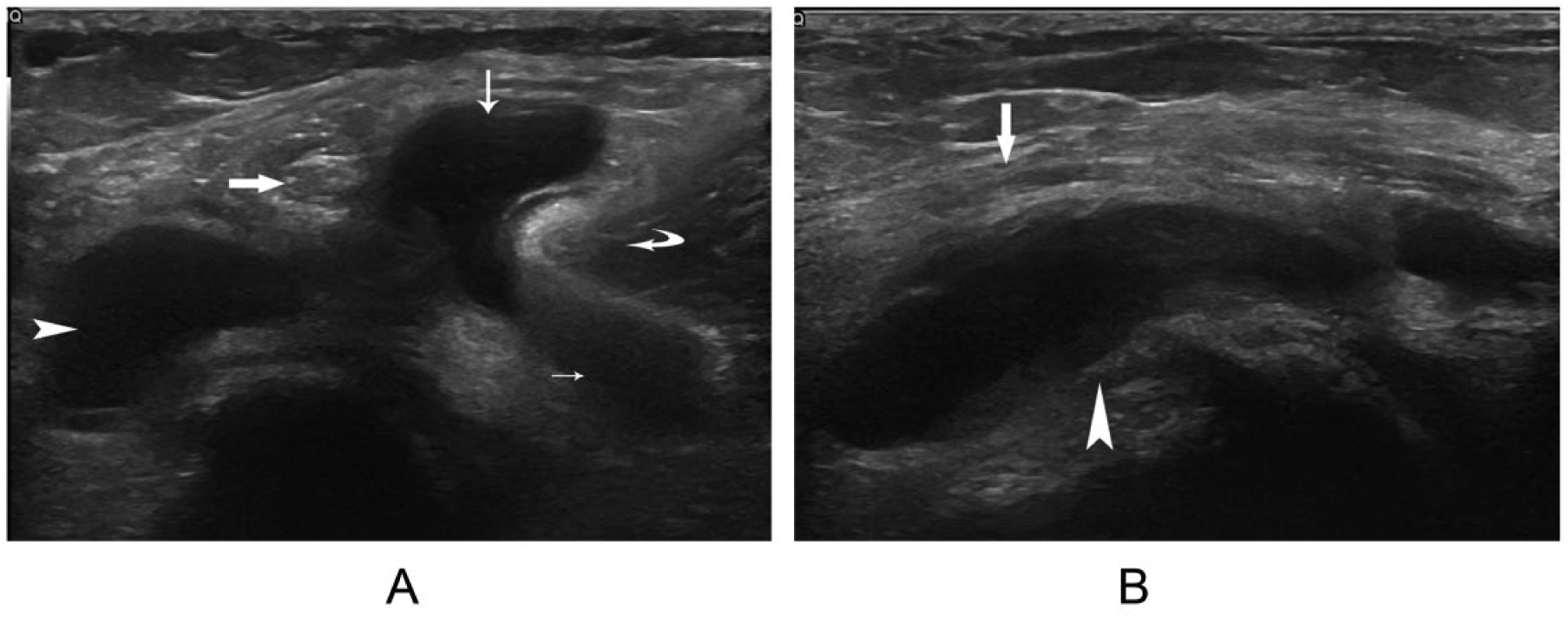
ʎ-Shaped Baker cyst. (A) Transverse image with the superficial part (long arrow); the deep medial part (arrowhead), which is deep to the semimembranosus tendon (thick arrow); and the deep lateral part (small arrow), which is deep to the medial head of the gastrocnemius (curved arrow). (B) The deep medial part of the cyst in longitudinal image.
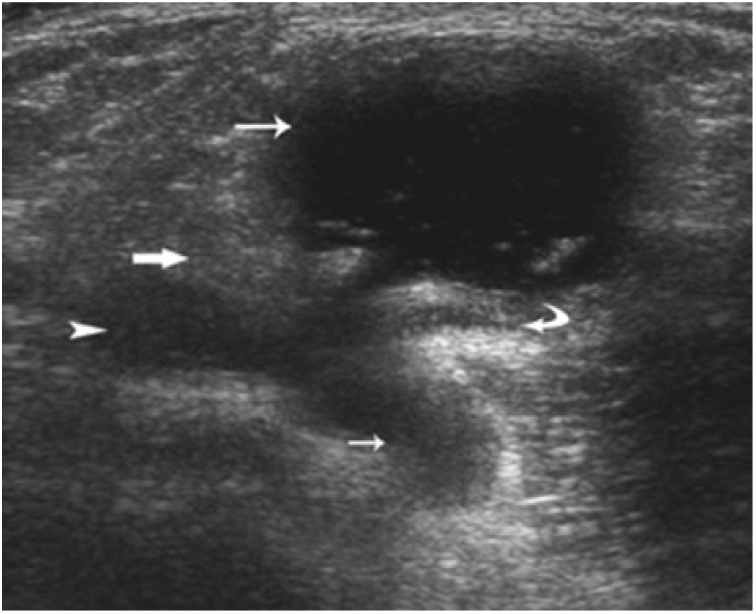
X-shaped Baker cyst. Transverse image with the superficial part (long arrow); the deep medial part (arrowhead), which is deep to the semimembranosus tendon (thick arrow); and the deep lateral part (small arrow), which is deep to the medial head of the gastrocnemius (curved arrow).
False ʎ-shaped Baker cyst: (A) the semimembranosus tendon (thick arrow) and the semitendinosus tendon (arrowhead) with anisotropy effect; (B) without anisotropy effect.
Sometimes a ʎ-shaped Baker cyst without the deep lateral part (base part) on transverse view can be seen (Figure 14). One possibility for this phenomenon is that the effusion in the deep lateral part of the bursa is so small that it cannot be visualized properly. Another possibility is that it is formed by the effusion due to the bursitis of the independent bursa separated from the deep lateral part of the G-S bursa by a septum because the deep medial part of the bursa has no communication with knee joint.13,21
ʎ-Shaped Baker cyst without the deep lateral part in transverse image: the body of the cyst (thin arrow), the deep medial part (arrowhead), and the semimembranosus tendon (thick arrow).
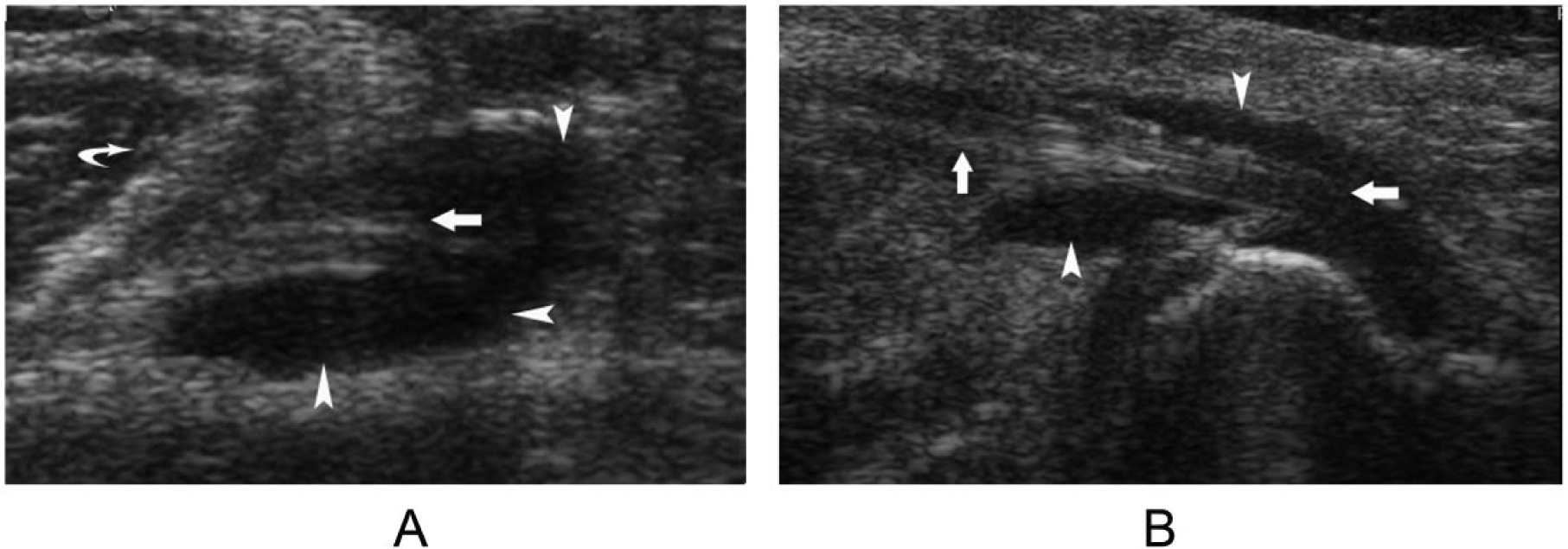
A Baker cyst that presents only the base part of a typical Baker cyst in atypical small Baker cysts may be another variation of the ʎ-shaped Baker cysts (Figure 9). The presentation of a Baker cyst with only the deep medial part of a ʎ-shaped Baker cyst on transverse view may suggest that the bursitis of the independent deep medial part of the bursa separated from the rest of the G-S bursa by a septum (Figure 15). 13 The reason is that joint fluid cannot enter this part of the bursa. This variation needs to be differentiated from the effusion of the semimembranosus bursitis, especially when the fluid distension is at the lower third of the bursa, where it also lines the SMT superficially. The semimembranosus-tibial collateral ligament bursa, commonly referred to as the semimembranosus bursa, is an inverted U-shaped bursa surrounding the central tendon of the semimembranosus. It is located at the insertion site of the tendon at the posteromedial aspect of the tibial epiphysis.13,24 The deep portion of the bursa lies between the tendon and the posterior aspect of the medial tibial condyle, while the superficial portion is located superficially to the tendon and lies between the tendon and the medial collateral ligament. They are connected superiorly along the anterior margin of the SMT. 25 Semimembranosus bursitis is usually due to impingement of the bursa against the osteophytes of the medial tibia. 24 Mild bursitis is usually confined to one portion of the bursa, either superficial or deep. The entire bursa may be affected in severe cases of bursitis, including the superficial, deep, and connection portions. Transverse images show a cyst surrounding the SMT in the three regions, while longitudinal images may show the tendon traversing the cyst (Figure 16). If a cyst around the SMT has its distal end adjacent to the level of the medial condyle of the femur but proximal end high in the popliteal fossa, it may be a Baker cyst. If its proximal end is below the medial condyle of the femur, semimembranosus bursitis is more likely. 21
ʎ-Shaped Baker cyst with only the deep medial part. (A) The cyst (arrowhead) is deep to the semimembranosus tendon (thick arrow) and medial to the medial head of the gastrocnemius (curved arrow) in transverse image. (B) The cyst is deep to semimembranosus tendon in longitudinal image.
Semimembranosus bursitis. (A) The effusion of the bursa (arrowhead) wraps the semimembranosus tendon (thick arrow) in the superficial, deep, and medial aspects in transverse image. The medial head of the gastrocnemius (curved arrow) is also seen. (B) The effusion of the bursa is near the insertion of the semimembranosus tendon in longitudinal image.
Baker Cysts With Extension Into Nearby Muscles
Baker cysts may expand in any direction, but they tend to expand in the intermuscular planes or spaces between muscle and knee capsule.3,18 Baker cysts with extension into nearby muscles are rare. Thus far, only six cases have been reported in the literature.18,26,27 Among them, two cases are with extension into vastus medialis muscle, and four cases are with extension into the MHG muscle. However, only two cases with extension into the MHG muscle were reported in an ultrasound study. 27 The breakthrough points of the extension into the MHG from the two sonographic cases are adjacent to the neck and the base of the cyst, respectively. They extend distally in the MHG in a cone or tube shape (Figure 17). The proposed pathogenesis is that weakened muscle fascia or a constitutional focal defect of the muscle fascia may predispose to penetration by an expanding cyst under pressure.18,26 Chronic microinjury may cause fascia weakness or defect. 27
Baker cyst extends into the medial head of the gastrocnemius (MHG) near the neck of the cyst. (A) A connection between the extension (chevron) in the MHG and the Baker cyst in transverse image. (B) The extension (chevron) in the MHG became larger in transverse image. (C) Longitudinal view of the MHG (arrow), a cone-shaped extension in the muscle with its bottom toward the inferior aspect of the MHG. The body of the Baker cyst (arrow head) could be seen superficial to the MHG.
Baker Cysts With Complications
The complications of a Baker cyst include rupture, hemorrhage, and infection. Among them, the most common one is rupture, while the rare one is infection. 1 Baker cyst rupture is usually associated with physical activity. Since the rupture mostly happens in the body of the cyst, leaked fluid can spread in adjacent tissue, especially the distal subcutaneous tissue or calf muscles (Figure 18A). 1 Patients usually feel sudden sharp pain in the posterior of the knee, followed by swelling in the calf, symptoms that are similar to a deep vein thrombosis and need to be differentiated. 28 Sonographically, a ruptured Baker cyst shows partial or complete emptying of the cyst and anechoic fluid collections in nearby soft tissue. However, occasionally, the rupture is so tiny that the fluid in the cyst leaks slowly without causing acute symptoms. Patents may complain of being uncomfortable or having swelling in the posterior knee or calf. Intracystic hemorrhage may be seen in a cyst as hypoechoic content partially filling the lumen (Figure 18B).
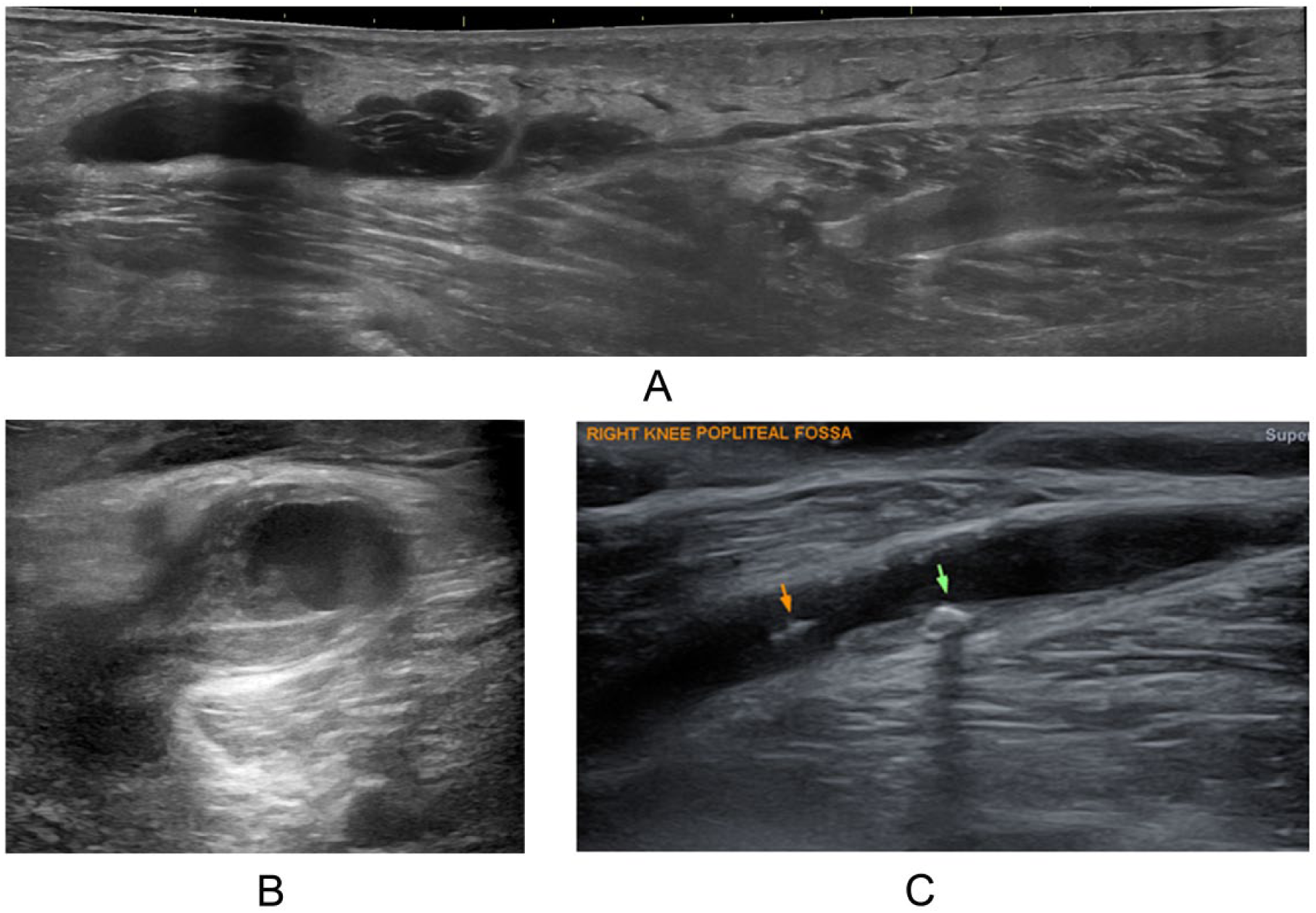
The complications of Baker cysts. (A) A ruptured Baker cyst with irregular outline of the low half and fluid spreading in subcutaneous tissue in longitudinal panoramic view. (B) Hemorrhage in a Baker cyst with hypoechoic content and a thickened wall in transverse image. (C) Loose bodies (arrows) in a Baker cyst in longitudinal view.
The existence of loose bodies in a Baker cyst is common. They may be migrated from the joint through the communication channel, 22 or they may arise by synovial osteochondromatosis in the cyst, which is an indirect complication of Baker cysts. 29 The benign metaplasia of the cells in the synovial membrane enables them to produce cartilage nodules on the inner surface of the synovial membrane (chondromatosis). When the nodules are broken off, the free cartilage nodules may undergo calcification or ossification (osteochondromatosis). They are usually multiple and in small, even size. 29 Loose bodies in Baker cysts may be osseous, chondral, or osteochondral fragments. They may be the result of fragmentation of the joint surface or osteoarthritis, fracture of the osteophytes, or synovial osteochondromatosis in the joint or in Baker cysts. Osseous and osteochondral loose bodies are relatively common. Sonographically, the bony or calcified loose bodies appear as hyperechoic foci with posterior acoustic shadowing, like gallstones (Figure 18C). 1 Sometimes the cysts are small and filled only with loose bodies without fluid inside. In this situation, the Baker cysts can easily be overlooked. An important clue is the shadowing of the loose bodies.
Conclusion
Baker cysts have a wide spectrum of sonographic appearances. The article covers most of the possible presentations of Baker cysts. Other presentations may be encountered in clinical practice. Retaining comprehensive knowledge of Baker cysts is important for the recognition and diagnosis of the cysts.
Footnotes
Acknowledgements
I thank Dr. Andrew Lata, radiologist and medical director of our department, for his kind support, dedicated time to review this manuscript, and critical advice on it.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.