
Abstract
Pseudoaneurysms of the lateral plantar artery (LPA) are rare. In this case study, a very rare case of a pseudoaneurysm of the LPA, caused by a knife cut, is reported. A female adult patient presented with a growing lump in the arch of the left foot for 4 weeks. She had an accidental steak knife stab her on the arch of the left foot and had the cut sutured 5 weeks prior. The physical examination revealed a warm, pulsatile, and tender lump without a clear border deep to the scar in the lateral arch. Duplex ultrasonography (DUS) detected a cavity with the wall uneven in thickness and the outer wall undistinguished. Doppler demonstrated a typical Yin-yang sign inside the cavity and a neck-like structure connecting the cavity to an artery along the path of the LPA, suggesting that this was a LPA pseudoaneurysm, caused by penetration trauma. Later, the patient received priority surgery to have the pseudoaneurysm repaired.
Keywords
A pseudoaneurysm, or false aneurysm, is a local hematoma with internal swirling blood flow, which comes through the wall defect of an adjacent artery due to damage to the arterial wall. The hematoma is contained by surrounding tissue without any layer of the vessel wall.1,2 Pseudoaneurysms of the lateral plantar artery (LPA) are rare, and most of them are iatrogenic. 2 LPA pseudoaneurysms caused by penetration trauma are very rare. Only a few cases have been reported in children and just two cases in adults.2–7 They all were caused by glass penetration except one by a nail. In this report, an adult LPA pseudoaneurysm caused by a knife cut is presented. It is also the first duplex ultrasonography (DUS) study of the LPA pseudoaneurysm.
Case Report
A 69-year-old woman was referred for a sonographic examination due to a growing lump in the arch of the left foot for 4 weeks. Five weeks earlier, she had an accidental steak knife stab on the arch of the left foot during a trip visiting relatives, in a foreign country. The wound was sutured in the emergency room of a local medical center. Four weeks earlier, she noticed a lump in the arch of the foot. It was painful when she extended her toes or pressed on it, and it was gradually growing in size. After she had returned from abroad, she went to see her general practitioner (GP) and was referred to the lab for a sonographic examination. She had been taking anticoagulant medicine, Eliquis 5 mg, twice a day for 4 years due to carotid stenosis. Physical examination revealed a scar about 4 cm in the lateral arch almost perpendicular to the long axis of the foot. A palpable lump without a clear border was deep to the scar. The lump was warm, pulsatile, and tender.
A sonogram of the left foot plantar aspect was performed with a linear high-frequency transducer (6–15 MHz) using the General Electric (GE) LOGIQ S8 ultrasound equipment system. In the lump region, an oval-shaped cavity was identified deep to the plantar fascia, measuring 4.9 cm × 4.3 cm × 3.0 cm. The inner wall of the cavity appeared smooth, while the outer wall appeared undistinguished. The wall also appeared uneven in thickness. Pulsatile swirling of mild hyperechoic content could be observed in the cavity during the live scanning (see Figure 1). Color Doppler showed a typical Yin-yang sign in the cavity (see Figure 2A). Power Doppler demonstrated rhythmic blood bursting into the cavity through a neck-like structure on transverse view of the foot (see Figure 2B). The proximal connection vessel of the cavity through the neck-like structure could be seen along the path of the LPA on the long axial view of the foot (see Figure 3A), while its distal connection of the LPA could be seen on an oblique long axial view of the foot (see Figure 3B).
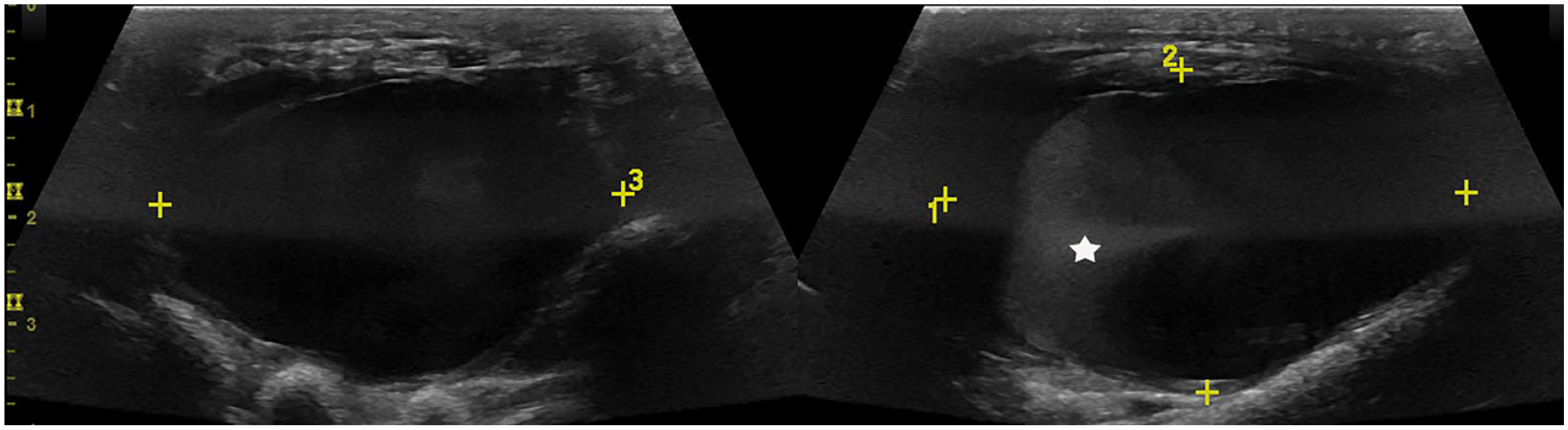
Oval-shaped pulsatile cavity. The wall was uneven in thickness, and the outer wall was undistinguished. Mild hyperechoic swirling (star) could be seen inside (right panel).
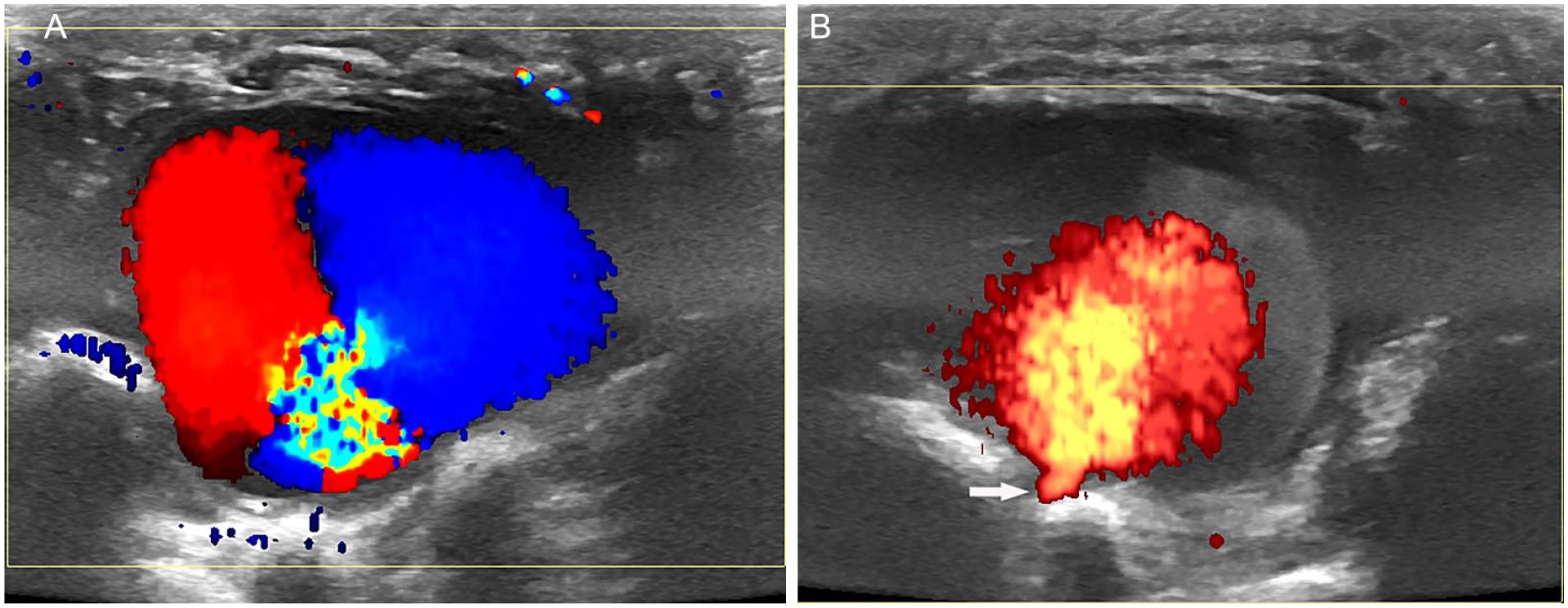
The Doppler characteristics of the cavity. (A) Color Doppler Yin-yang sign in the cavity. (B) Rhythmic blood bursting into the cavity through the neck-like structure (arrow) under power Doppler.
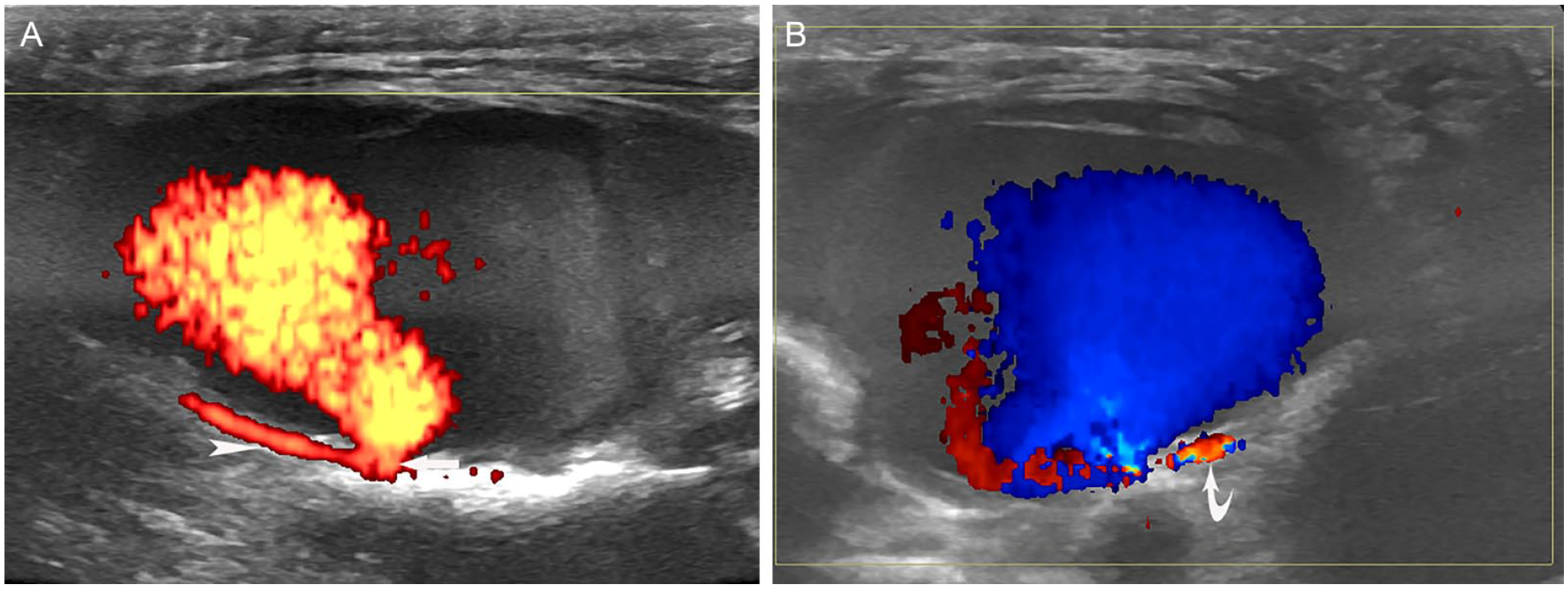
The relationship of the cavity with adjacent lateral plantar artery (LPA). (A) On long axial view, the neck of the cavity connected proximally with LPA (arrow head). (B) On oblique long axial view, the neck connected distally with LPA (curved arrow).
After this DUS examination, the patient was referred to an emergency room in a hospital by her GP. She was admitted to the vascular surgery department. Before the surgery, another DUS was done in the hospital, which confirmed the existence of this pseudoaneurysm. Surgical repair of the pseudoaneurysm was performed. A follow-up DUS examination detected no abnormality in the arch of the left foot 6 months after the surgery.
Discussion
Plantar arteries of the foot are mainly from the posterior tibial artery, which passes posterior to the medial malleolus and bifurcates into the medial and lateral plantar arteries. Comparing with the medial plantar artery (MPA), the LPA is thicker and is more like a continuation of the posterior tibial artery. It crosses the sole of the foot laterally toward the level of the base of the fifth metatarsal bone to form the plantar arterial arch, in which the medial aspect is joined by the deep plantar artery from the dorsalis pedis artery.5,8 The proximal half of LPA passes deep to the abductor hallucis and flexor digitorum brevis muscles, while the distal half passes deep to the plantar fascia, but superficial to the quadratus plantae, and lateral to the flexor digitorum brevis. The MPA passes along the medial aspect of the sole toward the first metatarsophalangeal joint, where it branches to the first toe and the first plantar metatarsal region. The path of this artery is deep to the abductor hallucis, quadratus plantae, and flexor hallucis longus muscles5,8 (see Figure 4).
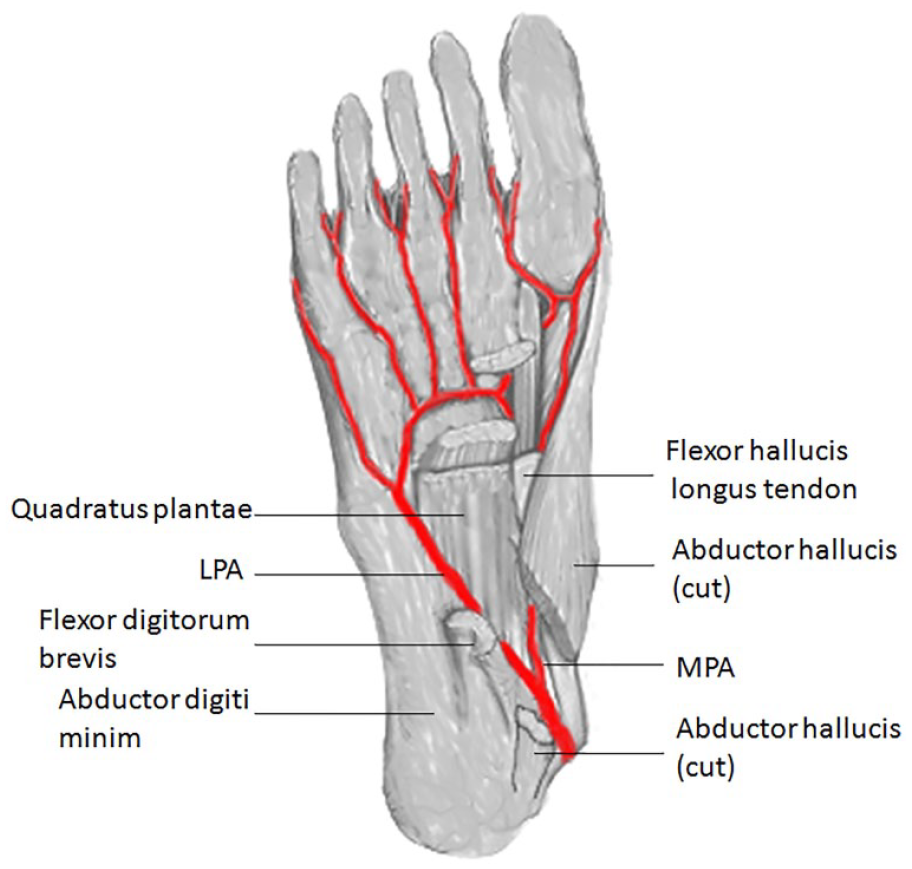
The anatomy of the plantar arteries. The LPA (lateral plantar artery) and MPA (medial plantar artery).
Clinically, patients with plantar pseudoaneurysms usually have significant local trauma history, either iatrogenic or penetrating. Most plantar pseuduoaneurysms caused by penetration trauma were reported in the LPA, with fewer in the MPA.9,10 The reason may be that the distal half of LPA lies in a relative superficial location, where it is deep only to the plantar fascia, and is susceptible to penetration injury.2,5,11 In contrast, the MPA lies deep to multiple muscles in the sole, which is more protected from a penetration injury.5,8 A pulsatile mass or local swelling may be the only sign of plantar pseudoaneurysms. 5 This patient had a knife cut at the left foot arch. The pulsatile mass in the injured area appeared 1 week later. DUS demonstrated a pulsatile cavity with typical color Doppler Yin-yang sign inside, and a neck-like structure connecting the blood-filled cavity to an artery. These suggest an aneurysm. Since the outer wall appeared undistinguished, and the wall appeared uneven in thickness, the aneurysm may be a false one, pseudoaneurysm. Combining the patient history, physical sign, and DUS findings, the diagnosis of pseudoaneurysm associated with penetration trauma can be made. Furthermore, the pulsatile mass was on the lateral aspect of the arch, and the artery connected to the pseudoaneurysm was along the path of LPA, which is the main artery in the area and just deep to the plantar fascia. Therefore, it is deduced that this is a pseudoaneurysm of the LPA.
It seems clear that the formation of this pseudoaneurysm originated from the knife cut. The defect of the cut might have been tiny and was not recognized during the surgical suture procedure. The anticoagulant medicine that this patient was taking might help prevent clot formation in the defect of the injured artery, which allowed blood passing to develop an adjacent hematoma. The hematoma was recanalized gradually to form a cavity, which connects to the lumen of LPA via the neck-like structure at the defect of the artery wall. In the meantime, the wall of the cavity became fibrotic.2,3
There are multiple imaging modalities for the diagnosis of a pseudoaneurysm. DUS is usually the first choice. It is non-invasive, inexpensive, easily repeatable, dynamic, and without ionizing radiation. 12 Furthermore, it is reliable in detecting the size, morphology, flow, and feeding vessels of a pseudoaneurysm. 13 It is especially useful when repeating imaging studies are required. DUS scanning of the current case provided excellent assessment of the above mentioned indices and was also confirmed by a repeated study before surgery. Computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are alternative choices for imaging and diagnosing a pseudoaneurysm. They both can provide more accurate and detailed information of a pseudoaneurysm. However, they are either radiation exposure or limited accessibility, and need intravenous contrast media. 3 Hence, they are used when precise measurements, imaging of the pseudoaneurysm anatomy, and the collateral circulation assessment are needed before surgery. 3
The complications of a pseudoaneurysm occur when it grows large enough. It can compress adjacent nerves or vessels to cause symptoms. The most serious complication is a pseudoaneurysm rupture. Its wall consists of organized hematoma and fibrous tissue without tensile strength of an artery, which has the potential to rupture. 2 Since the risk for rupture is high, immediate medical intervention is needed once a diagnosis of pseudoaneurysm is established. 5 The treatment of a pseudoaneurysm includes non-surgical and surgical methods. Non-surgical methods are used to induce spontaneous thrombosis in the pseudoaneurysm. They include external or ultrasound-guided compression, and ultrasound-guided thrombin injection into the pseudoaneurysm. 14 Surgical methods include repair of the pseudoaneurysm and vascular reconstruction. Usually a simple repair, as the current patient received, is effective, because the foot has good collateral circulation. 5
Conclusion
A pulsatile mass or swelling of the foot arch after an obvious penetration trauma is an alarming sign of plantar artery pseudoaneurysms. DUS is the first choice among the diagnostic imaging modalities. The sonographic diagnostic indices of LPA pseudoaneurysms include a color Doppler Yin-yang sign in a pulsatile cavity with the wall uneven in thickness and the outer wall undistinguished, and the cavity connecting to an artery along the path of the LPA via a neck-like structure. Immediate medical intervention is needed to prevent pseudoaneurysm rupture.