
Abstract
Two participants of a similar age and progression of COVID-19 diagnosis are presented. Each individual displays artifacts consistent with COVID-19 infection and recovery. Sonographic evaluation is utilized to view the state of their lungs, after infection. However, the observed healing patterns vary between the young adults. Variation in healing due to behavioral factors, such as vaping, are possible. The intent of this case study is to alert sonographers to the sonographic lung changes that may be attributed to COVID-19 and lingering symptomatology.
SARS-CoV-2 is a coronavirus discovered in 2019 that causes COVID-19. COVID-19 is a respiratory disease that spreads via aerosolized droplets and causes symptoms that range from mild to severe. 1 Young adults may contract the COVID-19 virus and experience mild to severe illness, but according to the Centers for Disease Control and Prevention (CDC), the incidence of SARS-CoV-2 in younger populations is less than that of adults.2,3 The true proportion of young adults affected by SARS-CoV-2 has increased since March 2020, but it is difficult to measure due to the lack of testing and the emphasis on adult viral spread. 3 Nevertheless, all populations should be assumed to possess the same viral loads and a similar incubation period. 3
Young adults may exhibit a range of presenting complaints from being asymptomatic to highly symptomatic. The symptoms of COVID-19 in young populations include, but are not limited to, fever, loss of taste or smell, shortness of breath, or nausea. 2 A recent meta-analysis reported that 16% of children are asymptomatic; however, further evaluation suggests the true proportion may be closer to 85% of COVID patients are asymptomatic. 4 Despite a seemingly low incidence of COVID-19 in young adult populations, the group remains at risk for developing severe symptoms. It has been reported that one in three young adults hospitalized for SARS-CoV-2 were admitted to the intensive care unit. 3 The children who experience a severe illness from SARS-CoV-2 are often due to underlying medical conditions, such as obesity, diabetes, and acute lung conditions. 3
Younger COVID-19 patients have been admitted to the hospital less frequently than adults. 3 The overall lack of young adult hospitalizations for COVID-19 pneumonia could be misleading whereas many were recovering at home. The diagnosis of SARS-CoV-2 is established mainly from a nasopharyngeal swab. Nasopharyngeal swabbing detects the genetic material of SARS-CoV-2 by the process of reverse transcription polymerase chain reaction (RT-PCR). 5 RT-PCR testing operates by amplifying small portions of DNA for genetic analysis. 6 Such testing has low sensitivity, so other methods have been adopted. Nevertheless, the National Institute of Health still advocates for testing via nasal or salvia sample. 7 Regardless, SARS-CoV-2 evaluations have been made using computed tomography (CT) as a diagnostic alternative. 8 A CT examination has an appropriate diagnostic sensitivity but remains costly and inappropriate for routine use in young adults. Lung ultrasonography (LUS) provides a point of care technique for diagnosing and monitoring SARS-CoV-2. 9 The use of LUS is more appropriate as it ensures safety for younger populations. A LUS is a quick diagnostic technique, which reduces ionizing radiation exposure, and is cost effective. Sonography also provides a fast and accurate diagnostic approach for consistently monitoring of COVID-19 pneumonia. 9 The use of a lung scoring system allows for the quantification of both CT and lung sonograms. 9 The quantification of lung images has been attempted by several authors; however, the modified lung ultrasound system (mLUS) is a popular point-of-care method. The mLUS scoring system requires the assessment of the pleural line, pulmonary parenchyma, and general complications, to create a comprehensive score of the upper and lower anterior, lateral, and posterior lung windows. 9 Utilizing an RT-PCR test coupled with LUS is a non-invasive and non-ionizing diagnostic approach to detect COVID-19 infection. 10
Given the need to provide surveillance of potential viral disease, a non-ionizing and non-invasive set of diagnostic tests were needed. LUS is a non-ionizing technique for detection of infection of the lungs and its progression. The modified ultrasound system was employed to evaluate two participants. Both participants, who are 20 years old, tested previously as positive for SARS-COV-19. Through LUS, the state of the lungs, post-COVID-19 infection, was evaluated. These participants were covered by our institutional internal review board approval (IRB:2021H0448).
Case Report
Participant 1
A twenty-year-old male, who tested positive for SARS-CoV-2, via RT-PCR testing in August of 2020, took part in a COVID-19 surveillance testing program and was asymptomatic at the time of testing. A quarantine period of 10 days, in university housing, was required upon notification of his positive test. This participant experienced body aches, fever, and loss of taste and smell during this time period. The fever reached its peak at 104°F on the second night of isolation; however, the fever persisted for 4 days at 100°F. After isolation was completed, this participant had lingering symptoms of SARS-CoV-2. The lack of his sense of smell was most notable and did not return until the following year.
The participant consented to participate during a pilot phase of a young adult COVID study. The IRB-approved research imaging examination included a limited sonographic examination of the lungs, heart, kidneys, and the completion of the EuroQol (EQ) survey. The EQ survey is used to allow participants to record their self-rated health score, based on five dimensions. 11 This participant had no lingering symptoms or “long COVID-19,” 12 at the time of examination, but detailed use of vape products and his frequency as being once an hour.
Participant 2
A second participant is a healthy, 20-year-old male who tested positive for COVID-19, via RT-PCR testing, in August 2020, and took part in a COVID-19 surveillance testing program. This participant had no symptoms at the time of testing but was recently in contact with COVID-19 positive individuals. A quarantine period of 10 days was fulfilled in personal housing, after receiving the positive result. Two days after testing positive, this participant began to experience symptoms of COVID-19 pneumonia, such as fatigue, a cough, chest pain, and a fever. After fulfillment of the quarantine period, this participant had few remaining symptoms of COVID-19 pneumonia.
This participant likewise consented to the pilot of the upcoming research study. His examination also included a limited sonographic examination of the lungs, heart, kidneys, and completion of the EQ survey. Since having COVID-19, this participant has experienced an infrequent cough. The second participant also reported a decrease in aerobic capacity since testing positive for SARS-CoV-2. Certain activities, like running, have become more difficult as a result. Such symptoms are still experienced today. He also self-reported as a non-smoker, including vaping.
Both participants were examined with a GE Logiq (GE Healthcare, Waukesha, WI) laptop ultrasound equipment system and a 2.5–3 MHz curvilinear and phased array transducer. A bilateral lung ultrasonogram focused on the pleural line, A-lines, B-lines, and lung sliding was completed for both participants using Lichtenstein’s imaging technique which is referred to as the bedside lung ultrasound in emergency (BLUE) protocol.13,14 The examinations were conducted by an experienced and credentialed sonographer. Participant 1 presented noticeable blurring of, and a fragmented, pleural line. He also had several sonographic windows that demonstrated consistent B-lines (see Figures 1–3). In addition, participant 1 had an artifact that separated the pleural line upon inspiration. His heart, renal, and EQ survey responses were unremarkable. The second participant did have demonstrable pleural line defects that appeared to be reuniting, or possible healing, but several sonographic windows continued to demonstrate pleural line artifacts (see Figures 4–7).
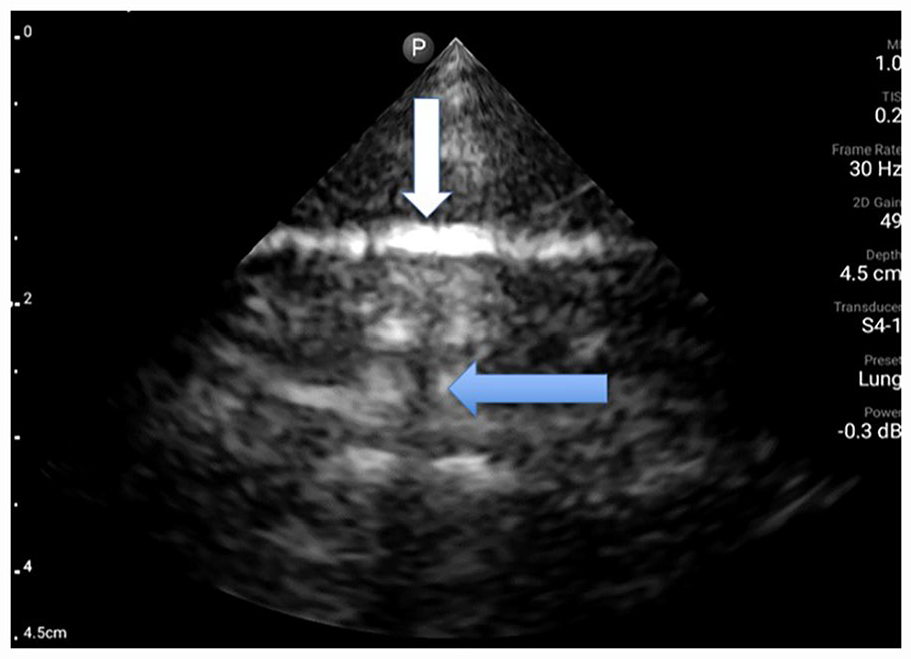
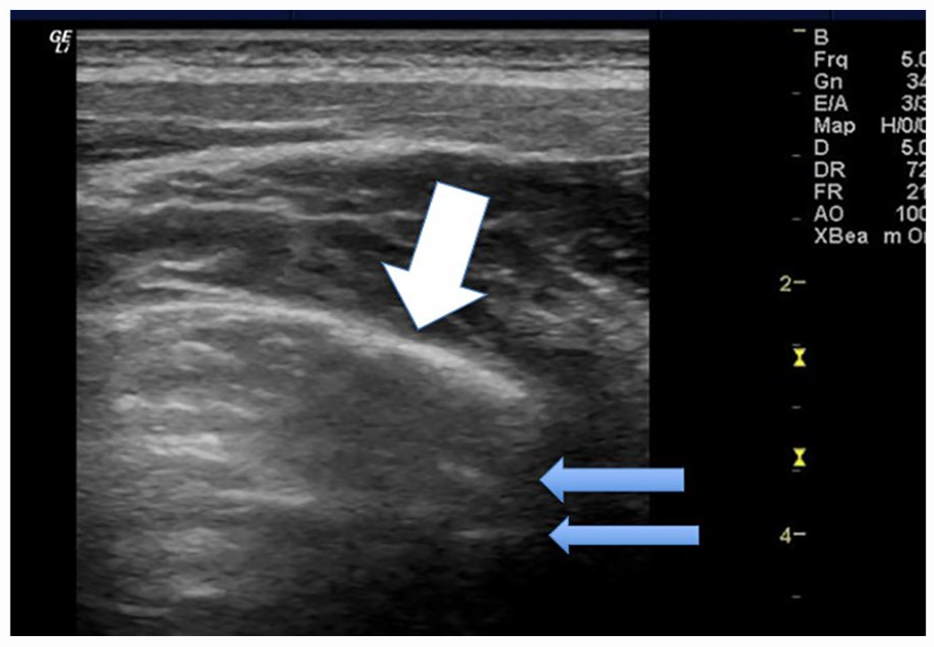
Sonographic image of participant 1 with an image taken of the right upper anterior BLUE point. The lung sonogram demonstrates a thickened pleural line as well as break denoted by the white arrow. The mLUS score for this defect is 1 point and 3 points for the discontinuous pleural line. Resultant B-line artifacts are also seen coming from the broken pleura. The mLUS score for this defect is 3 points for a fragmented pleural line and 1 point for <3 B-lines; therefore, a total of 8 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
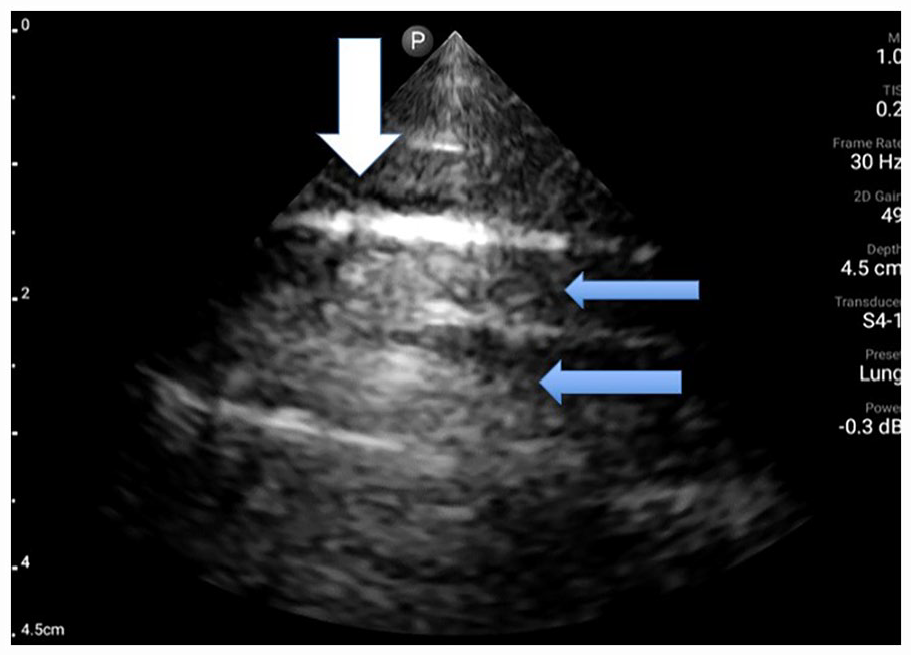
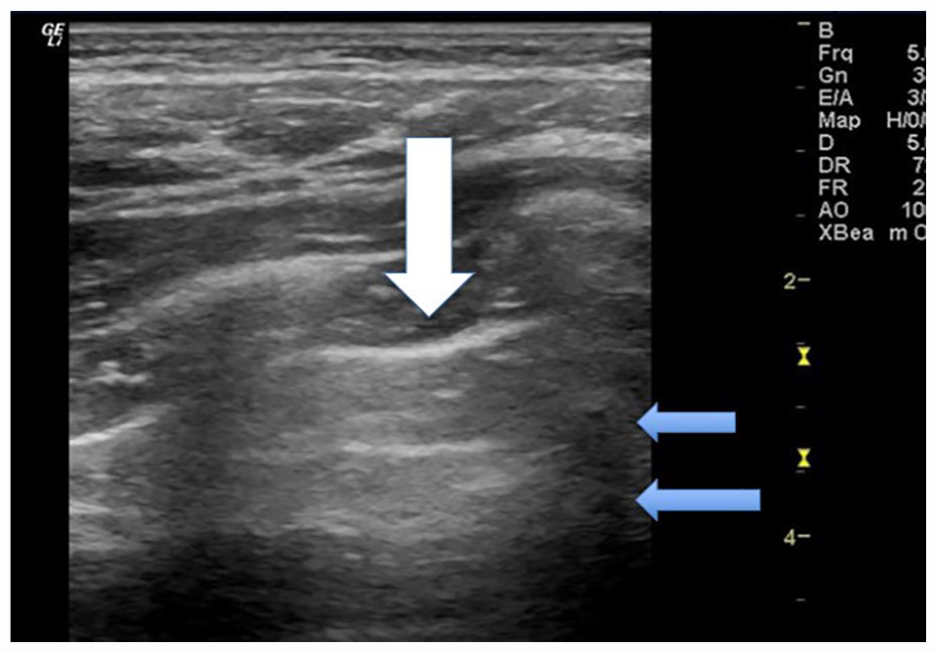
Sonographic image of participant 1 taken of the right upper posterior BLUE point. The lung sonogram demonstrates a thickened pleural line as well as break denoted by the white arrow. The mLUS score for this defect is 1 point and 3 points for the discontinuous pleural line. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 4 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
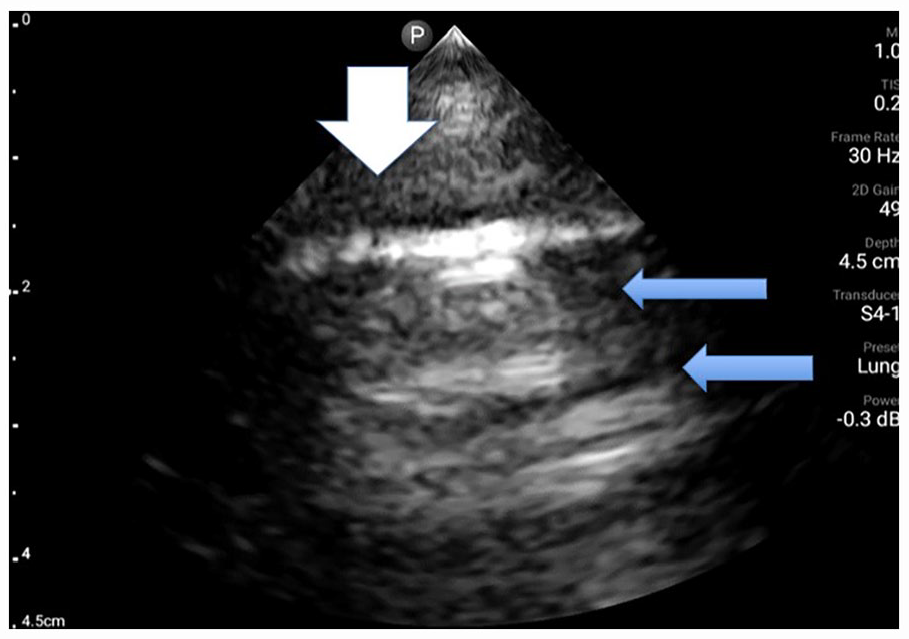
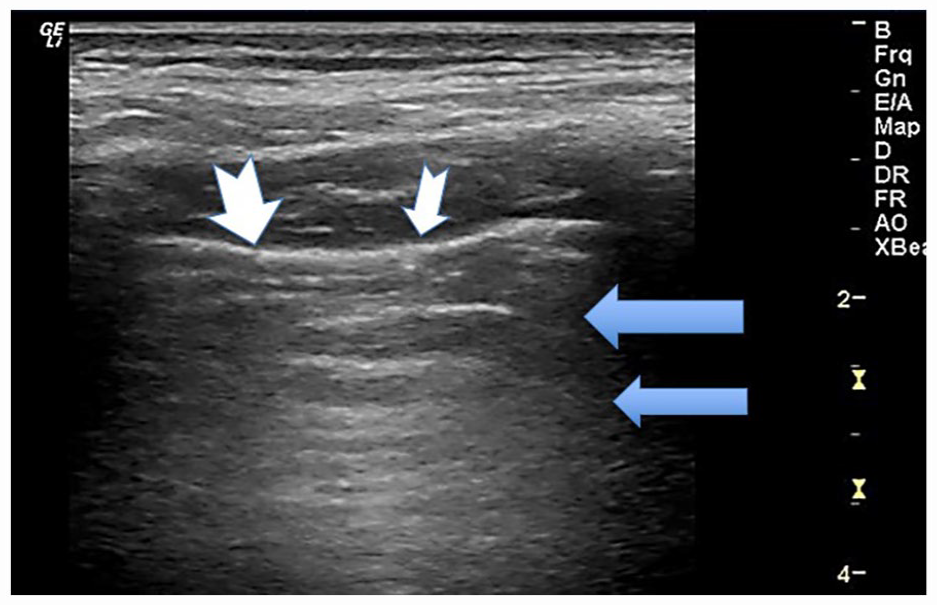
Sonographic image of participant 1 with an image taken of the left lower anterior BLUE point. The lung sonogram demonstrates a thickened pleural line as well as several breaks denoted by the white arrow. The mLUS score for this defect is 1 point for the thickening and 3 points for a discontinuous pleural line. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 4 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
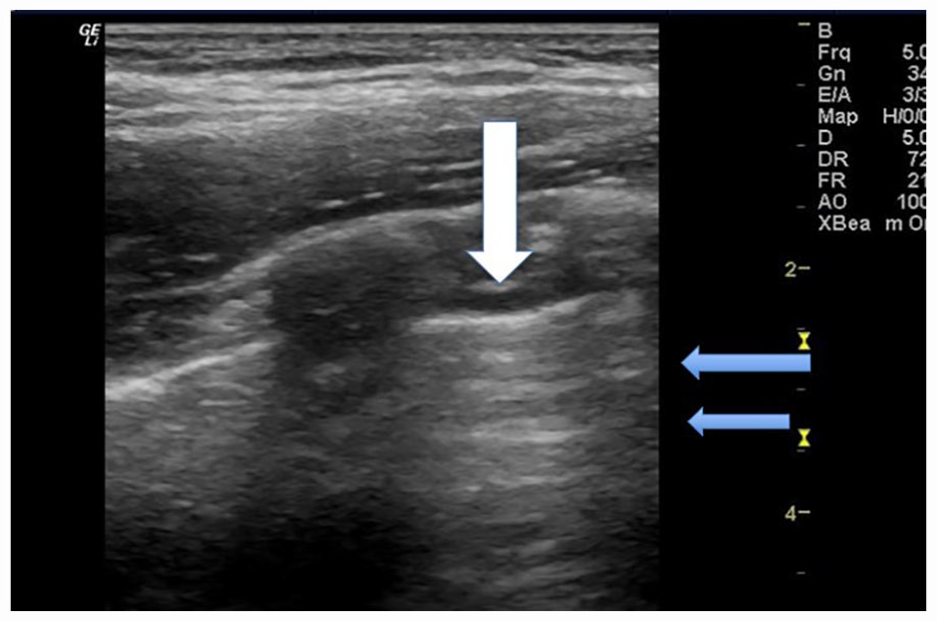
Sonographic image of participant 2 with an image taken of the right upper axillary BLUE point. The lung sonogram demonstrates a pleural line that measured <0.5 and is denoted by the white arrow. The mLUS score for this defect is 0 points for the pleural line. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 0 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
Sonographic image of participant 2 with an image taken of the right upper posterior BLUE point. The lung sonogram demonstrates a pleural line that measured >0.5 and is denoted by the white arrow. The mLUS score for this defect is 1 point and an additional 2 points for the blurred pleural line. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 3 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
Sonographic image of participant 2 with an image taken of the left upper axillary BLUE point. The lung sonogram demonstrates a pleural line that measured >0.5 and is denoted by the white arrow. The mLUS score for this defect is 1 point and an additional 2 points for the blurred pleural line. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 3 points is given just for this BLUE point window. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
Sonographic image of participant 2 with an image taken of the left lower posterior BLUE point. The lung sonogram demonstrates a pleural line that measured <0.5 and is denoted by the white arrow. The mLUS score for this defect is 0 points; however, on closer inspection, echogenic nodules were seen adhered to the pleural line so we did award an additional 2 points for the discontinuity. It is noted that there are few B-line artifacts and more normal A-line artifact, denoted by the blue arrow. The mLUS score for this lack of defect is 0 points; therefore, a total of 2 points is given just for this BLUE point window. It is important to note that on inspiration, these nodular areas on the pleura did tend to open and close. BLUE, bedside lung ultrasound in emergency; mLUS, modified lung ultrasound system.
The participants had a similar experience in their diagnosis of COVID-19, as both were asymptomatic at the time of testing. The first participant experienced more severe symptoms associated with SARS-CoV-2 coronavirus. The fever experienced by the participant was higher and over a longer time period. Participant 1 also experienced the loss of taste and smell for an extended amount of time. The second participant recovered more quickly in terms of time and experienced varied symptoms than the first participant.
The mLUS score was evaluated for the two participants. The comprehensive score includes upper and lower anterior, upper and lower axillary, and upper posterior windows, similarly to the pleural line evaluation. The total score is taken out of 34 points for a given side of the lungs, totaling 68. Each window is evaluated for the presence of B-lines. Participant 1 was given a score of 5/34 for the right side of the lungs, then 8/34 for the left side of the lungs. The windows alternated between a score of 1 or 2. A score of 1 indicates the presence of 3 B-lines. The score of 2 indicates 4 B-lines, or partially merged. The total score for participant 1 is 13/34. Participant 2 was given a score of 0/34 for the right side of the lungs, then 2/34 for the left side of the lungs. Every window, besides the left upper posterior, was awarded a score of 0. The left upper posterior was given a score of 2, indicating the presence of 4 B-lines or partially merged.
The score for complications, such as a pulmonary balloon, pneumothorax and empyema, or pleural effusion, is 0 for both participants (see Table 1).
A Modified Scoring System for Assessing SARS-COVID 19 Lung Disease.
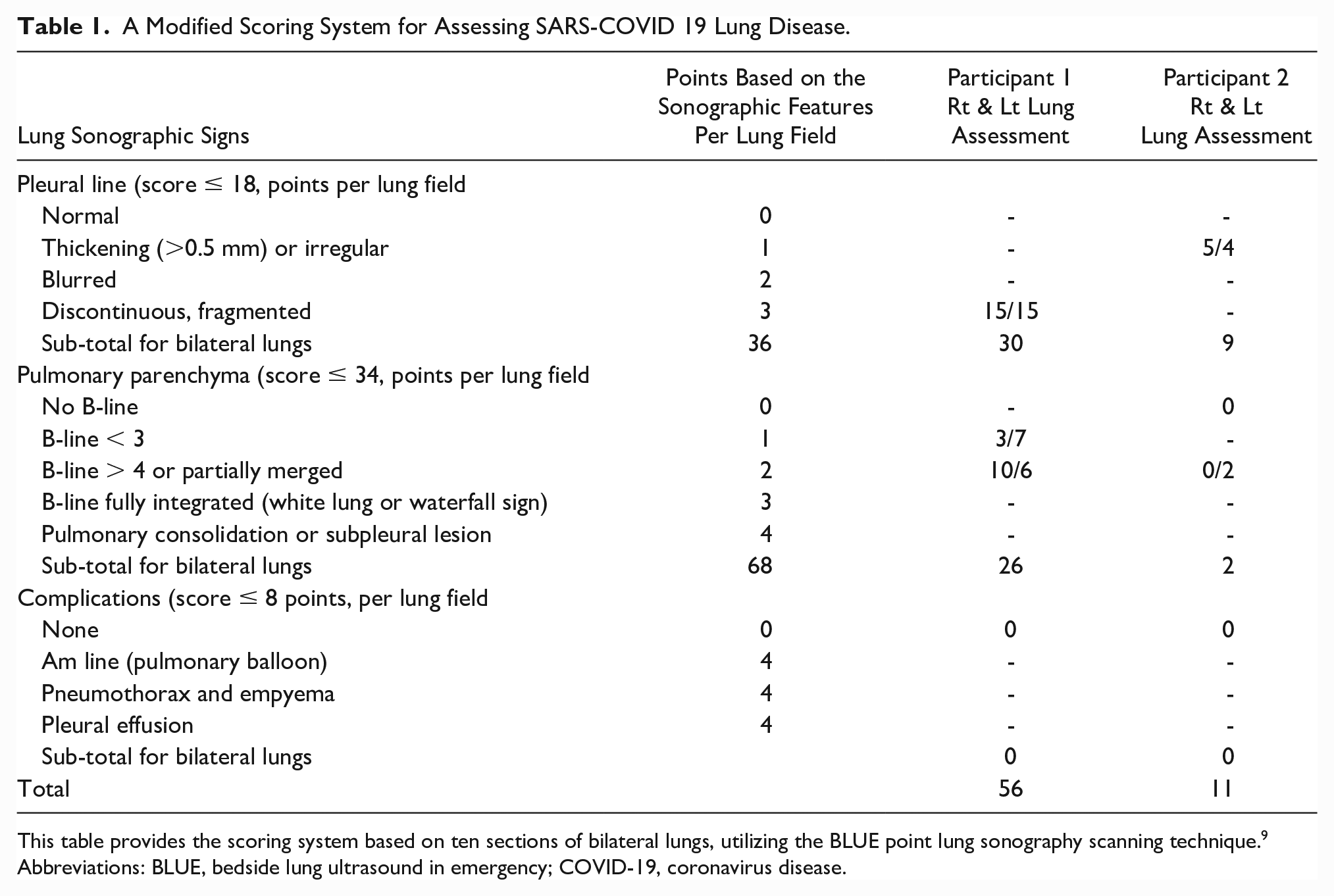
This table provides the scoring system based on ten sections of bilateral lungs, utilizing the BLUE point lung sonography scanning technique. 9
Abbreviations: BLUE, bedside lung ultrasound in emergency; COVID-19, coronavirus disease.
Despite these diagnostic findings, the first participant was not experiencing any respiratory symptoms, post-COVID. The only health concerns detailed were heart palpitations upon vaccine administration and stress-induced irritable bowel syndrome. The sonographic findings within the lungs could be associated with COVID-19 or lifestyle choices, such as a high frequency of vaping. The second participant mentioned dyspnea when engaging in exercise and an infrequent cough. The incidences pair closely in the timeline with recovery from COVID-19 but may be attributed to lifestyle changes at a pivotal point in life.
Discussion
The lungs are a key part of the respiratory system. The respiratory system supplies oxygen to the body to support life. Specifically, the lungs push oxygen into the bloodstream, which is carried throughout the body. In addition to exchange of gasses, the system aids in body temperature maintenance, filtering of foreign elements, and aiding sense of smell. 15 Individual lung function can be impacted by obesity. Although our participants were not overweight, obesity is known to decrease lung volume; therefore, strength and resistance are decreased. 16 The pleura is a membrane folded onto itself that surrounds each lobe of the lungs to separate the lung from the chest. 15 During LUS, a distinguishable artifact is the pleural line, or the boundary between the soft tissues and the lung tissues. The pattern of the pleural line is referred to as “the bat sign” where the upper and lower ribs appear as two wings and the pleural line serves as the body of the bat (see Figure 7). Recognition of this pattern is especially useful to differentiate from other hyperechoic lines. 17 In COVID-19 cases, the thickening of the pleural line with irregularity is common. 18 Alteration in appearance of the pleural line can be attributed to thickening and excess fluid in the interstitial tissues and pleura. 18
The progression and resolution of symptoms in COVID-19 patients has been closely observed in health care settings. Information is presented with the appropriate knowledge of COVID-19, at the time of this study. Clinicians have turned to different diagnostic parameters beyond RT-PCR, due to inconsistencies and the need to monitor patient’s health post-COVID. 18 Evaluation of COVID-19 has been monitored with CT, chest radiography, and lung sonograms. CT should be considered with caution due to the level of radiation exposure. The repeated use of CT could also lead to increased viral exposure to health care workers and in critical cases of COVID-19 and transportation of these patients can be precarious. 19 The emergency department and intensive care unit often order chest radiographs to establish a diagnosis, but this imaging modality has shown low accuracy for detecting COVID-19 specific pathology. 19 In comparison to CT and chest radiography, LUS can be a comparable diagnostic option. The results of lung sonograms are proportional to those of CT, but limit radiation exposure while allowing for replication and low cost in the clinical setting. 19 Patients are only exposed to non-ionizing radiation from lung sonograms; therefore, its use with symptomatic children and pregnant women can be completed and repeated for disease surveillance. 18 LUS is a point of care diagnostic technique; therefore, occupational exposure can be more limited, and patients are scanned at the bedside. LUS should be considered a competitive diagnostic option for clinicians trying to detect acute or chronic COVID conditions. 19
The pilot participants have many similar characteristics as far as their age, gender, education, social setting, and time of contracting COVID-19. Despite being in good health prior to infection, each participant had a prolonged recovery and continue to experience lingering effects that they believe are attributed to having had COVID-19. Artifacts are worth noting following recovery. Both infection and recovery from COVID-19 can vary for those with comorbidities. Comorbidities associated with COVID-19 pneumonia are hypertension, cardiovascular and cerebrovascular conditions, and diabetes. 20 Patients with comorbidities are more likely to face intensive care unit admission and mechanical ventilation. 21 Those facing COVID-19 alongside comorbidities can face an alternative recovery route than those without. Comprehension on the infection and recovery periods cannot continue without proper research, including imaging.
The mLUS scoring system was published by Tan et al. 9 It is based on the assessment of 12 regions of the lung. 9 The mLUS was utilized in this case study. A comprehensive score includes upper and lower anterior, upper and lower axillary, and upper posterior windows (see Table 1). Regarding the pleural line scoring, participant 1 had a score of 15 for the right side of the lungs and a score of 15 for the left side of the lungs. Each score is taken out of an 18-point system, and more points is considered to equate to great disease burden. The overall score was 30/36 pleural line examination. The comprehensive score is established from the appearance of the pleural line in the anterior, axillary, and posterior windows. To receive a score of a 3, which was established in every window, the pleural line must appear discontinuous and fragmented. Participant 2 was given a score of 5 for the right side of the lungs, then a score of 4 for the left side of the lungs. The overall score for the pleural line examination is 9/36 in participant 2. The scores of 0 and 1 were awarded in each of the windows. The pleural line will appear normal when given a score of 0. A score of 1 will indicate an irregular or thickened pleural line but is not blurred.
Interestingly, both participants had different lung sonographic results with participant 1 demonstrating continued pleural line discontinuations and resulting B-line artifacts (Figures 1–3). Conversely, participant 2 demonstrated pleural line “flaps” that appeared to be united until he took deep breaths (Figures 4–7). These pleural line partial unifications may be evidence of healing, but without prior imaging, this would be impossible to determine. Interestingly, the differences in the number of pleural line breaks and the mLUS scores are significant. The most notable difference is that participant 1 was a regular vaping product user. Individuals who smoke or vape could be at a higher risk of developing an infection or lung injury. 22 Studies have suggested that aerosols used in vape products can decrease the lung’s response to infection while damaging tissue and causing inflammation. 22 Injuries within the lungs associated with vaping are present in the form of diffuse B-lines 23 (see Figures 1 and 3).
The evaluation of COVID-19 by LUS is completed by addressing artifacts and quantifying the overall occurrence through quantitative scoring. The pattern of artifacts are “A-lines” and “B-lines.” A-lines are the horizontal repetition of the pleural line. The repetition of A-lines occurs due to the reflection of the transducer and lung tissue 19 (Figures 4 and 7). Differentiation of the A-lines and the pleural line can be made based on the localization of the “bat wing” on the images (Figure 4). The second pattern presented is B-lines. B-lines are identified as a “comet-tail” sign that begins at the pleura and fades before reaching the edge of the screen (Figures 3 and 7). The artifacts occur as sound waves pass through the soft tissue and pleura, then encounter a mixture of water and air. B-lines originate from fluid in the pulmonary interstitial space. 19 The amount of B-lines present indicates the state of interstitial pathology. 19 In the study participant’s comparisons, the recognition and ability to provide serial imaging would help to determine whether lung and pleural irregularities can be tracked to resolution.
Conclusion
Two male long-COVID participants underwent sonographic examination of their lungs, kidneys, and hearts, along with completing the EQ survey. Both participants presented with lung abnormalities. It cannot be guaranteed that these abnormalities are directly related to COVID-19, but this case study warrants the monitoring of long-COVID patient lungs via sonography. In the comparison of two male participants who were experiencing prolonged symptoms and demonstrable lung sonography artifacts, surveillance of their course of healing was paramount. Due to their age and need for ongoing diagnostic imaging, lung sonography is the most suitable means for documenting changes in their lung tissue.
The case study presented provides low-level evidence in evaluating two singular participants. Further research on a larger cohort of individuals is needed. Such research would determine whether this method could be used to discover underlying causes of long-COVID and guide patient treatment.
Footnotes
Acknowledgements
The primary author is grateful for receiving some financial support (OSU STEP funds) for analysis of data, manuscript preparation, and publication of this article.
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board, and the submitting Editor/Associate Editor had no involvement in the decision-making process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from The Ohio State University (2021H0448).
Informed Consent
This was made available to the participants as part of our OSU IRB approval 2021H0448.