
Abstract
Bilateral hydrocele of the canal of Nuck (HCN) is very rare, in adult females. Primary care physicians can misdiagnose this pathology without diagnostic imaging. A 37-year-old female complained of right lower quadrant (RLQ) pain, for a few months, reported to the emergency room. A non-reducible bulging protrusion was visualized in the RLQ. After performing the necessary blood work, the emergency physician ordered an emergent sonogram and computed tomography (CT). A transvaginal sonogram was performed to exclude gross adnexal masses, in the RLQ. An HCN canal was suspected in the right inguinal region. A non-contrast CT demonstrated a bilateral HCN, with the left significantly smaller than the right. In this case, a bilateral surgical excision of the hydrocele was recommended. Owing to the recurrence of the HCN, a cyst aspiration was not suggested. Physicians should consider the diagnosis of HCN in any female presenting with inguinolabial swelling. Sonography, CT, and magnetic resonance imaging (MRI) are the three diagnostic imaging techniques commonly used to diagnose this pathology. A multimodality approach is sometimes necessary when the sonography diagnosis is no definitve.
The Dutch anatomist, Anton Nuck, first described the canal of Nuck in 1691. 1 The hydrocele of the canal of Nuck (HCN) is an infrequent entity in adult females.2,3 HCN is often misdiagnosed as an inguinal hernia or an incarcerating inguinal mass, which can result in improper clinical management. 4 Some have considered HCN equivalent to the male hydrocele of the spermatic cord. 5 It can occur anywhere adjacent to the round ligament of the uterus, from the deep inguinal ring to the labia. 6
Embryologically, the persistent processus vaginalis, in the inguinal canal, of females has been referred to, as the canal of Nuck.7,8 In both males and females, the gubernaculum and the processus vaginalis play a significant role in developing the inguinal canal. In females, the patent processus vaginalis within the inguinal canal tends to obliterate by the first year of ex-uterine life. 9 The canal of Nuck rarely may not be obliterated even during adulthood and thus may manifest various pathologies in this region. The hydrocele of the canal of Nuck is one of the several pathologies evident in this region, with an incidence rate of less than 1%. 10 Some have considered the incidence of HCN to be eight times rarer than the male communicating hydrocele. 11 Bilateral HCN is even rarer occurrence, in adult life. The patient presentation may range from asymptomatic to severe tenderness in the groin region, typically without nausea or vomiting. 12
The canal of Nuck consists of two layers: the outer fibrous layer and the inner wall lined by single-layered mesothelial cells. The canal of Nuck can eventually lead to hernias or hydroceles, among females. 4 Hydroceles are formed in the canal of Nuck when there is an imbalance between the fluid secretion and absorption from the inner mesothelial wall.11,13 There are three types of HCN, and understanding this classification is essential since the management may differ among the three designations.1,11 A type I HCN does not communicate with the peritoneal cavity and appears as an encysted structure in the groin region. It is the most common type of HCN reported in the literature.6,14 Type II HCN directly communicates with the peritoneal cavity and may result in an indirect inguinal hernia. 13 A common recommendation is to use a laparoscopic approach to correct a type II HCN. 1 A type III is the rarest and can appear on diagnostic imaging, with an “hourglass appearance,” due to constriction at the deep inguinal ring.4,13 The superior encysted portion does not communicate with the peritoneal cavity, while the lower does. 1 Wang et al recently published their work and classified HCN into four categories based on the anatomic location. Using Wang’s classification, a type A HCN is located subcutaneously over the inguinal canal, a type B HCN is situated in the inguinal canal, and a type C is limited to the internal inguinal ring. 2 The type D HCN extends from the internal inguinal ring to the inguinal canal or just under the skin. 2
Diagnostic imaging is vital to diagnosing HCN, and many consider sonography a preliminary imaging technique for evaluating this pathology. 15 Equivocal sonograms can be assessed with computed tomography (CT) or magnetic resonance imaging (MRI). Therefore, some authors have advocated for the multimodality imaging approach to diagnose HCN.9,16
Case Report
A 37-year-old woman, G4 T3 P0 A1 L3 (gestation=4; term=3; preterm=0; Abortion=1; Living=3), presented to the emergency room (ER) at the local hospital. She was complaining of progressive pain in the right groin. Vital signs were reported to be normal. The complete blood count (CBC) and urinalysis results were also normal. Her beta human chorionic gonadotropin (HCG) was less than 5 IU, indicating the patient was not pregnant. A non-reducible painful bulge was visualized in the right lower quadrant (RLQ) by the on-call ER physician. An emergent sonogram was scheduled on the same day to determine whether there was an incarcerated hernia and appendicitis.
A dedicated sonogram of the RLQ was performed on this patient with both curvilinear and linear transducer connected to a Logiq E10 (GE, WI) ultrasound equipment system. The sonogram revealed an avascular, non-reducible, non-specific fluid collection in the right groin (See Figure 1). An echogenic soft tissue area was noted on the posterior aspect of this fluid collection, and it was reported as fat, within the inguinal canal (See Figure 2). The radiologist suggested adding an endovaginal sonogram to visualize the right adnexa with greater detail. Transvaginal sonography did not add any additional value to the cystic structure, seen on transabdominal imaging. The bilateral adnexa, ovaries, and the uterus were unremarkable.
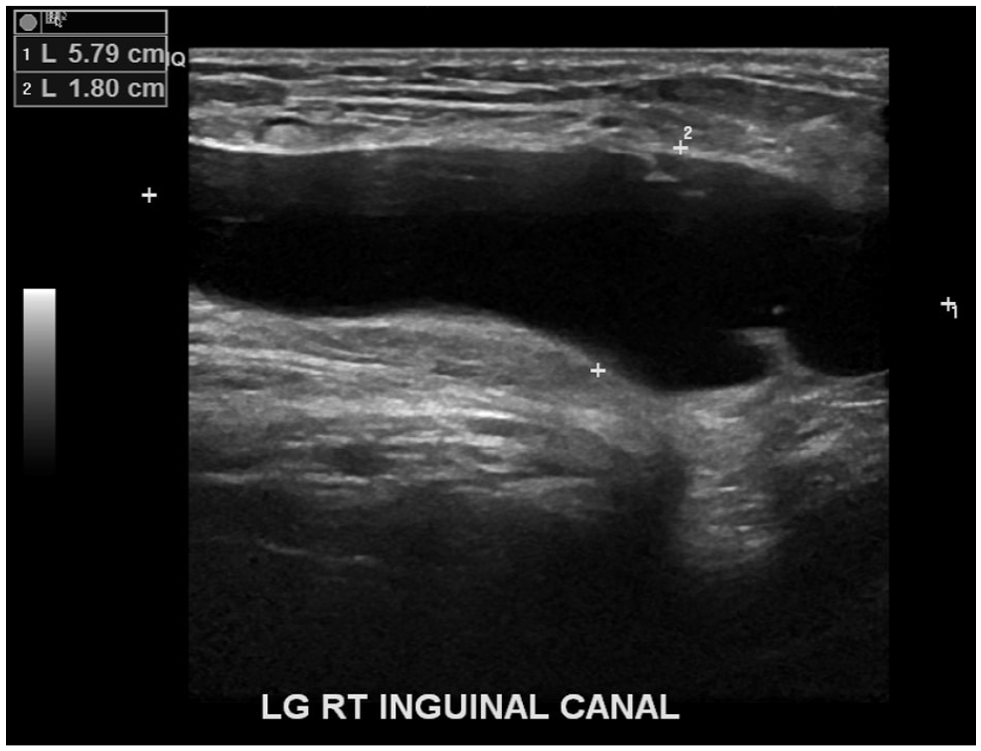
A sagittal sonographic view is provided of the 5.8 × 18 cm cystic structure, located in the right inguinal region.

A sagittal sonographic view of the echogenic structure adjacent to the cystic component is provided.
The radiologist recommended a non-contrast CT, to better delineate this cystic structure, seen on sonography.
A non-contrast CT revealed a bilobed elongated fluid collection with maximal dimension at 5 cm in the right inguinal canal, which raised the suspicion of an HCN (See Figures 3–5). A similar small HCN was also visualized in the left inguinal canal, which measured 3.0 cm in maximal dimension (See Figures 4 and 6). In this case, an MRI examination was not performed, as the CT was considered diagnostic. Based on the sonographic and CT images, it was most likely a bilateral HCN, which belonged to the traditional type I and Wang’s type B classification. Type I and Wang’s type B classification is based on the premise that there is no peritoneal communication superiorly or distally, and the HCN is within the inguinal canal.

An axial computed tomographic view is provided from a non-contrast computed tomogram of the pelvis. A transverse image showed the bilateral hydrocele of the Nuck canal. It is also important to note that the size of the hydrocele in the right groin was considered more significant than on the left.
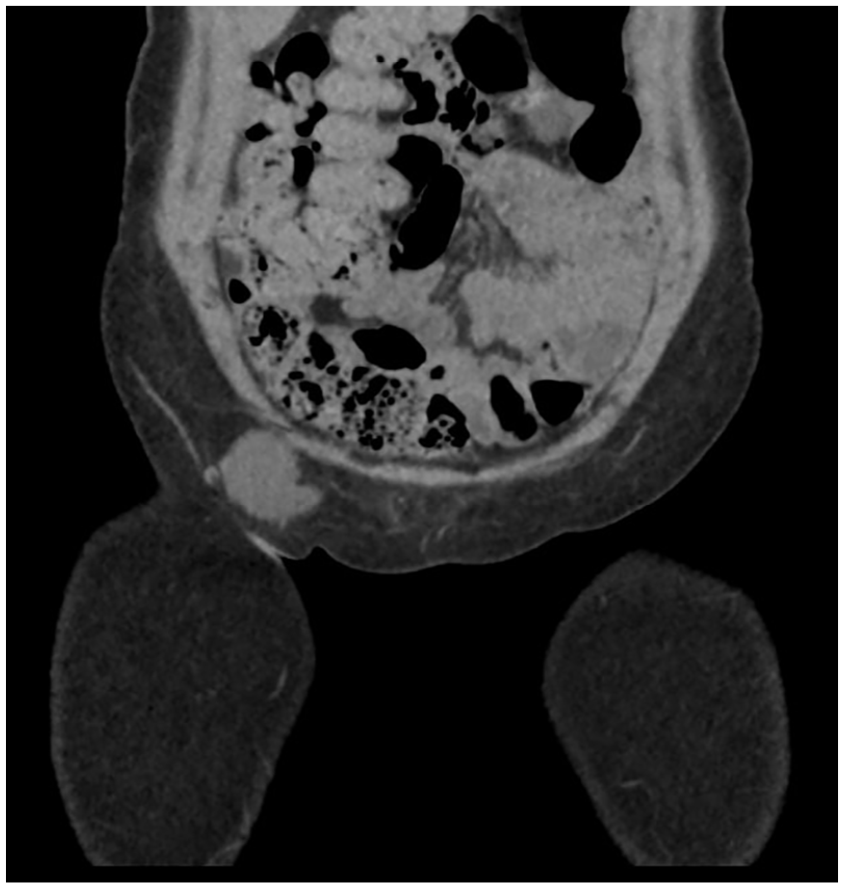
A computed tomographic coronal view demonstrates a bilobed cystic structure in the right groin area, which is suspected to be a canal of Nuck hydrocele.

A sagittal image from a non-contrast computed tomogram is provided. The image illustrated the hydrocele of the canal of Nuck, in the right groin (measured at 5 cm in maximal dimension).

The sagittal computed tomographic image illustrates the smaller hydrocele of the canal of Nuck in the left groin (3.1 cm in maximal dimension).
Treatment
A surgical consultation was recommended for elective surgery and complete excision of the HCN, rather than aspiration. Cyst aspiration may mitigate the symptoms associated with HCN but is not recommended, as a definitive treatment. The patient was scheduled for surgery in two weeks in another hospital. Due to technical reasons, the confirmatory histopathologic examination was unavailable for this patient.
It is important to note that a histopathologic examination is considered to be the definitive method to diagnose HCN. 4
Discussion
There are numerous case reports of HCN presenting unilaterally, but only a paucity of patient cases have been reported to present bilaterally, in the groin of adult females.17,18 Some studies have reported that inguinal swelling occurs 98.7%, in females with inguinal hernias, while only 0.76% account for an HCN. 10 Some have reported an HCN prevalence of 0.74% in female patients with inguinal swelling. 19 It is interesting to note that the prevalence or the incidence of HCN is reported in pediatric demographics only, and there seems to be a dearth of literature regarding the epidemiology of HCN, in adult females.
The current case study is one of the rarest case reports on HCN, in which the pathology appeared bilaterally. Clinically, inguinal canal pathologies manifest symptomatology in the lower pelvic quadrants or groins with varying severity in patients. Sonography, CT, or MRI is vital in diagnosing the HCN.20,21 Many authors believe sonography is the preferred or the initial diagnostic imaging technique for diagnosing HCN, based on high-resolution images, high-frequency transducer, dynamic mass evaluation, and lack of ionizing radiation.5,7,12,21,22 It is worth considering the proper sonographic technique, to diagnose a suspected HCN, should be initiated by evaluating the RLQ with the curvilinear transducer to better explain the relationship of the cyst with the adjacent anatomy. Any evidence of a fluid-like structure in the inguinal canal, in females, should be interrogated further with a high-resolution linear transducer to define the characteristics of the cyst. Sonographers and physicians must be familiar with the dynamics of their ultrasound equipment systems, to apply appropriate frequency, Doppler frequencies, sweep speed, focal zone, time gain compensation, sector width, and other relevant instrumentation, to yield diagnostic imaging of the HCN. Care should be taken not to increase the grayscale gain settings, which can inadvertently give the impression of complexity in the cyst.
If the sonographic examination is equivocal, MRI is the next best diagnostic imaging choice for delineating infection in the cyst. MRI is often considered the diagnostic gold standard for detecting HCN. 12 MRI provides a larger field of view, demonstrating a better anatomic relationship between the HCN and the intraperitoneal structures. Furthermore, MRI can detect subtle septations or complexities within the cyst, indicating infection or an inflammatory process.1,13,23 Administration of gadolinium may also help determine if the HCN is infected.12,24 The initial test of choice is controversial; while MRI offers several advantages, sonography and CT are more readily available.7,12,16 Some have suggested a multimodality imaging approach to better elucidate and classify HCN. 25 A multimodality imaging approach contributes unique insights, leading to a more accurate diagnosis and effective management. In the current case report, sonography was equivocal; hence, CT was ordered to delineate the pathology and anatomy for appropriate management. Furthermore, it is believed that the choice of imaging techniques may depend on the institutional expertise, the patient’s body habitus, and the availability of imaging equipment. 25
Some have suggested sonographic guided cyst aspiration for temporary relief of symptoms, but surgery is reported to be the definitive treatment, for this condition.12,21,26 The rationale is that while cyst aspiration can provide temporary relief, it does not address the underlying cause of the hydrocele. Surgical excision of the HCN and the inguinal canal repair can remove the hydrocele and prevent its recurrence, which provides a more permanent solution. 6 It is essential to underscore the complications of HCN, which would include infection, hemorrhage, or a large cyst with retroperitoneal extension. 27
RLQ tenderness in adult females carries numerous differential diagnoses. Some of the common diagnoses in the RLQ for a reproductive-aged female are ruptured ectopic, ruptured appendix, ovarian torsion, and bowel pathology (e.g., inflammatory bowel disease or other enteritis). Some of the less common diagnoses in the RLQ for adult females that may present as inguinolabial swelling are indirect or femoral hernia, lymphadenopathy, hematoma, ganglion cyst, cyst lymphangioma, neuroblastoma metastasis, abscess, Bartholin cyst, and neurofibroma.25,28,29
Conclusion
Many clinicians are unaware of pathologies within the canal of the Nuck pathologic spectrum. The HCN should be considered in cases of inguinolabial swelling among female patients. Surgical excision of the HCN is the definitive treatment. Sonography should be the initial diagnostic imaging choice for HCN owing to the lack of radiation, portability, dynamic visualization of the pathology, and the lack of preparation on the part of the patient for this test. The diagnostic multimodality imaging approach is beneficial in patients with equivocal sonograms. Imaging professionals, including sonographers, should be comfortable recognizing this pathology in their routine practice.
Footnotes
Ethics Approval
Ethics approval was obtained from the University of Manitoba with reference number:HS 26493 (H2024:177).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.