
Abstract
Current ultrasound systems have significantly improved spatial and temporal resolution secondary to increased transducer frequencies, increased bandwidth, and complex signal processing such as harmonics and compound scanning. The case presented describes the differential diagnoses of small, linear, mobile echogenic foci visualized by sonography in the left epididymal tail. Differentiation of moving parasites associated with filariasis versus mobile sperm may become more difficult as the resolution of ultrasound equipment continues to improve.
Introduction
As the resolution of ultrasound equipment improves, visualization of different entities, both normal and abnormal, has improved. When mobile echogenicities are seen within the epididymis, it may be due to lymphatic filariasis or to efferent duct obstruction secondary to postvasectomy changes.1–4 Although numerous cases of lymphatic filariasis have been published, it is uncommon in the United States; patients are unlikely to contract the disease unless they have been traveling to endemic regions.5,6 In the United States since vasectomy is a commonly performed procedure, postvasectomy changes to the epididymis would also be a common finding; Frates et al. 3 reported a 12.5% prevalence of mobile scrotal echogencities in postvasectomy patients. Although the sonographic presentation may be similar for these two entities, the patient’s treatment for each is very different. An accurate clinical patient history becomes an important part of distinguishing between these two processes.
Case Report
A 64-year-old man presented to his family medicine physician with complaints of left testicular pain. He stated that a few weeks prior he had been lifting and carrying his grandchild, following which he noted the pain in the left testicle. No abnormalities were detected during a physical examination. There was no history of vasectomy, scrotal surgery, or recent travel.
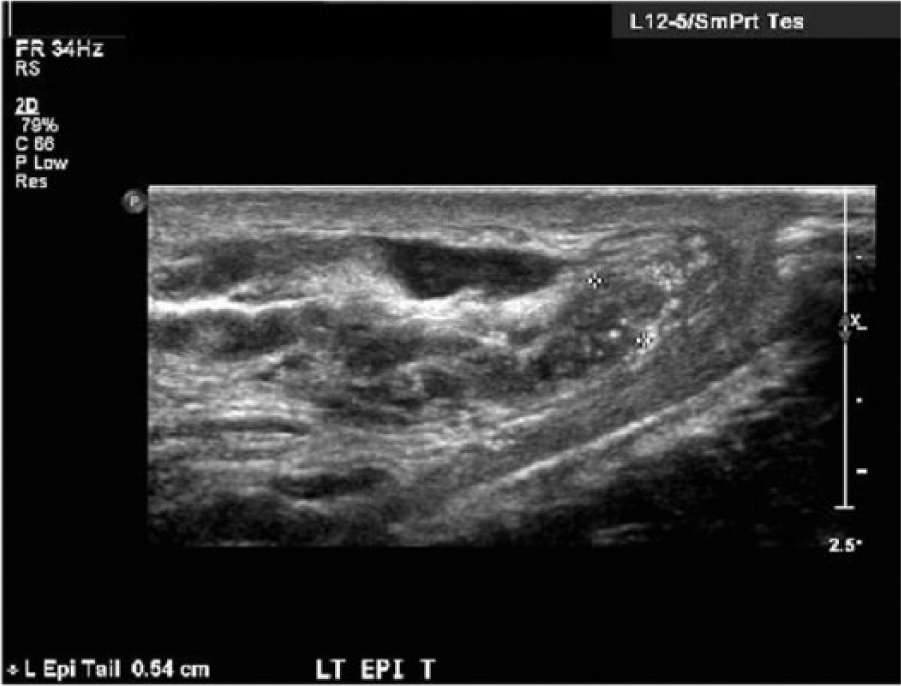
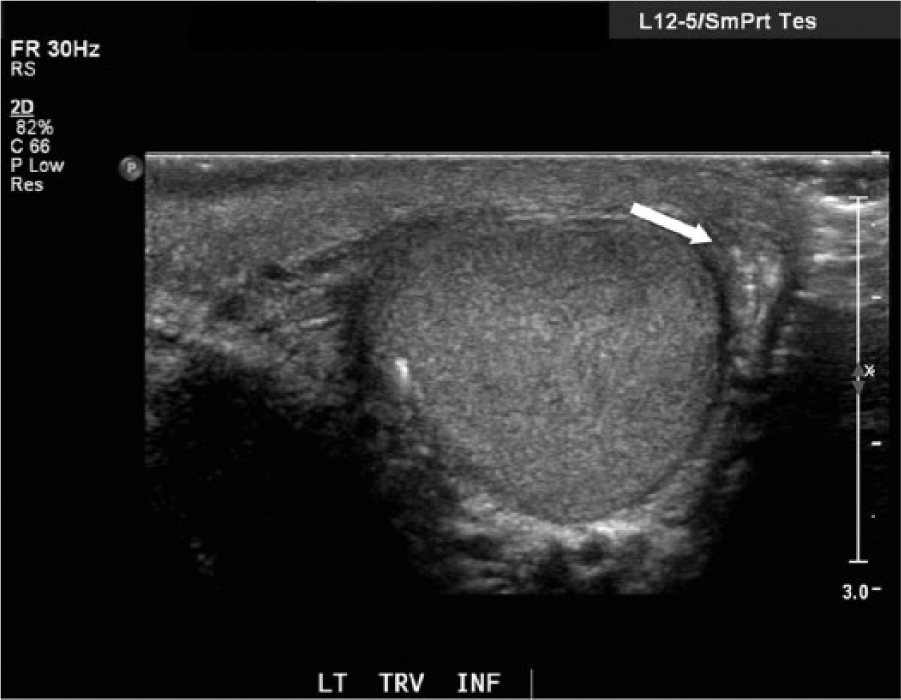
A testicular sonographic examination including color and spectral Doppler was performed using a Philips iU-22 ultrasound system (Philips Ultrasound, Bothel, Washington, USA) with a broadband L12-5 MHz linear array transducer. Punctate calcifications of uncertain clinical significance were visualized within the left testicle (Figure 1). Upon further evaluation, numerous mobile echogenicities were seen within the left epididymal tail (Figures 2 and 3, supplemental video in the online journal). When questioned about the patient’s travel history, he stated that he used to travel outside of the country for his job, although he had not done so since his retirement several years earlier. No more information was provided by the patient, and it was not possible to determine whether or not he had traveled to any endemic parasitic regions during his employment. Based on the sonographic images and clinical information provided, a diagnosis of slow flow or ductal obstruction secondary to scarring of the vas deferens (of unknown etiology), with a differential diagnosis of filariasis, was made. The patient returned a month later for evaluation of a hernia on the left side due to pain. It was confirmed that the patient had a left sided indirect inguinal hernia and a large cord lipoma. The patient later underwent a hernia repair during which the cord lipoma and the hernia sac were completely stripped away from the cord.
Transverse gray-scale image of the left testicle, showing punctate calcifications (cursors).
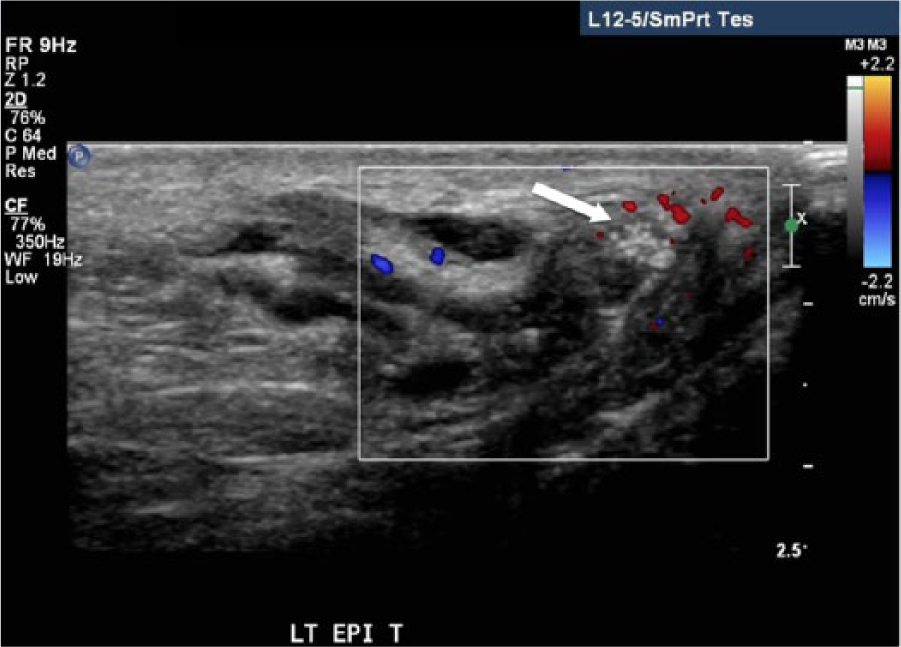
Color Doppler image of the left epididymal tail, showing small, mobile echogenicities (arrow).
Gray-scale image of the left epididymal tail, showing small, mobile echogenicities (arrow).
Discussion
Origin of Lymphatic Filariasis
Lymphatic filariasis is caused primarily by roundworms that are transferred to humans when bit by an infected mosquito. Lymphatic filariasis is a widespread disease, with 120 million people currently infected. 1 Approximately 65% of those infected live in South-East Asia and 30% in Africa. 1 This disease causes swelling of the limbs and male genitalia leading to social and physical disabilities. Wuchereria Bancrofti is a type of roundworm that is responsible for 90% of lymphatic filariasis.2,6 Larvae are contained within the intrascrotal lymphatic system where they develop into adult worms that can survive for 15 years or more. 5 Adult worms then produce microfilaria. Brugia malayi and B. timori are other parasitic roundworms that may act as causative agents using the same mode of transmission. 5 The twirling motion of the microfilaria is what is seen on sonography as mobile echogenic materials and is described as the “filariasis dance.”7,8
Clinical Features of Lymphatic Filariasis
During the acute stage of the infection, patients may present with fever, headache, backache, and nausea. Acute funiculitis, epididymitis, or orchitis may also be present. Chronic manifestations include lymphadenopathy, hydrocele, chyluria, and lymphedema. 5 It is assumed that as long as the worm remains viable, the lymphatic vessels remain patent. Death of the worm, however, leads to local necrosis of a granulomatous reaction around the parasite. Fibrosis occurs and lymphatic obstruction develops. 6 A sonographic sign of filariasis was first described as the “filarial dance” by Amaral and colleagues 7 in 1994, who believed that live adult filarial worms were creating the movement seen by sonography within the lymphatic system. Later, Shyamkumar and colleagues 8 suggested that the echogenic material represented microfilaria rather than adult worms. They based their report on documentation that adult worms were on average 1 to 4 cm in length and therefore larger than the 1 mm particles observed on sonography. Their hypothesis was supported by aspiration of dilated lymphatics that yielded microfilaria. It is important to note that filariasis, although common in endemic parasitic regions, is rare in the United States. Approximately 95% of people infected with filariasis are living in South-East Asia, India, and Africa. 1 Definitive diagnosis of lymphatic filariasis is possible using smear or serological tests. 8
Postvasectomy Epididymis Changes
Postvasectomy mobile echogenicities within the epididymal region may mimic the appearance of filariasis. During a vasectomy, a small section of the vas deferens is cut and then removed. Following the procedure, thickening of the epididymis may occur from epididymal tubular ectasia. The characteristic sonographic speckled appearance is thought to be due to the multiple interfaces between the epididymal tubule walls and fluid within. 9 Large clusters of spermatozoa, known as megasperm, trapped within the dilated tubules may be seen by sonography. The typical appearance is multiple echogenic foci moving in random swirling patterns. 3 Observation of megasperm within the epididymis has been a relatively recent finding and for the most part is due to improvements in sonographic equipment. Typically, megasperm are an incidental finding and pose no clinical concern.
Ramifications of Inguinal Hernia
An alternative hypothesis of tubular obstruction caused by extrinsic compression secondary to an inguinal hernia may provide a possible explanation for the visualization of mobile sperm within the epididymis. Inguinal hernias arise in the internal inguinal ring and extend superficially and inferomedially down the inguinal canal, anterior to the spermatic cord. Contents of the hernia may include bowel or fat. Indirect hernias in men may extend into the scrotum and may be a cause of ductal obstruction, swelling, and pain. Sonographic characteristics of inguinal hernia are fluid- or air-filled loops of bowel with peristalsis in the scrotal sac. 4
Several studies examining the sonographic appearance of mobile echogenicities within the scrotum could provide no explanation for men who have not had a history of filariasis or undergone a vasectomy. They suggest it may be due to scarring of vas deferens from a prior nonsurgical insult or infection. 3 It also has been noted that observation of mobile echogenic foci within the epididymis has coincided with improved sonographic imaging capabilities that have allowed for increased resolution of scrotal contents. 10 Recent ultrasound equipment improvements in image quality, including improved spatial resolution and increased transducer sensitivity, and signal processing improvements, such as harmonics and compound scanning, have led to more frequent detection of structures that are much smaller and deeper than was previously possible.
Sonography is an invaluable tool for the visualization of small structures. However, no data have been published as to how frequently sonography may be able to detect and distinguish between the pathologies considered in this case study, namely, megasperm versus lymphatic filariasis. With the improvements in ultrasound equipment and the ability to identify echogenicities within the epididymis, it is likely that these data will become available in the future. Following the evidence of mobile echogenicities within the epididymis, diagnostic medical sonography in conjunction with a complete medical history, clinical findings, and laboratory results are all essential elements in the implementation of a treatment plan specific to the patient.
Conclusion
Recent enhancements of ultrasound equipment could explain the observation of movement of echogenic foci within the epididymis that have been previously attributed to filarial infection or postvasectomy changes. It is important to recognize the similar appearance of these echogenicities and the different pathophysiologies that may cause them. In the absence of a proven filariasis infection or previous scrotal surgery, mobile echogenic foci within the epididymis may present as an isolated finding of no clinical significance or as a complication of an inguinal hernia.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.