
Abstract
A cyst of the canal of Nuck is a rare condition that occurs when the processus vaginalis fails to obliterate during embryologic development. When a nonreducible groin mass is seen in women and girls, a cyst of the canal of Nuck should be considered in the differential diagnosis. Sonography has shown to be accurate and reliable at diagnosing these cysts and should be the primary imaging modality used to image groin masses.
A cyst of the canal of Nuck (CCN) is a rare gynecologic condition in both women and girls, with few reports in the literature.1–3 It is the equivalent of the hydrocele that occurs in men and boys, and it occurs when the processus vaginalis, after migrating through the inguinal canal, does not fully obliterate during the first year of life. Serous fluid becomes entrapped in the inguinal canal, creating a hydrocele. It is a palpable, nonreducible groin mass that may present with pain or may be asymptomatic. Sonography has shown to be effective at diagnosing CCN, and sonographers and sonologists should consider this diagnosis any time a woman or girl presents with a nonreducible groin mass.4–7
Case Report
A middle-age woman presented with a sudden onset of a swollen, palpable mass in the right groin. The patient reported no pain and no previous surgeries or procedures in the area. A sonographic examination of the right groin region was done using a Philips iU22 system (Philips Ultrasound, Bothel, Washington) with an L9-3 linear array probe. The limited pelvic sonogram showed an anechoic, avascular, and cystic structure measuring 4.1 × 3.5 × 1.0 cm in the groin region (Figure 1A,B and Figure 2). The lesion was superficial to the femoral vessels and near the inguinal canal (Figures 3 and 4). A fat-containing inguinal hernia appeared when the Valsalva maneuver was performed in the standing position (Figures 5 and 6). In addition, a small portion of the cystic structure appeared to slide into the inguinal canal when imaging in the standing position (Figure 7). The contralateral side was assessed for comparison and had no abnormal findings. The lesion was diagnosed as a hydrocele of the canal of Nuck (cyst of the canal of Nuck) with a concomitant, fat-containing inguinal hernia.
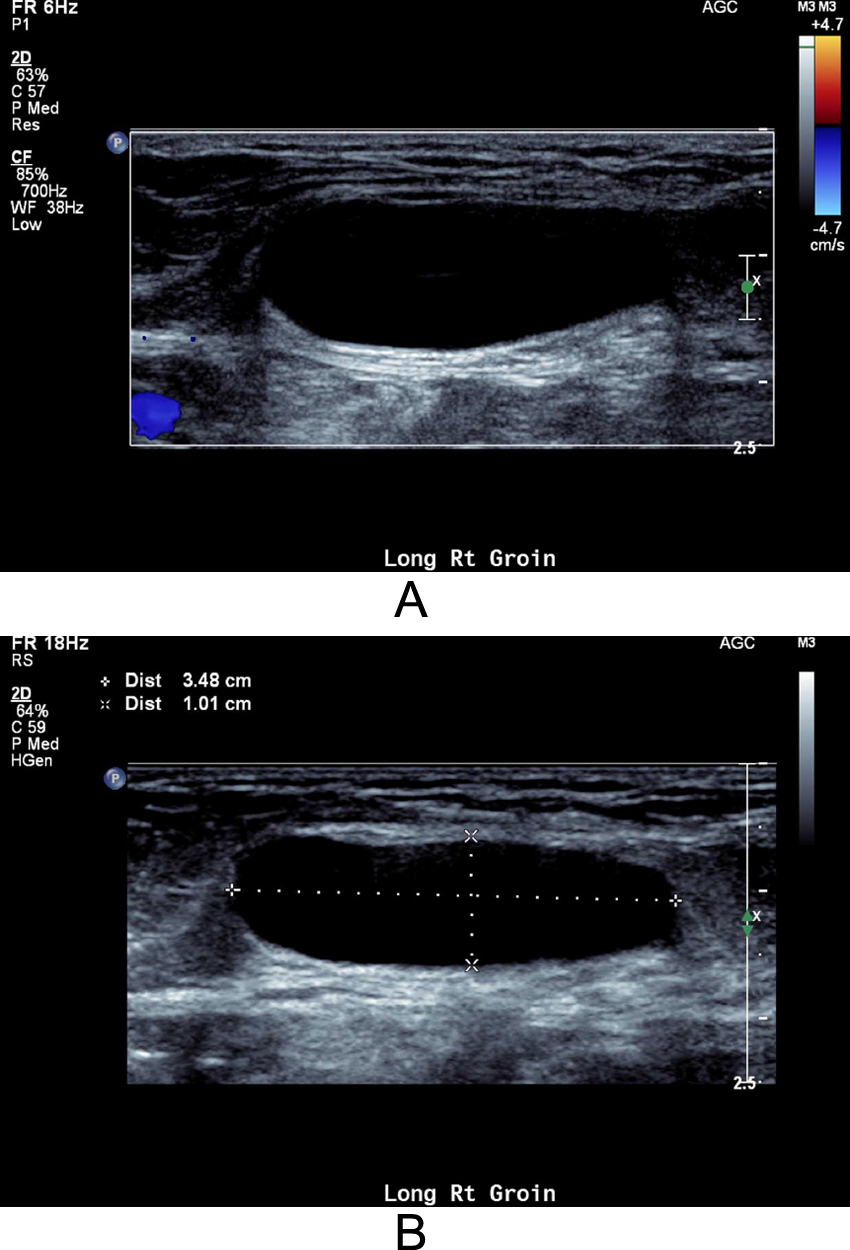
Longitudinal imaging of the right groin with the patient supine: (A) a color Doppler image showing an anechoic, avascular cystic structure and (B) a grayscale image of the structure with anteroposterior and transverse measurements shown.
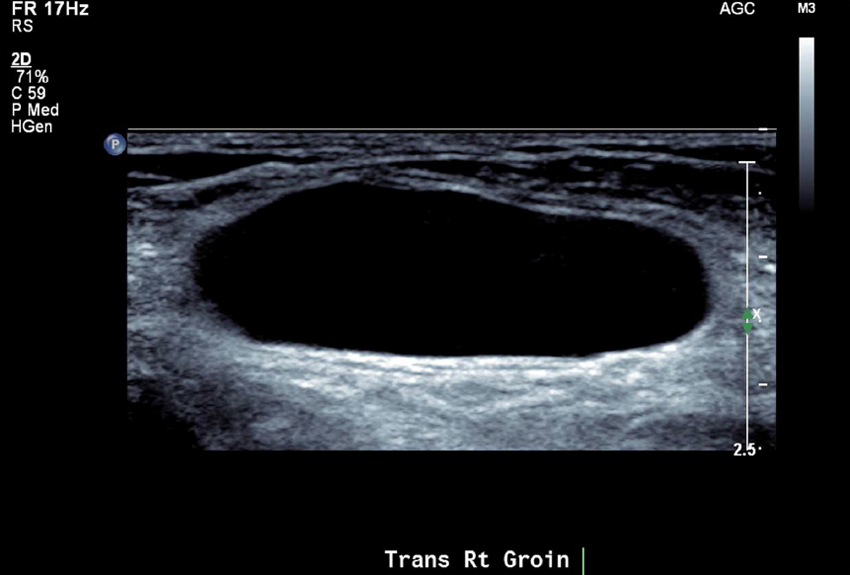
Transverse imaging of the right groin with the patient supine, showing the anechoic cystic structure.
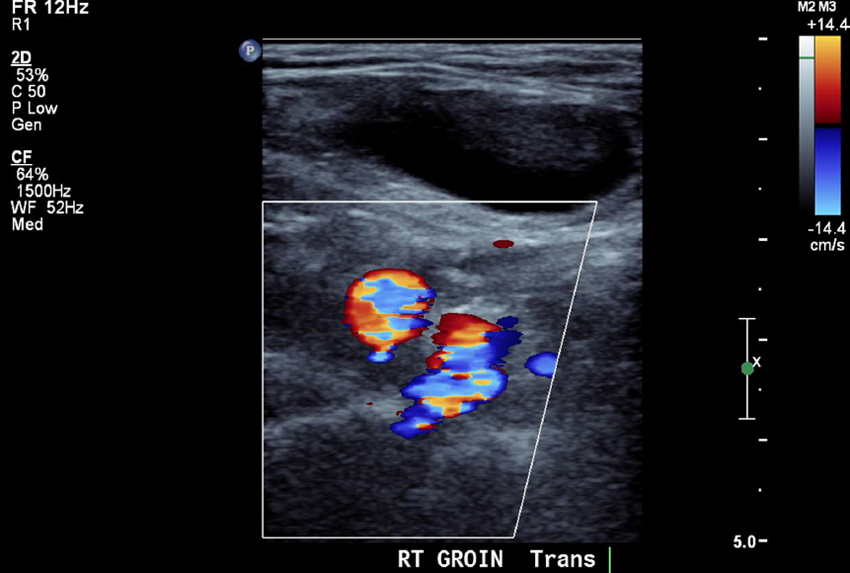
Transverse color Doppler image of the right groin with the patient supine, showing absence of flow in the cystic structure and no communication with the common femoral artery or vein.
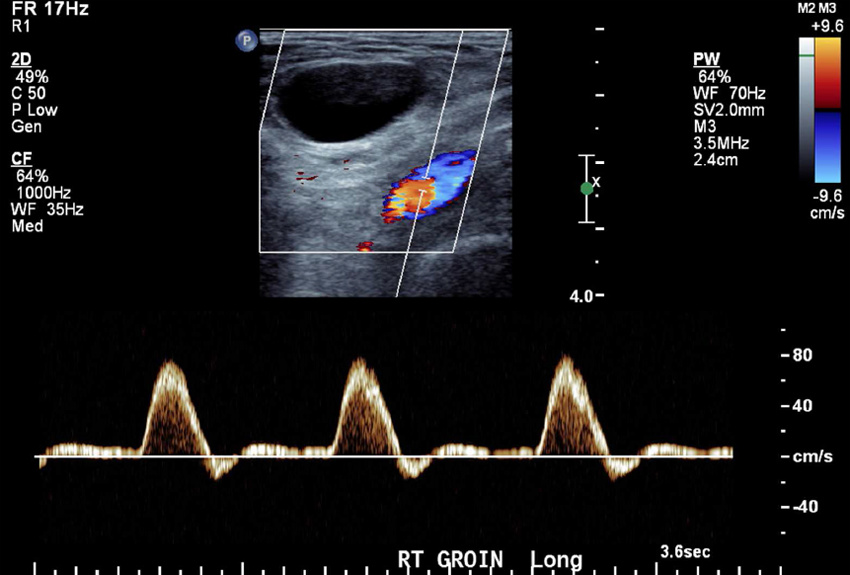
Spectral Doppler image taken in the right groin with the patient supine, showing normal arterial Doppler flow signals and no communication with the cystic structure.
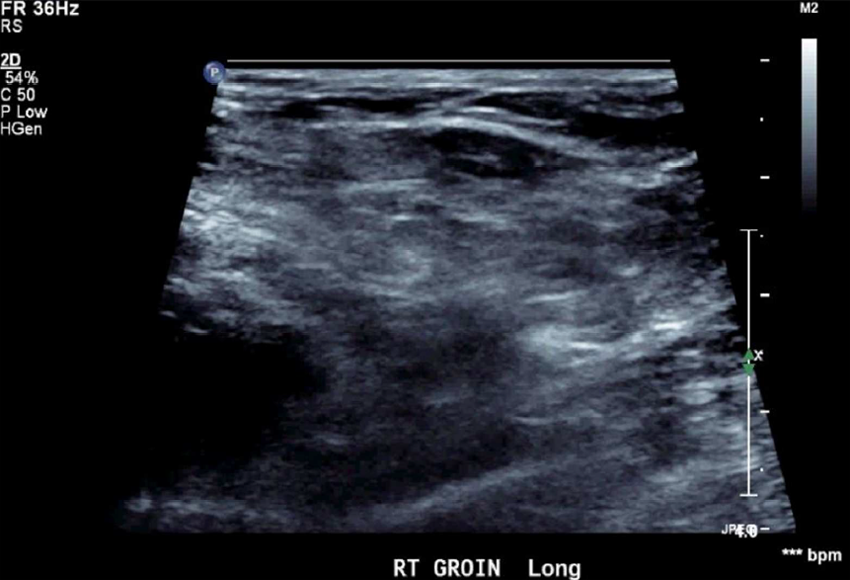
Longitudinal grayscale image of the right groin with the patient standing, without Valsalva.
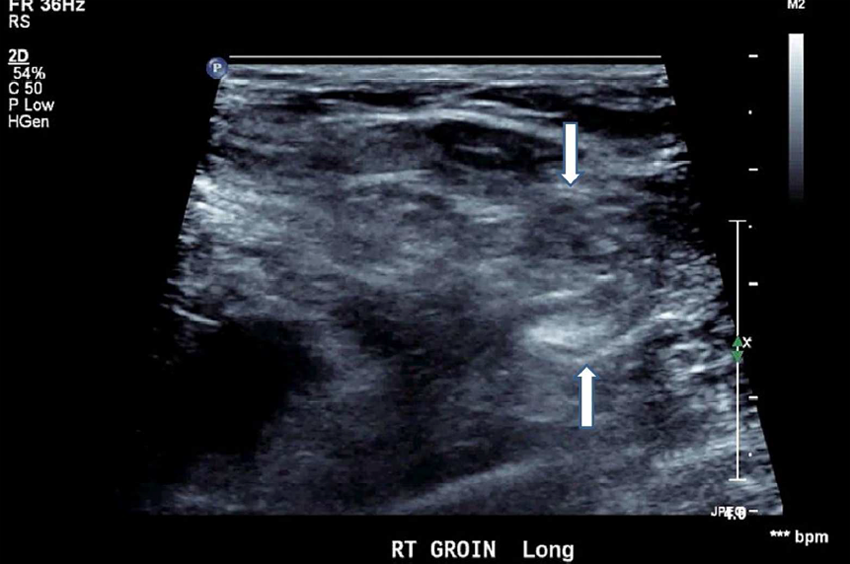
Longitudinal grayscale image of the right groin with the patient standing, with Valsalva. Arrows point to the inguinal hernia.
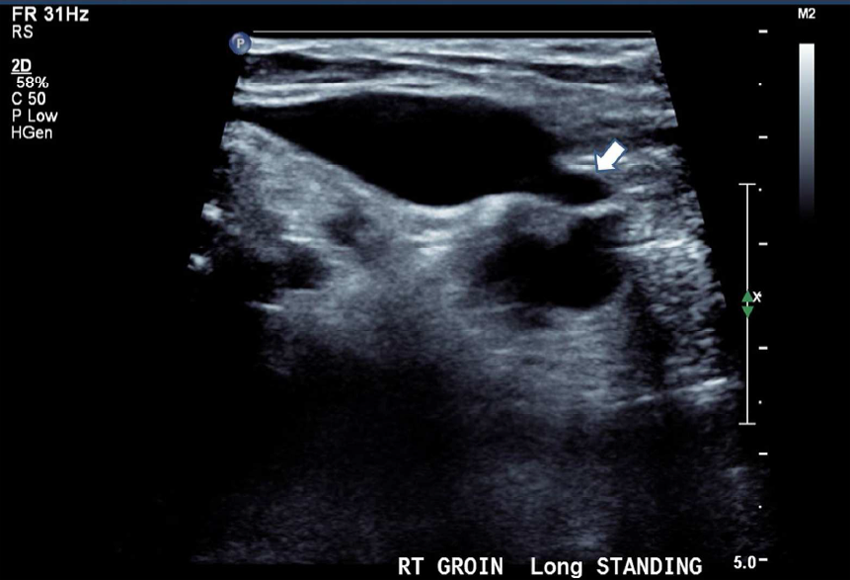
Longitudinal grayscale image of the right groin with the patient standing. Arrow points to where the cyst moved into the inguinal canal.
Discussion
The Inguinal Canal
The inguinal canal, located in the groin area, is a small narrow passage that lies above and parallel to the inguinal ligament. It begins at the level of the deep inguinal ring, which lies at a midpoint between the superior iliac spine and the pubic symphysis and lateral to the inferior epigastric vessels. It continues for approximately 4 cm before it ends at the superficial inguinal ring superior to the pubic tubercle. 1 The canal is formed by the processus vaginalis, an outpouching of peritoneal tissue that descends through several layers of the abdominal wall: the transverse fascia, the musculature of the internal oblique muscle, and the aponeurosis of the external oblique muscle. 1 The processus vaginalis forms the innermost layer of the canal, which provides the passageway for the gonads to descend from the false pelvis into the true pelvis.
In female embryonic development, the ovaries do not descend past the true pelvis. Instead, the round ligament of the uterus, along with the processus vaginalis, passes through the deep inguinal ring, creating the canal of Nuck. By the time the processus vaginalis migrates to the level of the superficial inguinal ring and connects to the labia majora, it consists of only a few strands of fibrous tissue. 2 The canal of Nuck should fully obliterate by the end of the first year of life. 2
Pathophysiology
A CCN in women is equivalent to a hydrocele of the scrotum in men. It occurs only in women and is rarely reported in the literature.3,4 It is typically the result of the failure of the canal to close within the first year of life. Fluid accumulates within the inguinal canal, creating a cyst-like lesion.5,6 The location of the cystic lesion within the canal will depend on the level at which the canal did not obliterate. If the upper part was not obliterated, then the fluid collection may communicate with the peritoneal cavity and is called a congenital hydrocele. 5 An infantile hydrocele occurs when the canal is obliterated at the deep inguinal ring but is open at the superficial inguinal ring. 5 In this situation, the hydrocele may extend from the labia superiorly into the canal. If the canal is obliterated at the level of both the superficial and deep inguinal rings, fluid may be trapped in between both ends of the canal, creating a CCN. 5
A CCN may present as a painless swelling in the groin region that can extend into the labia majora. 3 In some cases, it may present with a deep or aching groin pain, or it may be asymptomatic and an incidental finding on physical examination.3,6,7 The mass can be fluctuating and is not reducible. 8 In some cases, the cyst can be strangulated or infected, in which case it may present as an abscess. 4
Sonography of the Canal of Nuck
Although there is no defined, standardized scanning protocol for the groin region, Grant et al 7 described an imaging protocol to detect groin hernias. Because a CCN and hernias typically appear in the same location, the protocol should be able to detect cystic lesions as well as hernias. The examination demands high resolution in the near field; therefore, a high-frequency linear transducer is required. The transducer should be placed directly over or slightly inferior to the inguinal ligament, which is typically identified as an echogenic fibrous structure. 7 The transducer is moved from the labia majora laterally toward the inferior epigastric artery. The transducer should be rotated 90 degrees and moved medially to interrogate the entire inguinal ligament. 7 Finally, the area over the femoral canal, which is located medial to the femoral vein and proximal to the saphenofemoral junction, should be evaluated. 7 Throughout the examination, the Valsalva maneuver should be performed. If a hernia is suspected but not demonstrated in the supine position or with a Valsalva maneuver, the sonographer can repeat the protocol with the patient standing.
Sonographically, a CCN appears as a cystic lesion with smooth borders. It is most typically described as sausage shaped but also has been documented as a comma-shaped lesion with the tail projected toward the inguinal canal.3,5,6 The cysts are small, averaging 3 to 5 cm in length and typically less than 0.5 cm in diameter, although larger cysts have been reported.3,5 Other sonographic descriptions include a cyst with septations, a cyst within a cyst, and multicystic.9,10 The lesion should have through transmission with posterior acoustic enhancement and will not demonstrate vascularity with color or spectral Doppler.4,11 When transducer pressure is applied, the Valsalva maneuver is performed, or the standing position is used, the cyst may move but does not appear to reduce. 8
Magnetic resonance imaging (MRI) also can diagnose a CCN, but there is a general lack of reported findings by MRI.4,5,8,11 Although there are no validity statistics for the sonographic diagnosis of CCN, the ability to accurately demonstrate the pathology has been well described in the case report literature.3–6,12–14 Sonography is cost-effective compared with MRI and is easily performed in the groin region; therefore, it should be the first imaging modality used to image groin masses.
Inguinal Hernia
Inguinal hernias are the most common differential diagnosis, but they also may coexist with a CCN in up to one-third of cases, which creates difficulty in accurately diagnosing the condition3,8 Groin hernias are classified as direct, indirect, and femoral. A direct hernia is located medial to the inferior epigastric artery and occurs when the abdominal wall muscles are weak, allowing the contents to protrude through the wall of the inguinal canal.7,15 An indirect hernia occurs along the inguinal canal, and the contents pass through the inguinal canal.7,15 A femoral hernia does not involve the inguinal canal and instead is located medial to the femoral vein. 7 Fat and/or bowel, presenting as solid, hyperechoic structures in any of these locations, indicate a hernia is present.4,7
Unless a groin hernia is incarcerated, it should be reducible with transducer pressure, helping to differentiate it from a CCN. 15 The Valsalva maneuver can reveal occult hernias by demonstrating movement of the omentum or bowel into and out of the inguinal canal, whereas a cyst will not demonstrate such movement.4,7 Other differential diagnoses include Bartholin’s cysts, lipomas, femoral aneurysms, and lymph nodes.3,6 The CCN should not demonstrate vascularity, thus differentiating it from lymph nodes, aneurysms, and malignant masses. Bartholin’s cysts have a characteristic location at the junction of the middle/lower labia majora, which should eliminate confusion with a CCN. 3
Treatment
Surgical removal is the most curative treatment, and the subsequent pathologic examination is the gold standard for the diagnosis of a CCN.6,12 Because CCNs are highly associated with inguinal hernias, it is recommended that the deep and superficial inguinal rings be inspected at the same time and repaired if necessary. The neck of the processus vaginalis should be ligated to prevent reoccurrence. 4 Cyst aspiration is rarely curative and is associated with a high rate of recurrence. 3
Conclusion
A CCN should be considered any time a nonreducible groin mass is found in women and girls. It can be confused with inguinal hernias but also can occur in conjunction with an inguinal hernia. Because sonography is cost-effective, is efficient, and can reliably differentiate an inguinal hernia from a CCN, it should be considered the first line of imaging for nonreducible groin masses in women and girls.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.