
Abstract
Objective:
This study aimed to investigate the efficacy of sonography in reducing morbidity and mortality among patients with shock, particularly in the emergency department (ED). By employing the “Rapid Ultrasound for Shock and Hypotension” (RUSH) protocol with ED patients, the aim was to assess its contribution to patient outcomes.
Materials and Methods:
This prospective, cross-sectional study spanned 2 years and was conducted in a university-based emergency department. Overall, 100 adult patients with blood pressure ≤90/60 mmHg and shock index >1 were enrolled. The RUSH protocol was followed for each patient.
Results:
The study comprised 35 females and 65 males, with a mean age of 57.12 ± 17.1 years. The RUSH assessment indicated that 50 patients had fluid volume indices below 1.5 cm, predominantly presenting with hypovolemic shock (55%). Extended Focused Assessment with Sonography in Trauma (E-FAST) examination revealed free abdominal fluid in 18% of the patients. Cardiogenic shock, including arrhythmia and heart failure, was diagnosed in 9 patients each. Nine patients experienced obstructive shock. Initial RUSH protocol diagnoses included hypovolemic shock (n = 55), distributional shock (n = 19), cardiogenic shock (n = 8), obstructive shock (n = 6), and complex shock (n = 12).
Conclusion:
The RUSH protocol has emerged as an early, systematic, and practical method for assessing patients with hypotension and shock in the ED. It may also offer the potential to enhance patient management and outcomes.
Shock is an acute clinical syndrome that primarily results from inadequate delivery of oxygen and nutrients to tissues and organs, leading to cellular dysfunction. According to a systematic review, approximately 2% of patients presenting to the emergency department (ED) have hypotension, with systolic blood pressure (SBP)
Ultrasonography (U/S) is a safe and rapid imaging technique that can be performed at the patient’s bedside.2,3 It is an imaging method widely used in emergency medicine in recent years and has become an essential diagnostic tool in many EDs worldwide; it may facilitate early diagnosis and treatment of patients with signs of hypotension and shock who are admitted to the ED by narrowing down the differential diagnosis. Some underlying causes of shock, such as pericardial tamponade, abdominal aortic aneurysm (AAA), hypovolemia, and free fluid in body cavities resulting from trauma and cardiogenic shock, can be rapidly diagnosed via U/S.
Many bedside U/S protocols have been developed to evaluate patients requiring critical care in the ED. The most widely known is the “Rapid Ultrasound for Shock and Hypotension” (RUSH) protocol. The RUSH protocol is used in patients with hypotension and shock to help identify the underlying causes and make a rapid diagnosis. Extended Assessment with Sonography for Trauma (E-FAST) was performed following the RUSH protocol. This method assesses the presence of free fluid in the abdomen and thoracic trauma with the help of U/S. This study aimed to identify the underlying causes and make a differential diagnosis of shock in hypotensive patients presenting to the ED with the help of bedside U/S and RUSH protocol. Furthermore, this study determined the contribution of U/S to the diagnosis and treatment of critically ill patients.
Materials and Methods
This prospective, cross-sectional study included 100 non-pregnant adult patients admitted to the ED of a university hospital over a 2-year period. Patients with a shock index
After the initial emergency examination in the ED, the underlying causes of hypotension and shock were evaluated, on average, in less than 5 minutes. Within the first 10 minutes of admission, the RUSH protocol of bedside U/S was performed. Sonographic evaluation was performed using an M-turbo ultrasound system (FujiFilm Sonosite, Bothell, Washington State) and three transducers (sector, linear, and convex). The effects of the device and protocol on the patient’s clinical course were also studied. An accredited senior emergency medicine resident with basic and advanced U/S training implemented the RUSH protocol for all patients.
Implementing the Bedside U/S and RUSH Protocol
The RUSH protocol comprises the following three steps:
Step 1: Pump.
Step 2: Tank (Volume).
Step 3: Pipes (Veins).
Step 1: Evaluation of the heart
Cardiac imaging was performed, with the patient in the supine position, using a sector transducer to view the heart in the parasternal long and short axes, as well as the subxiphoid and apical four-chamber views.
Initially, any anechoic appearance around the heart, indicative of pericardial fluid, was assessed. If pericardial fluid was identified, further evaluation was conducted for signs of diastolic notching, as the presence of this fluid could lead to tamponade by impairing the right ventricular filling, potentially resulting in shock. Patients diagnosed with cardiac tamponade were subsequently classified as having obstructive shock (See Figure 1).
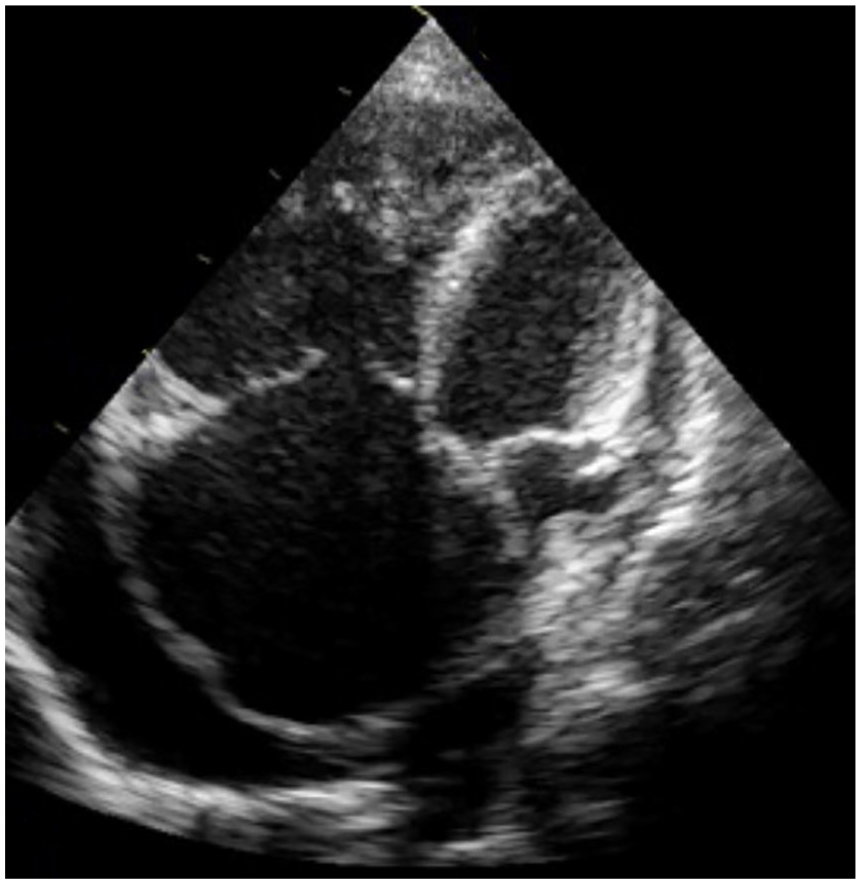
Sonographic apical long axis view of an emergency room patient who exhibited pericardial tamponade.
Cardiac function was assessed by examining left ventricular contractility, which was classified based on the ejection fraction (EF) values as follows: >70%, hyperdynamic; between 50% and 70%, normal; between 40% and 50% mildly hypokinetic; <40%, critically hypokinetic.
In cases where the heart was hyperkinetic, severe anemia or hypovolemic conditions resulting from fluid loss were suspected.
In addition, the presence of fever, with a focus on infection in such scenarios, was evaluated as indicative of the early stages of septic shock. In contrast, a critically hypokinetic heart prompted considerations of cardiogenic shock, stemming from severe heart failure, or a late stage of septic shock, particularly if accompanied by fever with a focus on infection.
Patients who exhibited an increase in the right ventricular size were assessed for pulmonary embolism, which can cause obstruction of the right ventricle. Accompanying findings including a dilated and overloaded inferior vena cava (IVC), with a diameter exceeding 2.5 cm that did not collapse during respiration, and deep vein thrombosis (DVT) detected in a Venous Duplex examination of the lower extremities were considered indicative of obstructive shock.
Step 2: Evaluation of blood volume status
To evaluate the blood volume status of patients, the process began by measuring the diameter of the IVC from the subcostal window using the long axis. Measurements were performed distal to the hepatic vein (i.e., approximately 1-3 cm from the entrance of the IVC into the right atrium). Subsequently, the estimated central venous pressure (CVP) was assessed based on the extent of IVC collapse during respiration. Patients with a low IVC diameter were particularly considered for hypovolemic shock. Those with an IVC measurement less than 1.5 cm were categorized as hypovolemic, whereas those with a measurement exceeding 2.5 cm were classified as hypervolemic (See Figure 2).
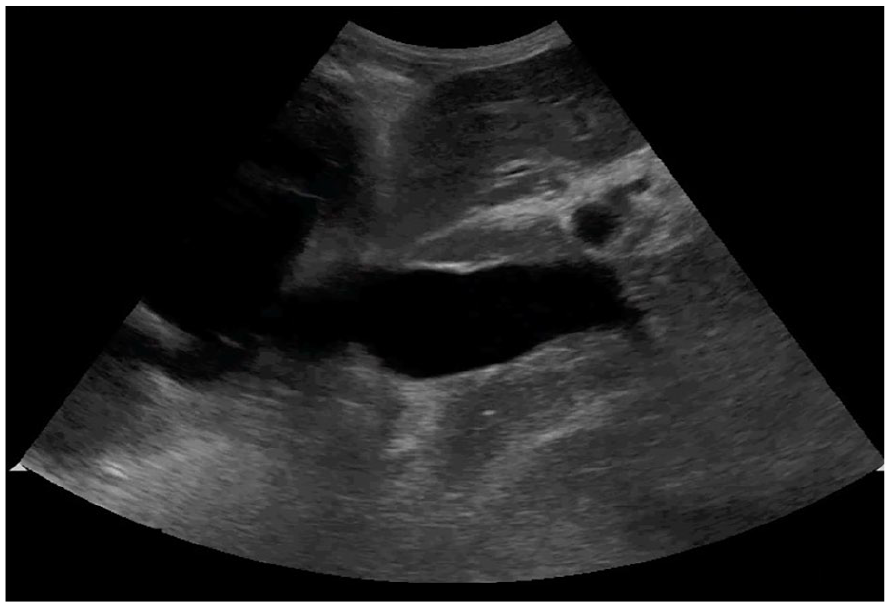
Midline sagittal view of an emergency room patient’s dilated inferior vena cava.
During the E-FAST examination, both the abdominal and thoracic cavities were examined for free fluid to identify the potential sources of hypotension and blood volume loss. Using a convex transducer, specific regions such as the subxiphoid area, Morrison’s pouch (hepatorenal space between the liver and right kidney), and splenorenal (lineorenal) space between the spleen and left kidney were examined for signs of free fluid (hemoperitoneum), particularly in the pelvic area. Additionally, the presence of pleural effusion (hemothorax) was assessed by pulmonary imaging using a sector transducer.
Patients with free fluid in the thoracic cavity were initially diagnosed with hypovolemic shock. Furthermore, within the framework of the E-FAST examination, the lungs were also evaluated for pneumothorax, a potentially concealed condition that can disrupt the volume status and lead to obstructive shock.
Step 3: (Pipes-veins)
During vascular examination, the presence of an aortic aneurysm or dissection, which could potentially cause shock, was assessed. This evaluation involved the examination of the aorta through the suprasternal, parasternal, epigastric, and supraumbilical areas, using a sector transducer. Patients with an aneurysm or dissection were classified as having hypovolemic shock owing to the risk of rapid blood loss.
Further evaluation included scanning for deep vein thrombosis (DVT) using a linear transducer to inspect the femoral and popliteal veins. Patients with DVT, along with enlarged right cardiac structures and a high IVC index, were considered to have obstructive shock, with pulmonary embolism primarily suspected as an underlying cause.
Patients with no definitive U/S findings to explain hypotension were assessed for distributive shock. Patients with an evident focus on infection were within the framework of septic shock. In addition, patients with a history of drug intoxication, snakebite, scorpion bite, or anaphylaxis were evaluated as having distributive shock.
In scenarios where patients presented with hypotension and shock, the underlying causes were thoroughly investigated using U/S as part of a comprehensive examination, adhering to the RUSH protocol performed in three steps (See Table 1). Patients with indications of multiple causative factors for shock were categorized as having complex shock, reflecting the multifactorial nature of their condition.
Example of Shock Assessment Following the RUSH Protocol. 4

RUSH, Rapid Ultrasound for Shock and Hypotension; RV, right ventricular; IVC, inferior vena cava; DVT, inferior vena cava.
Statistical Analysis
The IBM SPSS Statistics 29.0.1.0 package program was used to analyze the study data. Continuous variables were evaluated using the Shapiro-Wilk test, histogram, and q-q plots to determine whether they conformed to a normal distribution. The independent sample t-test or one-way analysis of variance was used to analyze normally distributed continuous variables, and the Mann-Whitney U or Kruskal-Wallis test was used to analyze abnormally distributed continuous variables. The chi-square test was used to analyze categorical variables. Results are reported as mean ± standard deviation, median (min-max), frequency (n), and percentages (%). During evaluation, cases where the p-value was
Results
In all, 100 patients, 35 females and 65 males, who presented to the ED with hypotensive complaints (weakness, dizziness, oral intake disorder, chest pain, trauma, etc.) with a blood pressure of 90/60 mmHg or lower were included in the study (average age, 57.12 years).
The most common complaints were oral or rectal bleeding (17%), impaired consciousness (13%), dyspnea (13%), oral intake disorder (12%), and trauma (8%).
Patients with hypotension were hospitalized in the emergency critical care unit. Their vital signs (pulse rate, fever, and blood pressure) were recorded (See Table 2).
Reference for Patient Vital Signs and Subsequent Findings for Evaluating the Study Patient’s Examination Results.

The patients were evaluated via U/S based on the RUSH protocol, while the emergent evaluation, emergency treatment procedures, or emergent intervention procedures were completed by another emergency (ER) physician.
One patient’s abdomen could not be visualized by U/S because of gas distension in the abdomen and obesity. Initial examination revealed a heart rate of 35 beats per minute. The patient was diagnosed with cardiogenic shock because electrocardiogram (ECG) showed a complete atrioventricular (AV) block.
RUSH
PUMP: Evaluation of the pumping function of the heart and its results
In this step, wherein the pumping function of the heart was evaluated, free fluid was observed around the heart in seven patients. Pericardial tamponade caused by advanced effusion accompanied by diastolic notching was observed in four of these patients.
Ejection fraction (EF) calculations revealed that seven patients with EF less than 40% were considered to be critically hypokinetic. Furthermore, 16 patients, whose EF values were measured between 40% and 50%, were considered mildly hypokinetic, and 73 patients had EF values within the normal range (50%-70%). The remaining four patients had EF values greater than 70%, indicating that these patients had extremely hyperkinetic cardiac functions.
The right ventricle diameter in five patients was enlarged, and ten patients had decreased right ventricle diameter, three of them had pericardial effusion. The right ventricle diameter of the remaining 85 patients was considered normal (See Table 3).
Evaluation of the Study Patients’ Cardiac Pumping Functions.

RUSH: Rapid Ultrasound in Shock and Hypotension.
TANK: Evaluation of volume status and the results
The IVC diameter of 50 patients was <1.5 cm, and the estimated CVP values were found between 0 and 5 cmH2O. Furthermore, the IVC diameter of 20 patients was between 1.5 and 2.5 cm. The IVC was evaluated as collapsing by more than 50% in these patients (estimated CVP values 5-10 cmH2O), and a volume deficit was detected in all these 70 patients.
In 24 patients, the IVC measurement was between 1.5 and 2.5 cm and the IVC was collapsed by less than 50% (estimated CVP values of 10-15 cmH2O). In five patients, IVC diameters were >2.5 cm, and it was noted that the IVC did not collapse (Estimated CVP values > 20 cmH2O). IVC diameters could not be measured in one obese patient.
In the FAST examination, free fluid was visualized within the abdominal or thoracic cavities in 18 patients. Only 12 patients with free fluid within the abdominal or thoracic cavity experienced severe volume depletion. In one patient with obesity, FAST could not be performed because of intense gas.
After observing that three of our patients did not have pleural slipping movement, we examined these patients in M-mode and found stratosphere findings that were evaluated as pneumothorax. Two of these patients had trauma and the other had iatrogenic pneumothorax with dyspnea after biopsy (See Table 4).
Study Patients Results Based on the RUSH Second Step of Volume Evaluation.

IVC, Inferior vena cava; FAST, Focused Assessment with Sonography in Trauma.
PIPES: Vascular examination and its results
In this step, an aortic evaluation was performed first. Of the four patients with abdominal and back pain, two had dissection of the abdominal aorta and one had an abdominal aortic aneurysm. Optimal evaluation of the fourth patient, who was obese, could not be performed because of high intestinal gas content. Dissections were visualized via tomography. The DVT was detected in three patients during venous system evaluation. Two of these had enlarged right ventricles, and a pulmonary embolism was present on dynamic computed tomography (CT) imaging (See Table 5).
Study Patient’s Results Based on Their Vascular Examinations.
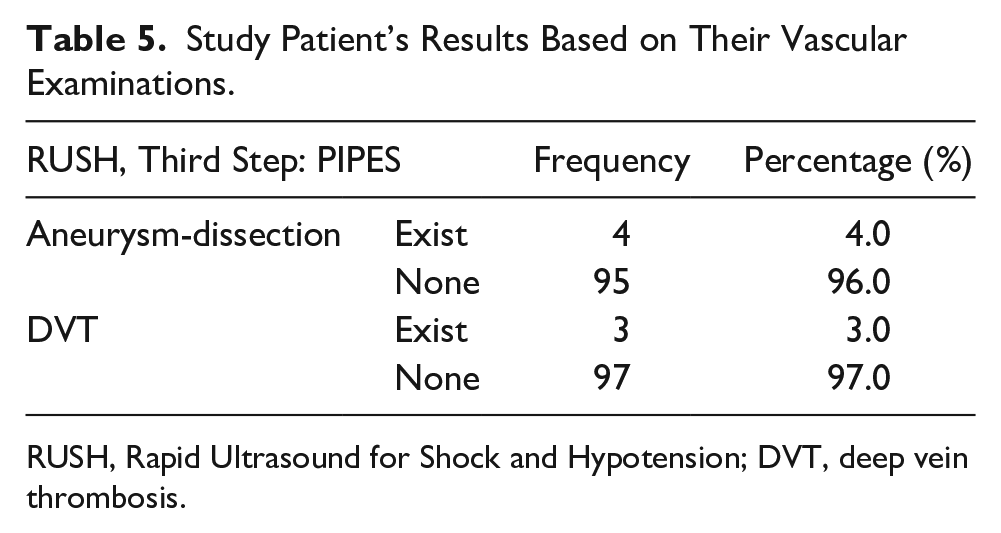
RUSH, Rapid Ultrasound for Shock and Hypotension; DVT, deep vein thrombosis.
During the pre-diagnosis of shock, 55 hypovolemic shocks, 19 distribution shocks, 8 cardiogenic shocks, 6 obstructive shocks, and 12 shock types were evaluated as complex shocks among 100 patients. All prediagnostic evaluations were confirmed by relevant consultant physicians.
After the evaluation made in the first 10 minutes, 4 of our patients, who were quickly diagnosed, showed a poor clinical course, and died in the ED, whereas 56 of the remaining 96 patients were discharged from the intensive care unit, and 16 were discharged after treatment in the ED.
Discussion
Time is a vital factor during examinations for the early diagnosis and treatment of patients with shock admitted to the ED. The U/S, which is a safe and fast imaging technique that can be used at patient bedside, can help to diagnose, and treat patients early by narrowing down the differential diagnosis of patients who visit the ED with hypotension and shock findings.
In this study, 100 patients (65 male and 35 female), who were aged
Sonographic evaluation (i.e., RUSH), as defined by Perera et al., 4 requires an examination protocol that focuses on finding the cause of shock in hypotension and shock patients and consists of three steps: pump (pump), tank (volume), and pipes (veins). This is a method for quick bedside U/S evaluation, wherein the pumping power of the heart, body volume status, and vessels are examined. The main role of this method is to elucidate the most probable diagnosis by narrowing the definitive exclusion range of other life-threatening conditions among all potential causes in patients with signs of hypotension and shock.
In the RUSH study conducted by Ghane et al. with 77 hypotensive patients (38 males and 29 females) RUSH was applied, on average, within the first 10 to 25 minutes of the patients’ admission. 5 In addition, U/S imaging was performed by a radiologist who was a resident to the ER physician. In our study, U/S evaluations were performed by ER physicians who received basic and advanced U/S training. All evaluations were completed by the same physician within the first 10 minutes and the results were recorded.
Eight patients were included in the study with signs of circulatory disorder in the ED with a BP of 90/60 (mean arterial pressure below 65 mmHg) but did not have any finding that could cause hypotension as per the RUSH protocol. These patients were evaluated for distributional shock (anaphylaxis in two patients, drug poisoning in three patients, snakebite in one patient, scorpion sting in one patient, and hypoalbuminemia caused by cirrhosis in one patient).
Nine patients were included in this study. The U/S evaluation could not be optimally performed in one patient because of the patient being overweight and insufficient pathological findings on U/S.
In the present study, all diagnoses were confirmed by consultant physicians by comparing the initial diagnoses we provided to the patients via the RUSH protocol, other imaging methods (e.g., CT), and definitive diagnoses made by the relevant ER physician or other consultant physicians.
FAST evaluation could not be performed in obese patients because of the presence of intense gas. The usefulness of abdominal sonographic evaluation is limited in obese patients because of high abdominal depth, intestinal gases, and abdominal fat. In addition, because the experience of the physician performing the U/S can change the value of the diagnosic result, physician-related limitations can be present. The inability to visualize retroperitoneal free fluids by sonography is a U/S-based limitation of FAST evaluation.
If a patient in shock shows insufficient filling and an IVC
When other parameters were evaluated, tamponade was detected with effusion close to 3 cm around the heart, whereas aortic dissection starting from the patient’s aortic root was observed in the U/S examination at the next stage. The detection of aortic dissection by U/S in a patient with hypovolemic shock caused by fluid loss in the initial diagnosis can be considered a separate example of U/S evaluation being a diagnostic tool independent of the clinical status of the disease.
Rapid distinguishing of the etiology of shock allows for quick administration of correct treatment. For example, large fluid resuscitation required for a patient in hypovolemic shock can cause immediate decompensation if administered to a patient with acute cor pulmonale, and inotropic therapy initiated in a volume-depleted patient may similarly result in death. 6
Considering the initial diagnosis of shock in all patients, 55 of the 100 patients were evaluated as having hypovolemic shock; 19, distributional shock; 8, cardiogenic shock; 6, obstructive shock; and 12, complex shock. While the diagnosis was made by U/S in 91 patients, all prediagnostic evaluations made by excluding other shocks in the remaining 9 patients were confirmed by the relevant consultant physicians.
This study highlights the efficacy and utility of bedside U/S guided by the RUSH protocol within the initial critical minutes of patient evaluation in the ED. The consequent narrowing down of potentially life-threatening conditions within the first critical moments upon ED admission has significantly enhanced clinical outcomes.
This approach, managed solely by ER physicians trained in basic and advanced U/S, not only streamlines the workflow but also ensures that diagnostic agility is not compromised because of the unavailability of specialist radiologists. The uniformity in performing these evaluations within the first 10 minutes by the same physician ensures consistency and reliability of the results. This rapid evaluation and diagnostic process, as demonstrated in our study, highlights the significant advantages of integrating U/S into the initial management of patients with shock in the ED, thereby contributing to the existing literature and clinical practices.
Limitations
This study was limited by its pre-experimental design and the convenience sample of patients recruited. Given the threats to internal and external validity, the results cannot be generalized beyond those specific to this cohort of patients.
Conclusion
The RUSH protocol is a practical and effective method for the early systematic assessment of patients presenting to the ED with signs of hypotension and shock. By evaluating the pumping function, body volume status, and vessels of the heart, the RUSH protocol aids in the prompt diagnosis of the underlying causes of hypotension and shock.
Early diagnosis and treatment are crucial, particularly in patients with hemodynamic instability. The application of the RUSH protocol with bedside U/S in patients presenting to the ED with hypotensive symptoms and circulatory disorders can significantly contribute to effective emergency treatment and reduced mortality rates. In addition, it may be valuable to monitor treatment responses through repeated evaluations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from (Cukurova University Non-interventional Research Ethics Commitee [Approval number 28 on February 14, 2014]) (Decision #28).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed the guidelines provided by the ethics committee and the IRB (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment were not followed in this study because no animals were used.
Trial Registration
Not applicable.