
Abstract
Intraocular foreign bodies (IOFB) present differently depending on the type of material (wood, glass, metal) for the IOFB, extent of the injury, and location of the injury. IOFB and the injury can cause a perforation or penetration of the globe which can require more extensive treatment including surgery. Proper evaluation of the IOFB and injury can help to determine extent of the injury, the prognosis of the vision, and health of the eye before and after treatment but may be difficult for the physician depending on the view of the posterior chamber being compromised by media or simply by patient sensitivity. The extent of the injury may also prevent proper evaluation due to swelling, lacerations on the lids, or pain. Proper ophthalmic sonography can provide a quick evaluation of the globe for any IOFB in both the outpatient setting as well as emergency department setting. Evaluation via sonography may allow the physician to accurately diagnose and properly treat the patient to help restore and prevent further loss of vision.
Keywords
Ophthalmic sonography utilizes sound waves emitted from a transducer which is reflected or absorbed by anatomy of the eye. The electrical signal is then relayed back to the computer and converted to an image. Sonography can be used to evaluate both the anterior and posterior aspects of the globe. A foreign body will appear hyperchoic on a sonogram and will appear as a bright white line or area on the image if an intraocular foreign bodies (IOFB) is present. 1 Proper evaluation of IOFB can be difficult on slit lamp exam or fundoscopy, due to injury caused by the IOFB. Physicians can utilize other means to help them in their evaluation and ophthalmic sonography is one of those tools. Whether performed by the physician or sonographer proper technique can provide valuable information of the eye or injury to the eye in both outpatient clinical setting, emergency department, and urgent care. Ultrasound equipment systems are relatively inexpensive, and training can be performed by a Certified Diagnostic Ophthalmic Sonographer (CDOS).
Case Study
In early June of 2019 a 73-year-old male was working on his trailer beside the road when a truck drove by and blew some debris into the patients face. Patient stated he was not wearing any eye protection at the time. He felt immediate pain in his left eye, he rinsed it out and looked in the mirror and everything seemed normal. A few hours later the pain returned along with redness and blurred vision. Two days later, the patient went to urgent care and was referred to ophthalmologist. The patent was seen by an ophthalmologist the following day.
The attending ophthalmologist performed an ophthalmic sonogram without noting an IOFB. The attending drew fluid from the eye and injected antibiotics. The patient was to be follow by an optometrist who treated with drops. Pain and photophobia (light sensitivity) were resolved with drops along with vision improvement. Patient was then referred to second ophthalmologist for cataract extraction consult. Prior to scheduling surgery, the patient had computerized tomogram (CT) performed that was ordered by the second ophthalmologist and showed possible IOFB.
Patient was referred to a third ophthalmologist, at which time the patients vision measured 20/300 in the left eye with notable pain and redness. The physician ordered ophthalmic sonography of both the anterior and posterior chamber in combination with anterior photos of the iris. With proper technique on sonography an IOFB as well as a retinal detachment, endophthalmitis and traumatic cataract caused by the IOFB was noted on the sonogram (Figures 1–3) and protrusion of the IOFB was seen on the anterior photo of the iris (Figure 4). Patient was consulted same day by a retinal ophthalmologist and scheduled for surgery to remove the IOFB and repair the retina. The IOFB was a 1 cm (approximate) bristle from a wire grinding brush (Figure 5). IOFB was removed, retinal detachment was repaired twice, and cataract was removed as well. One year later patient’s vision measured 20/50 with correction.
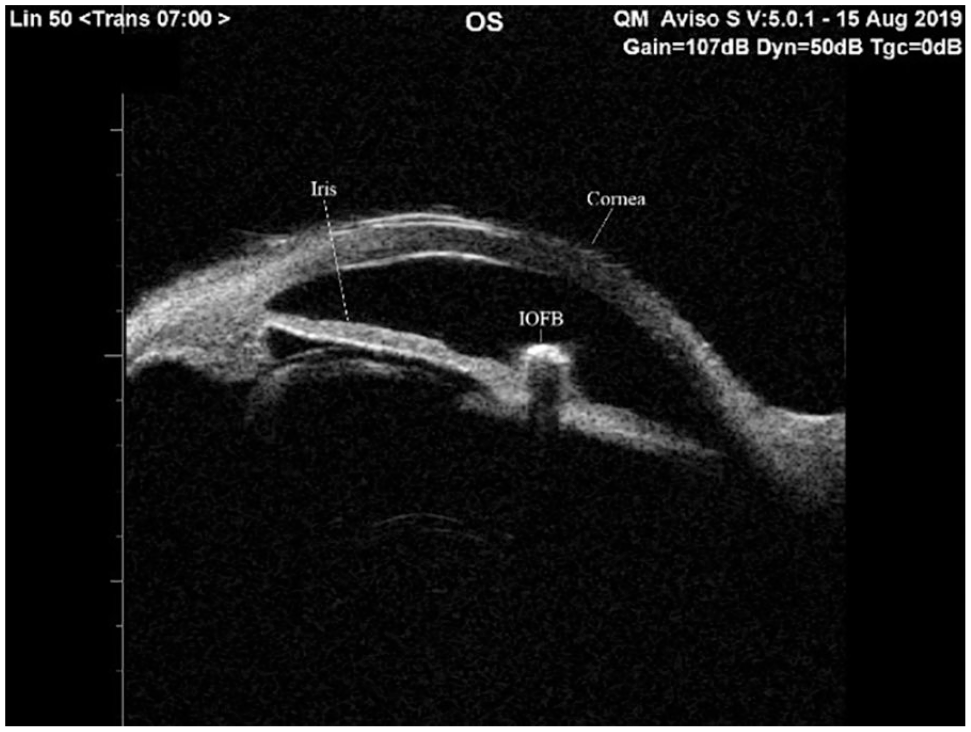
Demonstration of IOFB on immersion sonography technique using a transverse cut of the area. IOFB, intraocular foreign bodies.
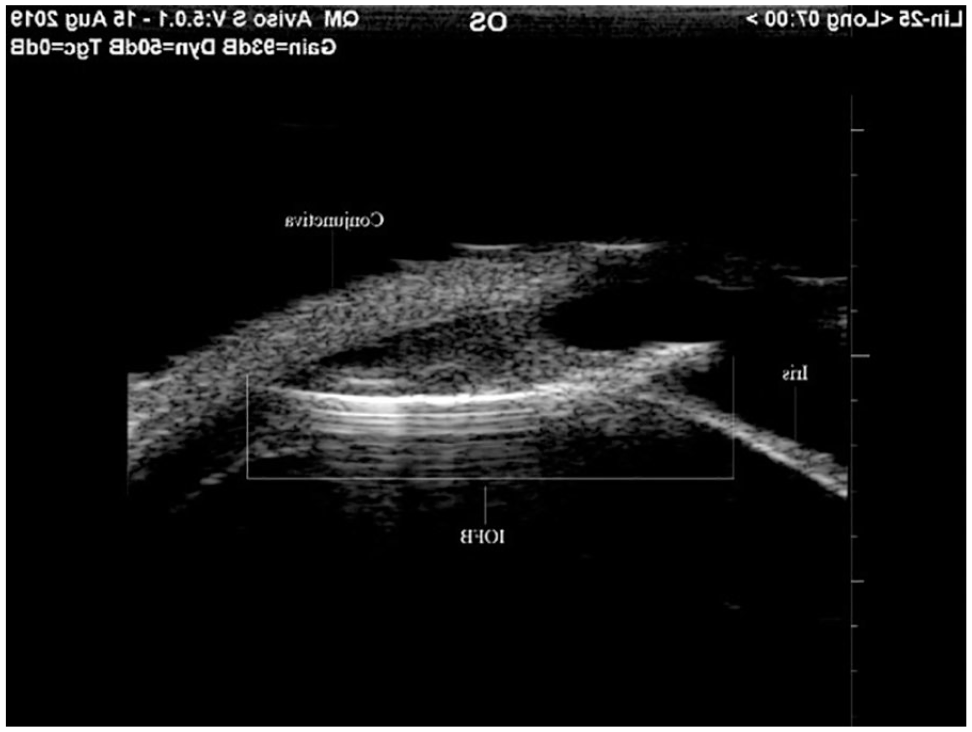
Demonstration of IOFB on immersion sonography technique using a longitudinal cut of the area. IOFB, intraocular foreign bodies.
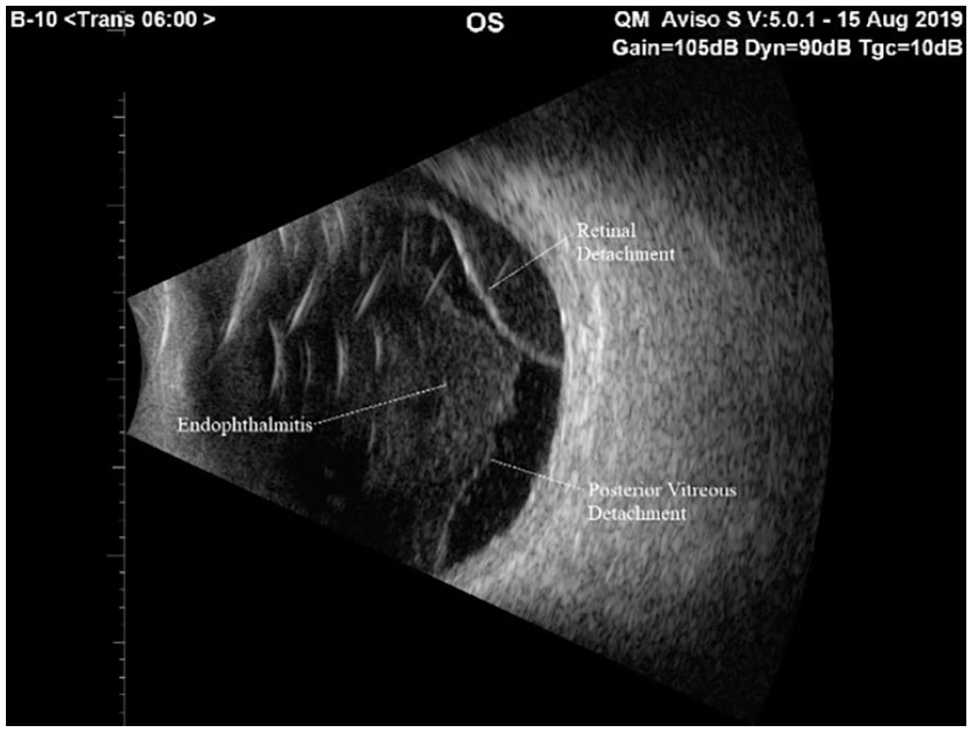
Demonstration of retinal detachment, vitreous detachment, and endophthalmitis on posterior sonography.
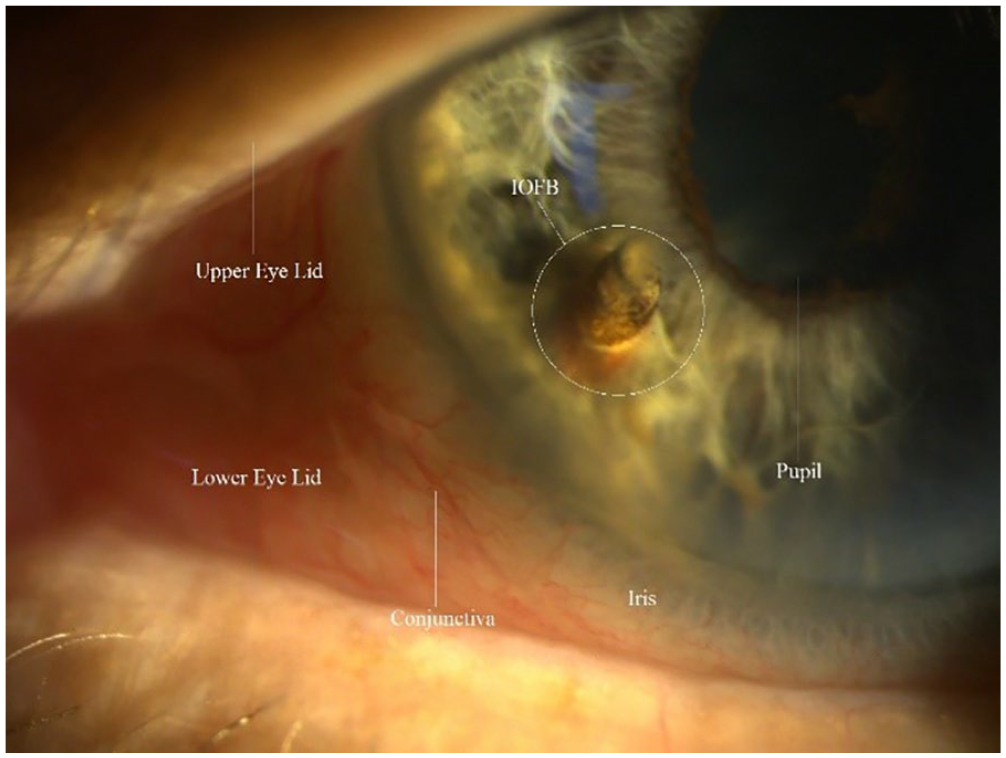
Demonstration of iris with IOFB protruding as seen on slit lamp photography. IOFB, intraocular foreign bodies.

IOFB after removal. IOFB, intraocular foreign bodies.
Discussion
Two months after the initial injury this patient was finally able to get proper treatment for the IOFB and extending injuries caused by the accident and vision was restored to 20/50 after multiple surgeries to remove the IOFB, cataract, and repair the retina. If proper technique was used on the initial sonogram, the patient may have been treated sooner and avoided infection and possibly gained a better vision outcome. It would have also avoided multiple office visits with a second, third, and fourth ophthalmologist and having to have a CT completed.
IOFB are seen in approximately 18-41% of open globe injuries which make up about 3% of all emergency room (ER) visits in the United States. 2 Currently, CT is utilized in the emergency depart to determine if there is an IOFB in the eye. 3 This test can be overwhelming for the patient as well as time consuming causing the patient to be more anxious about the extent of the injury. Ophthalmic sonography can be performed quickly and at bed side without the patient having to be moved from the ER. Sonography, like CT can determine intra ocular foreign bodies such as wood, glass, and metal if proper technique is utilized.
Ophthalmic sonography is a quick and noninvasive test that can provide the physician with a great deal of information on patients suffering from pain and/or vision loss that is unexplained following an injury. The test can be performed on a closed eye as well as open eye with the aid of numbing drops such as proparacaine. The utilization of a medium between the probe and eye such as Genteal Gel or another artificial tear gel allows for better signal strength providing a higher quality scan. Proper immersion technique by the sonographer can provide a view of the anterior aspect of the eye. Utilizing the correct probe and with proper technique all of the posterior chamber can be evaluated as well as further past the globe and into the orbit to determine the extent of the injury and see if there is any orbit or muscle involvement.
Along with evaluating the globe and orbit following an injury, unexplained vision loss and pain cause by diagnosis such as posterior scleritis, melanoma, vitreous hemorrhages, retinal tears, retinal detachments, and posterior vitreous detachments all can be evaluated with the use of sonography. Immersion technique can evaluate the angles for angle closure which can present as unexplained pain in the eye as well as nausea.
Conclusion
The case above demonstrates the importance or proper technique of ophthalmic sonography whether done in the emergency department, urgent care, or outpatient clinic for the evaluation of IOFB and extent of an injury as well as to evaluate unexplained vision loss or pain. Sonography is an important and extremely useful tool not only for the ophthalmic community but for ER and urgent care physicians. Relatively low cost and easily portable units are available and training for proper technique can easily be obtained by a CDOS. With high resolution capabilities and user-friendly capabilities, sonography can provide a great deal of information of the eye and surrounding anatomy. Sonography is currently used by retinal ophthalmologist primary to evaluate the globe if there is no view of the fundus or evaluate for retinal/posterior vitreous detachments and used by ocular oncologist to assess and measure tumor size and characteristics. In addition, sonography can help the physician evaluate smaller structures such as ciliary body and angles. The use of ophthalmic sonography in the ER and out-patient clinical setting is a valuable tool that allows the physician to perform a quick noninvasive test to evaluate for an IOFB as well as evaluation for unexplained pain or vision loss.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.