
Abstract
Objective:
A research project was conducted to determine what patient education skills, community health education skills, and community outreach activities are included in the US-accredited diagnostic medical sonography (DMS) programs.
Materials and Methods:
A quantitative, cross-sectional research survey was sent via email to DMS program directors of 245 accredited programs, resulting in 118 (48.2%) completed surveys returned. Written informed consent was obtained from all subjects before the study. The survey assessed the inclusion of 13 specific patient education skills, eight community education skills, and nine community health/outreach activities in DMS programs.
Results:
Of the 12 patient education skills, 11 were routinely included in 90% of programs. The remaining skill of patient negotiation was included in 75.1% of programs. For patient education skills, 69.4% were required by programs, and 30.6% were encouraged by programs. Community education skills were less commonly included in DMS programs, with 27.4% to 51.3% inclusion rates. The most common community education skill was tailoring messages to intended public audiences. Community outreach activity inclusion in programs ranged from 32.5% to 66.7%, with 77.5% only encouraging participation. Health fairs, health screenings, and self-care education were the most common activities. Incorporating community-related skills into the curriculum was listed as a “good idea” by 72.6% of program directors.
Conclusion:
Patient education skills are routinely required or encouraged in almost all responding educational programs. However, most DMS programs do not require or encourage community education skills. Community outreach activities are not generally required or encouraged by DMS programs, with health fairs and screenings being the most common. Time constraints are the most cited reason for not including community-related content or activities in the programs.
Keywords
When a health care professional interacts with a patient, three distinct interaction levels occur. The first and most important is the professional competency in delivering care, including therapies and diagnoses. The second level involves interpersonal skills such as informed consent and procedural information. The third level is the most broad-based and involves patient education, information exchange, and, at times, community education.
The World Health Organization describes patient education as “helping the patient . . . to acquire knowledge and competencies about the disease and its treatments, in order to better collaborate with the caregivers, and to improve their quality of life.” 1 Pedersen et al. 2 noted that patient education is any planned educational activity designed to improve patient’s knowledge and health behaviors. This study investigated the teaching of patient education, community education, and community outreach skills in diagnostic medical sonography (DMS) programs, in the United States. As witnessed during the COVID-19 pandemic, public health, community outreach, and health education profoundly impacted patient populations. Acknowledging the benefits of public health practice within the US health care system, national associations of medical and allied health professions have pushed for core interprofessional education competencies to emphasize the integration of public health and clinical care (IPEC). 3 With the growing burden of chronic disease and comorbidities, strategies to promote health, prevent illness, improve health outcomes, and reduce health disparities include collaborative efforts to educate and care for individuals, families, patients, and communities. 4 In this direction, US medical education has begun incorporating public health philosophy in clinical practice. This philosophy expands the focus of care solely away from the individual patient’s presentation toward integrating social and behavioral determinants of health into practice. Merging public health, community education, and patient care reflects the shared responsibility of health professionals to promote the health and well-being of the individuals and communities they serve.
This public health philosophy incorporates patient education, community education, and community outreach into clinical practices. This expansion of disciplines is seen throughout health care education. For example, new physicians are encouraged to incorporate public health philosophy in primary care, 5 internal medicine, 6 emergency medicine, 7 psychiatry, 8 radiology, 9 neurology, 10 and pediatrics. 11 Nursing has long engaged in public health efforts and community health education. 12 Numerous other health professions have embraced community outreach and health education, including social work, 13 dentistry, 14 occupational therapy, 15 speech-language pathology, 16 physical therapy,17,18 complementary and integrative medicine,19,20 as well as other clinical fields.21 –23 There are two significant impacts that high-quality patient education and communications can provide. The first is that it improves patient outcomes, both directly and indirectly.24,25 The second is communication skills, including patient education skills, which are essential for any health care professional to function at the highest levels.26 –28
In a systematic review conducted by D’Agostino et al., 24 one of their conclusions was that communication training effectively increases patients’ total level of active participation in health care interactions. This conclusion is supported by Sheehan et al., 25 who conducted a systematic review of the impact of communication between allied health and primary care practitioners, finding that communication skills are crucial for continuity of care. Other literature shows that transversal competencies such as patient education are critical professional skills. Low et al. 26 conducted a scoping literature review on transversal competency development and concluded that these skills are critical for health professionals to build resilience and manage change. A position paper by Akiko and Karolina identifies key transversal skills, including communication skills, that are becoming crucial for front-line health workers to provide effective people-centered care. 27 In another scoping literature review by Bennett et al., 28 communication skills were the second most valuable nontechnical skill in allied health.
There is strong evidence of the value of communication skills, including patient and communication education. However, there is a marked lack of literature on this topic for sonography, even though patient education is an essential responsibility. 29 The Standards and Guidelines for the Accreditation of Educational Programs in Diagnostic Medical Sonography 29 list “demonstrate knowledge of the roles and responsibilities of health care professions to effectively communicate and collaborate in the health care environment” (p. 16) as a curricular requirement. Still, there is no specific mention of “patient education.” Reid-Searl et al. 30 also noted very little literature on patient education in sonography. A few articles addressed patient communications,30,31 and multiple articles addressed “breaking bad news”.31 –35 Patel et al. 36 noted that improved sonographer training is warranted for patient visits and dedicated community outreach events, especially with individuals and families. Sonographers do participate in health fairs,37,38 community-based programs, 39 and interprofessional and community partnerships to perform diagnostic ultrasound procedures, often for underserved communities. 40 With their increasing participation in community outreach and screening efforts, it is valuable for sonographers to use a public lens to contextualize patient education. Outside of a few articles addressing health literacy by patients and families, no community health education articles were found related to DMS.
Based on the healthcare wide movement toward incorporating public health concepts into clinical practice and evidence that these approaches have a positive impact on both patients and practitioners, this study aims to assess the current state of patient and communication education being taught in DMS programs, what community outreach activities are being conducted, and what barriers exist to incorporating these skills into existing programs. The research questions for this study were as follows:
Materials and Methods
In May 2022, the authors received Institutional Review Board approval (IRB# 22-122) to proceed with the study. The survey instrument used in this study was previously developed by Tilson et al. 41 in a study of patient education and community education skills taught in radiation therapy programs. The authors developed the initial survey for the original study using lists of patient and community education skills published in the literature. The survey was pilot-tested and was revised before being distributed. The same instrument was used for this study. The Alchemer software was used for the survey instrument, which contained general demographic questions such as the type of program, the number of faculty members, the number of students, the highest academic degree for the program director, and the publication history of faculty in the program. Then, program directors were asked to indicate how often 13 patient education skills, eight community education skills, and nine community health activities were required or recommended in their programs. The final section of the instrument listed several community health/outreach activities students might participate in, as well as questions about the barriers to incorporating more education skills in the curriculum and if such skills were appropriate for sonographers.
A quantitative, cross-sectional research survey invitation was emailed to all 245 program directors of accredited DMS programs. The program directors’ email addresses were extracted from the Council on Accreditation of Allied Health Programs (CAAHP) website. The program directors received an email invitation explaining the nature of the study, stating that no personal information or institutional identification would be collected and asking them to complete the survey. The first page of the survey was the informed consent and excluded individuals who did not agree to participate. Approximately two weeks after the initial email invitations were sent, a follow-up email reminding the program directors about the survey was sent. The survey was closed after 30 days of data collection.
Data Analysis
Extracted data were exported to International Business Machine (IBM) Statistical Package for the Social Sciences (SPSS). Quantitative data were characterized using descriptive statistics. For categorical items, frequency and proportions were calculated. The median and interquartile range were performed on continuous items that were not normally distributed. Chi-square calculations were performed to determine whether significant associations existed between the demographic information in the survey and the skills list information. A Wilcoxon signed-ranked test compared the median community education skills required by the programs with the median patient education skills required. Post hoc testing was performed on the results using an alpha value of 0.05.
Results
Of the 245 DMS program directors invited to participate in this study, 118 responded, resulting in a response rate of 48.2%. The margin of error for a sample size of 118 is ±9.0% at the 95% confidence level. It is important to note that not all 118 responses were completed in full.
Demographic Information
This study’s program directors were registered diagnostic medical sonographers holding multiple subspecialties. Most oversaw an associate-level program (68, 57.6%) at a community college (61, 51.7%) with 11 to 15 enrolled students each year (29, 24.6%). The modal educational level of program directors was a master’s degree (67, 56.8%), and most completed a certificate program when training for sonography (46, 39.0%) (See Table 1 for complete demographic information).
The Study Participant’s Demographic and Educational Program Information.
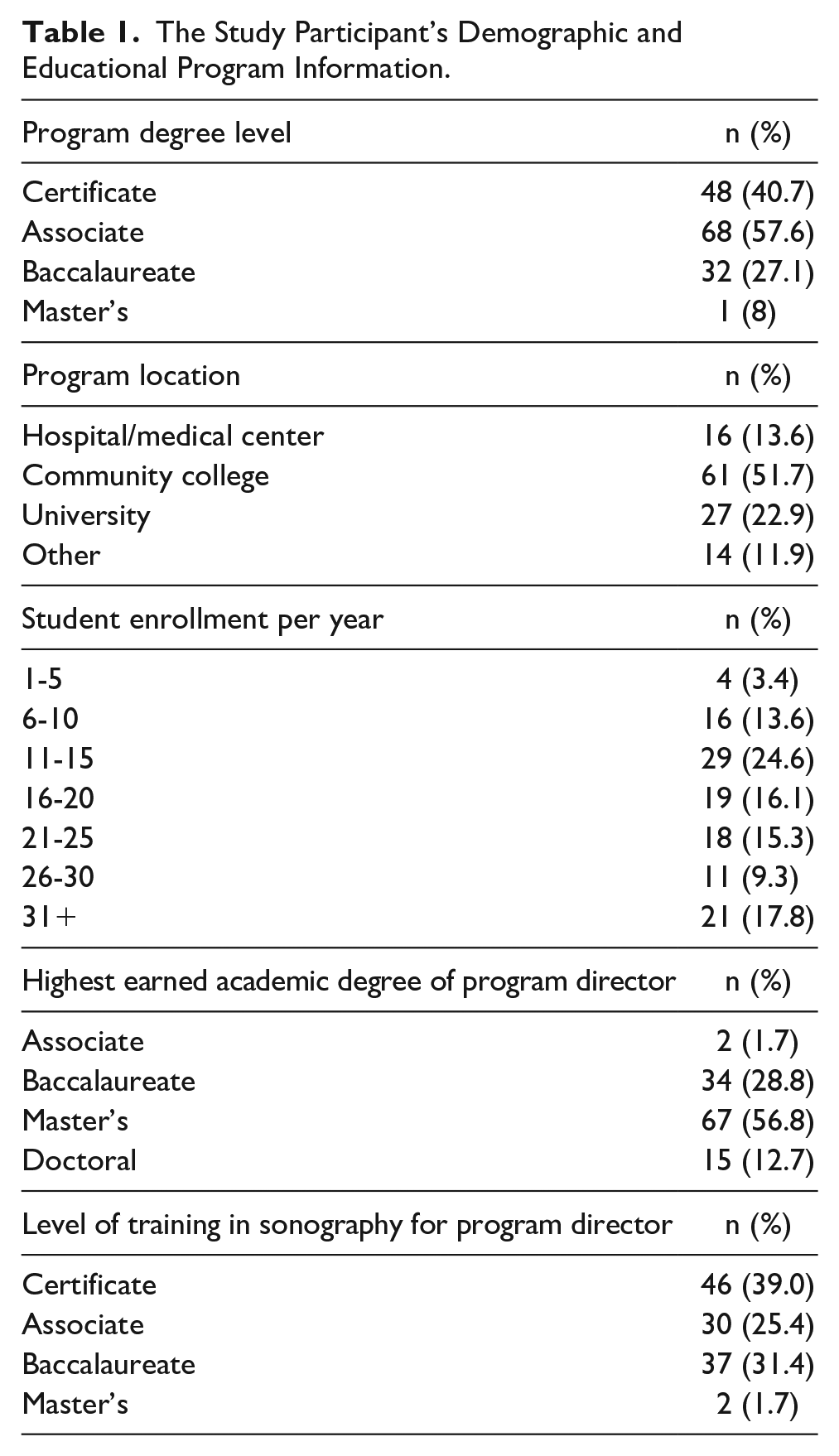
The DMS program directors reported a median number of full-time faculty members of 2 (interquartile range [IQR] = 2-3) and part-time/adjunct faculty members of 2 (IQR = 1-3). They also indicated a mean number of clinical sites of 17.5 (IQR = 12-26.5). The median number of faculty members who published a peer-reviewed journal article was 0 (IQR = 0-1). The median number of faculty members who published a non–peer-reviewed article was 0 (IQR = 0-0.75).
Patient Education Skills
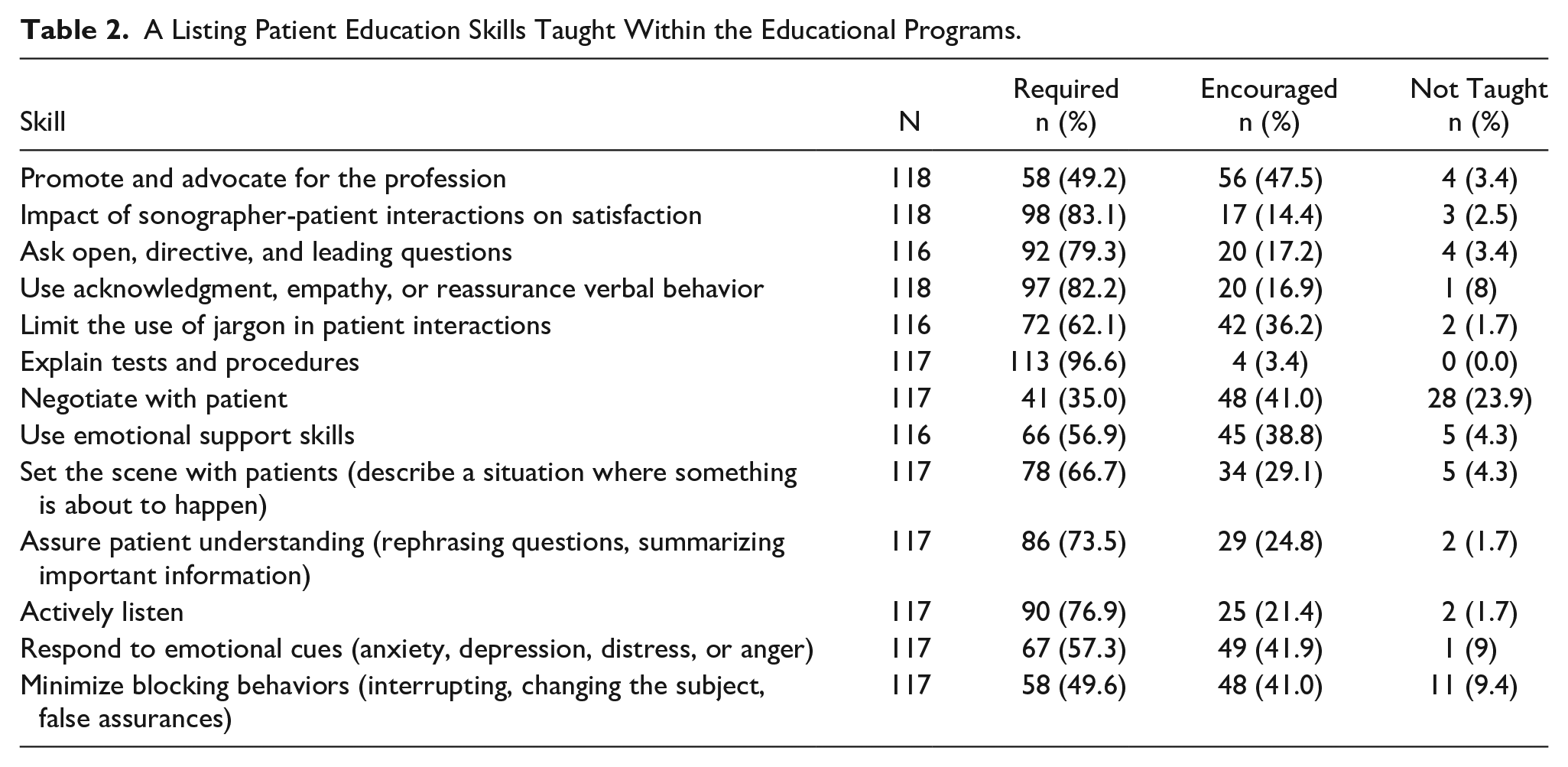
Participants were provided with a list of competencies associated with patient education and were asked to identify whether the skill was required, encouraged, or not taught in their respective programs (See Table 2). Explaining tests and procedures to patients had the greatest number of required responses (113, 96.6%). Promoting and advocating for the profession had the greatest number of responses for skills that were encouraged (56, 47.5%). The skill least taught was negotiating with patients (28, 23.9%). The median score for patient education skills was 21 of 26 possible (IQR = 18.8-24).
A Listing Patient Education Skills Taught Within the Educational Programs.
Community Education/Outreach Skills
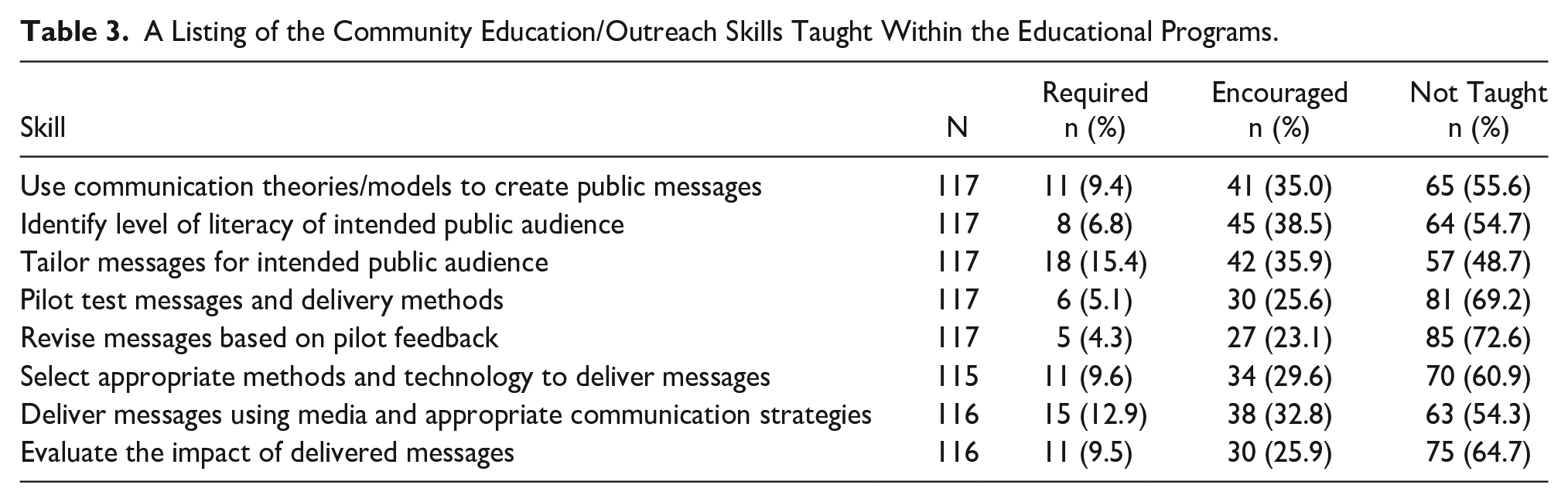
The DMS program directors were provided with a list of competencies associated with community education and outreach and were asked to identify whether the skill was required, encouraged, or not taught in their respective programs (See Table 3). Tailoring messages for the intended public audience had the greatest number of responses for skills that were required (18, 15.4%). Identifying the literacy level of the intended public audience had the greatest number of responses for skills that were encouraged (45, 38.5%). Revising messages based on pilot feedback was the most common skill not included (85, 72.6%). The median score for community education and outreach skills was 2 of 16 (IQR = 0-8).
A Listing of the Community Education/Outreach Skills Taught Within the Educational Programs.
Comparing the medians for patient and community education skills, a Wilcoxon signed-ranked test showed a significant difference: Z = −9.4, p < .001. Sonography program directors reported a significantly higher number of patient education skills being taught (required or encouraged) than community education and outreach skills.
Community Health/Outreach Activities
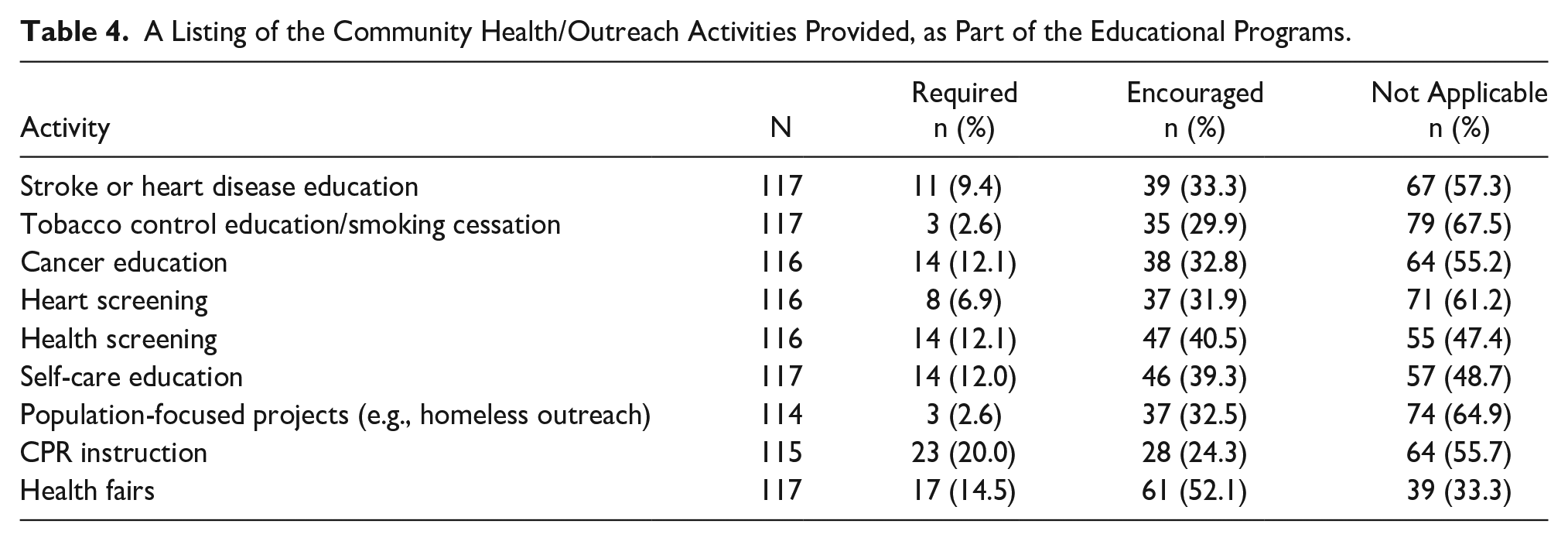
The DMS program directors selected whether students were required or encouraged to participate in community health education outreach activities (See Table 4). Most program directors required participation in cardiopulmonary resuscitation (CPR) instruction (23, 20.0%) and health fairs (17, 14.5%). The most encouraged participation was in health fairs (61, 52.1%), health screenings (47, 40.5%), and self-care education (46, 39.3%).
A Listing of the Community Health/Outreach Activities Provided, as Part of the Educational Programs.
Barriers
The DMS program directors revealed time constraints (104, 88.1%) as the greatest barrier to students participating in community health and education outreach. Other barriers included funding constraints (54, 45.8%), never gave it much thought (28, 23.7%), not sure where to start (25, 21.2%), no institutional support (17, 14.4%), no interest (5, 4.2%), and not certain (1, 0.8%). Only three (2.5%) program directors indicated no constraints with their students participating in community health and education outreach.
Sonographers’ Role in Public or Community Health Education
The DMS program directors were asked what they believed the role of sonographers should be in public or community health education and outreach. Of the 117 program directors who responded, 77 (65.8%) thought it was a good idea and should be encouraged; 8 (6.8%) stated it should be a formal part of the profession; 28 (23.9%) said it was a good idea but should not be part of sonography education; and 4 (3.4%) indicated it should not be part of the profession for sonographers.
Chi-square calculations did not reveal any significant associations between the role of sonographers in community health education and outreach and program type (certificate [p = .40], associate [p = .12], baccalaureate [p = .44], and master’s program [p = .84]). When assessing the association between the role of sonographers in community health education and outreach and program directors’ level of education, no significant finding was identified: χ2(9) = 14.2, p = .12.
Discussion
A survey sent to 245 program directors of accredited DMS programs in the United States resulted in a return of 118 responses. This survey collected demographic information about the program director and faculty, the number of students in the program, the degree level, and the nature of the program. The survey listed 13 patient education skills, eight community education skills, and nine community health activities. Program directors were asked to indicate if these skills and activities were required, encouraged, or not addressed. There was no significant association between any of the demographic factors and the communication skills or activities factors. There was a significant difference in the median number of patient education skills taught versus the median number of community education skills taught, as the programs required very few community education skills or community activities. Although 72.6% of program directors reported that including community-based skills in the curriculum was a “good idea,” time constraint was the primary barrier to requiring these skills and activities.
Research Question 1
What patient and community health education competencies are taught in DMS programs in the United States? Of the 13 skills listed, all were required (66.8%) or encouraged (28.7%), with one exception. How to negotiate with patients was not required or encouraged by 23.9% of program directors. These findings align with a similar study assessing radiation therapy patient and community health education competencies. 41 These findings suggest that DMS programs place value on patient communication skills. However, there is little or no literature to support this finding.
Research Question 2
What community health/outreach activities are required or encouraged in DMS programs in the United States? Most of the eight community education skills evaluated were not part of the DMS curriculum, with 9.0% required and 30.7% encouraged. The two most required skills were tailoring the message for the intended public audience (15.4%) and selecting appropriate methods and technology to deliver messages with 9.6%. The two least addressed community education skills were pilot test messages and delivery methods, with 69.2% not addressing this skill, and revised messages based on pilot feedback, with 72.6% not addressing this skill. Tilson et al. 41 found similar levels of outreach activities for radiation therapists. These findings suggest that the role of sonographers as community educators is not typical in DMS programs.
Research Question 3
What barriers exist specific to sonography students participating in community health education outreach programs? Responses were received for this item from 118 respondents. The most cited barrier was time constraint, with 104 (88.1%) listing this factor. Other barriers were funding constraints at 45.8% and no institutional support at 14.4%. Of interest is that 23.7% of program directors “never gave it much thought,” 21.2% were “not sure where to start”, and 4.2% were “not interested.” In the study of radiation therapy programs, 41 the top two barriers to outreach were also time constraints and funding.
Research Question 4
Do program directors believe sonographers should have a role in public or community health education and outreach? Overall, program directors supported the idea of sonographers having such a role. Eighty-nine percent of program directors believed that community education and public outreach are good ideas and should be required (65.8%) or encouraged (23.9%) in the curriculum. Only four directors indicated that community education should not be part of the profession. These numbers indicate a mismatch between what program directors believe is in the profession’s best interest and what they can incorporate into the curriculum. In a similar study of radiation therapy programs, 41 33% of program directors believed community outreach should be a required skill, and 52% believed it should be encouraged.
Research Question 5
Is there a significant association between program type and program directors’ thoughts about the role of sonographers in community health education and outreach? Chi-square calculations found no significant association between program directors’ thoughts toward community outreach and program type, with p-values ranging from 0.12 to 0.84.
Research Question 6
Is there a significant association between program directors’ education level and thoughts about the role of sonographers in community health education and outreach? There was no significant association between the program director’s education level and their view on sonographers’ reported role in community education, with a p-value of .12.
Research Question 7
Is there a significant difference in the median number of patient education competencies required compared with the median number of community education competencies required? The finding was significant at p < .001, with most patient education skills included and most community education skills not included in the curriculum.
Limitations
This study had several limitations, which are related to the research design. The pre-experiment design and participant sample, by convenience, provide threats to internal and external validity. The response from these participants is unique and cannot be generalized. An added limitation was that the survey had a 48% return rate, and it is unclear if the results would differ if the remaining 52% of program directors had participated. An additional concern is that the participant’s self-reported data cannot be varied. Third, based on the analysis of responses, one question about community activities appears to be misunderstood by respondents. The community engagement question asked about students teaching CPR classes, but comments suggest it was interpreted as students being CPR-certified.
Conclusion
This study aimed to determine what patient and community education skills were being taught and what community outreach activities were incorporated into DMS educational programs in the United States. Of the 13 patient education skills listed in the survey, only two were not taught or required by almost all programs. Those two were negotiating with patients and minimizing blocking behaviors. The two skills with the highest requirement rate were explained testing procedures at 96.6% and the impact of sonographer-patient interactions on satisfaction at 83.1%. This finding aligns with the literature supporting patient education skills associated with patient outcomes. These numbers also indicate that DMS program directors generally value patient education skills in sonographers. One interesting observation is that CAAHP does not explicitly address patient education but only states that sonographers must demonstrate effective communication.
The literature indicates that most health care disciplines incorporate public health models such as community education and outreach into clinical practice. This contrasts with sonography, where very few community education/outreach skills are taught or required in DMS programs. Of the eight skills listed, the most common skill taught was tailoring messages for the intended public audience at 15.4% and delivering messages using media and appropriate communication strategies at 12.9%. Five of the nine community health outreach activities evaluated were not required or encouraged, but most programs either required or encouraged participation in health screenings, heart screenings, and health fairs. These findings are at odds with 72.6% of DMS program directors believing that community-related skills should be part of the profession. Time constraint was cited as the most significant barrier to inclusion. This indicates that the sonography profession may need to consider increasing the minimum educational level to incorporate these additional skill sets. There were no significant associations between the program’s education level, the program director’s education level, the number of faculty members in the program, the type of the program, publication history, and whether patient education skills were required or encouraged.
This study may suggest that program directors consider both patient education skills and community education, as well as outreach skills, as valuable skills for sonographers. There is a high rate of requiring or encouraging almost all patient education skills, although no accreditation requirement exists. However, few community education or outreach activities are incorporated into the DMS program, even though most program directors believe they should be. Such a finding suggests that the DMS profession may want to explore including these skills in future curriculum models.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB# 22-122).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.