
Abstract
There is an increasing demand for sonographer credentials and facility accreditation associated with federal reimbursement of sonography examinations. Therefore, a national survey was conducted to identify the education/certification status of sonographers currently performing studies that receive federal reimbursement. The survey, addressed to sonography administrators, also investigated the sonography laboratory accreditation status. Results indicated that approximately 12% of the sonographers were reported to have no sonography-specific credentials. The primary age range of this group was 25 to 34 years, and 64% were graduates of a two-year (minimum) allied health education program other than sonography. Forty-two percent indicated their sonography lab was not accredited. Should the Centers for Medicare and Medicaid Services (CMS) require facility accreditation, there may be a significant impact on sonographer requirements as a condition of employment.
Keywords
More than 300 million imaging procedures are performed annually on 7 out of every 10 Americans. 1 This includes basic X-ray and/or sonography procedures, which can provide the necessary information for approximately two-thirds of patients requiring diagnostic imaging. 2 Diagnostic medical sonography is a relatively young imaging modality that was first recognized as an occupation in 1973. Two years later (1975), the first national examination was administered to a group of sonographers who voluntarily set the precedent for determination of a minimum standard of education and training. In 1982, Weber State College became the first institution to receive accreditation status for their diagnostic medical sonography education program. 3 Since that time, there has been continual growth in both the number of credentialed sonographers and accredited sonography programs. Currently there are more than 50,000 sonography positions in the United States, and employment opportunities are expected to increase by 18% in less than 10 years. 4
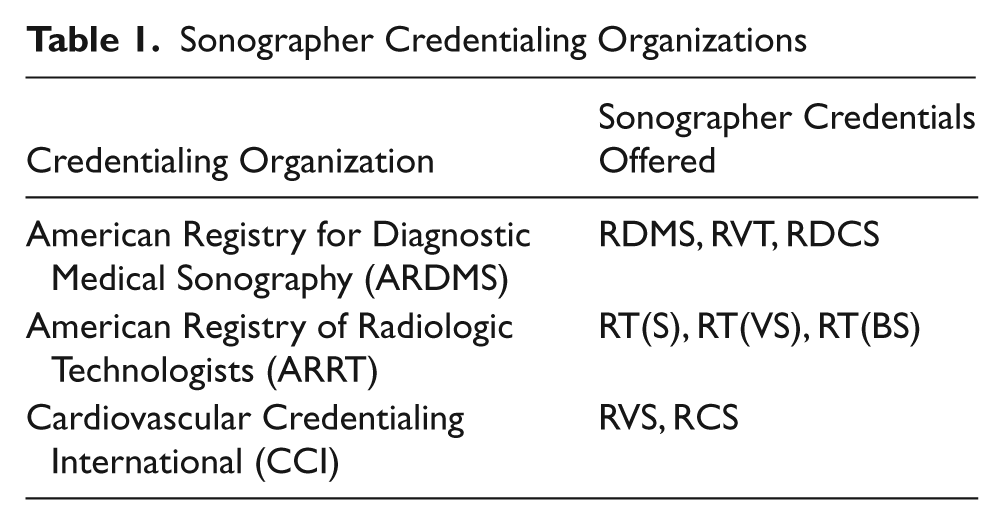
Sonographer credentials can be obtained through the American Registry for Diagnostic Medical Sonography (ARDMS), 5 the American Registry of Radiologic Technology (ARRT), 6 and Cardiovascular Credentialing International (CCI) 7 (see Table 1). Sonography programs may choose to obtain accreditation recognition through regional accreditation, granted to their educational institution, and/or program specific accreditation. Program-specific accreditation agencies include the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Joint Review Committee on Education Programs in Radiologic Technology (JRCERT).8,9
Sonographer Credentialing Organizations
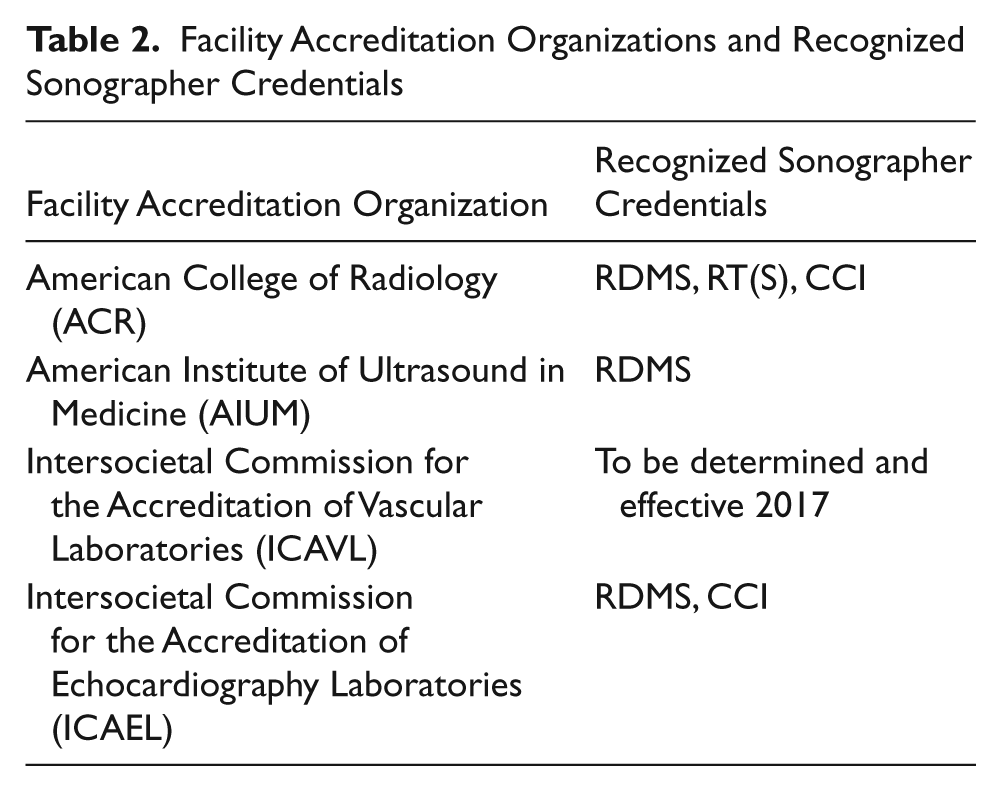
Facilities providing sonography services may also obtain voluntary accreditation status (Table 2). Organizations that provide sonography laboratory accreditation include the American College of Radiology (ACR), 10 the Intersocietal Commission for the Accreditation of Echocardiography Laboratories (ICAEL), the Intersocietal Commission for the Accreditation of Vascular Laboratories (ICAVL), 11 and the American Institute of Ultrasound in Medicine (AIUM). 12 Each of these organizations has slightly different credentialing requirements for the sonographer. The ACR recognizes the RDMS, RT(S), and CCI sonographer credentials. 10 The Intersocietal Accreditation Commission (IAC) offers accreditation for vascular testing (ICAVL), echocardiography (ICAEL), nuclear cardiology, nuclear medicine, PET (ICANL), magnetic resonance (MR) (ICAMRL), computed tomography (CT) (ICACTL), and carotid stenting (ICACSF). 11 The programs that are most often used for sonography laboratories are ICAVL and ICAEL. ICAVL standards state that appropriate (but not yet defined) credentials will be required effective January 2017. 13 The ICAEL will require RDMS or CCI credentials, effective 2014, for both adult and pediatric echocardiographers.14,15 The AIUM recognizes the RDMS credential only, with exception of the RT(S) for breast sonographers. 12
Facility Accreditation Organizations and Recognized Sonographer Credentials
To this point, sonographer certification, sonography program accreditation, and sonography laboratory accreditation indicate a recognized level of excellence, but the requirement for any of these is, for the most part, voluntary. Until a minimum standard is mandated, consumers may be wrongly assuming the quality of the sonography examination they may be receiving.
In 1996, the World Health Organization (WHO) convened a study group to investigate the need for adequate training and education of those performing diagnostic sonography examinations. The resulting report, published in 1998, included the following information:
The use of diagnostic ultrasound by individuals without proper training and experience adds to the likelihood of unnecessary examinations and misdiagnosis. . . . The proper, safe, and effective use of diagnostic ultrasound is therefore highly dependent on the user, who has a major impact on the examination’s overall benefit. . . . For this reason, standards for ultrasonography training are a prerequisite for the provision of diagnostic ultrasound services of high quality.16(p2)
Although global consensus regarding sonographer training was generated many years ago, currently there are no federally mandated education or credential requirements related to individuals performing medical imaging examinations in the United States. There has, however, been considerable effort over the past 2 decades to address this issue.
Since 2000, there has been continual legislative lobbying action to ensure that all persons performing diagnostic imaging attain a minimum educational and training standard. The Consistency, Accuracy, Responsibility, and Excellence in Medical Imaging and Radiation Therapy Act (CARE bill), drafted in 1998, was sent to Congress in 2000 with unsuccessful passage. The CARE bill continues to be introduced before Congress annually, gaining increasing support by stakeholders each year. One of the predominant support groups is the Alliance for Quality Medical Imaging and Radiation Therapy, composed of more than 26 organizations representing a constituency of more than 750,000 allied health care professionals. The CARE bill specifically addresses the technical/ professional education and credential requirements of individuals performing diagnostic imaging examinations reimbursable by the Department of Health and Human Services, which includes Medicare and Medicaid. 17 According to the proposed CARE bill, federal reimbursement for an imaging examination performed by an individual not meeting the specified education or credential requirements may be denied. Upon enactment of the bill, there will be a set amount of time for those not meeting those mandates to become compliant. 17
In 2007, the CARE bill was sent to the US Government Accountability Office (GAO) for review and recommendation. The GAO reported that the Centers for Medicare and Medicaid Services (CMS) spending for sonography imaging services nearly doubled from 1999 to 2004. Approximately 41 million sonography procedures were provided to Medicare recipients in 2005 alone. More than half of those procedures (69%) were performed at sites other than hospitals (physician’s office, hospital outpatient department, skilled nursing facility, etc.). Nearly 47% were performed in the physician’s office. 18 The GAO report presented research findings from claims data, peer-reviewed literature,19-21 and sonography-related professional organizations to support the fact that the skill of the sonographer is critical to correct diagnosis.
Also included in the GAO’s findings was a statement indicating that, according to the American Registry for Diagnostic Medical Sonography, approximately 50% to 60% of those presently performing sonography examinations possess the proper credentials. Therefore, the GAO recommended that sonographers performing federally reimbursed studies be appropriately credentialed or work in accredited facilities. 18
Although the CARE bill has not yet been enacted, there has been considerable regulatory action in support of the GAO’s recommendation. One example stems from the Medicare Modernization Act of 2003 that simplified the numerous Medicare Part A and B fiscal intermediaries and carriers to 15 Medicare administrative contractors (MACs) for regional oversight throughout the United States. Although this transition will not be completed until 2011, certain MACs have already implemented sonographer credentialing or facility accreditation requirement contingencies to receive reimbursement of some sonography examinations.22,23
Another example is found in the Bureau of Labor Statistics (BLS) 2010–2011 description of diagnostic medical sonographers. The section titled “Training, Qualifications, and Advancement” contains the following information:
No States require licensure in diagnostic medical sonography. However, sonographers may become credentialed by one of the professional certifying bodies. Most employers prefer to hire registered sonographers because registration provides an objective measure of an individual’s professional standing. To become registered, one must first become eligible to take the examination by completing the proper education, training, or work experience.
4
It should be noted that since the publication of the 2010–2011 BLS document, two states (New Mexico and Oregon) have enacted state licensure laws, both in 2009, requiring that sonographers be recognized by a national credential/certification body. The growing public awareness of the need for individuals performing sonography to obtain a minimum level of education and training is the culmination of many who have championed the effort throughout the history of this still young imaging modality.3,24-30
Lest one concludes that all diagnostic imaging mandate initiatives are aimed at sonography, federal guidelines for mammography centers were established in 1998 by the US Food and Drug Administration (FDA). The Mammography Quality Standards Act (MQSA) requires accreditation of all mammography facilities. This accreditation may be obtained through a nonprofit accreditation organization or state facility that meets the designated FDA guidelines. Included in these guidelines are educational background, training, and experience requirements for the personnel performing mammography and the physicians reading and interpreting the mammography procedure results. 31 This federal mandate applies to the more than 8000 facilities currently in practice in the United States. 32
More recently, the Medicare Improvements for Patients and Providers Act (MIPPA) of 2008 mandates that imaging centers providing magnetic resonance imaging, computed tomography, nuclear medicine, and positron emission tomography imaging procedures must be accredited by a designated accreditation organization by January 1, 2012, to be eligible for federal reimbursement. The only organizations approved by CMS to handle MIPPA accreditations are the ACR, the IAC, and the Joint Commission. 33 Although the above examples are related to federal reimbursement for imaging procedures, Medicare has historically served as an exemplar for third-party payers. 34
As the momentum for proposed mandatory sonographer education and training standards ensues, it is important to learn more about those currently performing diagnostic medical sonography examinations. The need for this action is further supported by one of the objectives of the Society of Diagnostic Medical Sonography Strategic Plan to “increase the collection, analysis, and dissemination of sonography practice data.” 35 Therefore, a national survey was conducted in March 2010. The primary purpose of this research study was to identify the education/certification status of sonographers currently performing studies that receive federal reimbursement. A secondary purpose was to identify the potential impact on current sonographers, their employers, and the delivery of sonography education if exam-specific certifications were to be required for federal reimbursement. The data are further intended to establish a benchmark of currently unknown statistical information for future research.
Materials and Methods
A literature search was conducted using EBSCO, ERIC, PubMed, Google Scholar, and CINAHL search engines and keywords associated with sonographer credentials, sonographer training, diagnostic imaging, and the CARE bill. The search indicated gaps in information regarding credentialing and accreditation status of departments currently receiving CMS reimbursements as well as needs for initial and additional sonographer training as reform initiatives evolve. Based on these findings, a 19-question demographic survey was developed. The instrument was reviewed by a panel of educators in the radiologic sciences for both readability and content validity. After revision, human subjects’ research approval was obtained through the researchers’ educational institution. The sample population originated from a database consisting of 11,453 hospitals, independent diagnostic imaging centers, physician group practices, single-physician offices, and mammography screening centers currently receiving reimbursement for diagnostic medical sonography procedures from the CMS. 36 From this database, a simple random sample was obtained using Microsoft Excel’s random-number generator and sorting functions (Microsoft, Redmond, Washington). A total of 50 facilities were selected from the database to participate in a pilot study of the survey. Participants were encouraged to include comments regarding the readability and content of the questions. Final survey revisions were made based on pilot survey feedback.
The revised survey was then mailed to 2000 randomly selected facilities and addressed to the sonography department administrator. Recipients were informed as to the purpose of the survey and assured that participation was voluntary and confidential. Recipients could respond via a secure survey Web site or return the paper instrument via postage-paid envelope. Each survey was assigned a number to eliminate duplicate responses. Approximately one month later, reminder postcards were sent to all nonrespondents. All paper instrument response data were manually transferred to the online database, and the data were checked for accuracy by random selection of 10% of the manually transferred survey responses. Data were downloaded into Microsoft Excel and SPSS Statistics 17 (SPSS, Inc, an IBM Company, Chicago, Illinois) for analysis. Descriptive statistics and cross-tabulations were calculated for prevalence and discrimination purposes. Cross-tabulation shows the relationship of the frequency distribution between two categories.
Results
Of the 2000 questionnaires mailed, a total of 323 valid surveys were received, which represents a 16% response rate. Each facility received a numbered instrument that was either returned or the number was input on the Web site, and duplicate numbers would not be accepted to ensure each survey represented a single facility. Coding accuracy, performed on 10% of the manually transferred survey instruments, was 99.98%. Not all respondents chose to provide information for every question on the instrument. Therefore, variations in the sample numbers (n) depicted in individual questions are reflected in the results.
Demographics
The geographic distribution of respondents was categorized by zip code according to US Census Bureau regions and divisions data. 37 Figure 1 demonstrates that a fairly proportionate regional representation was obtained nationwide.
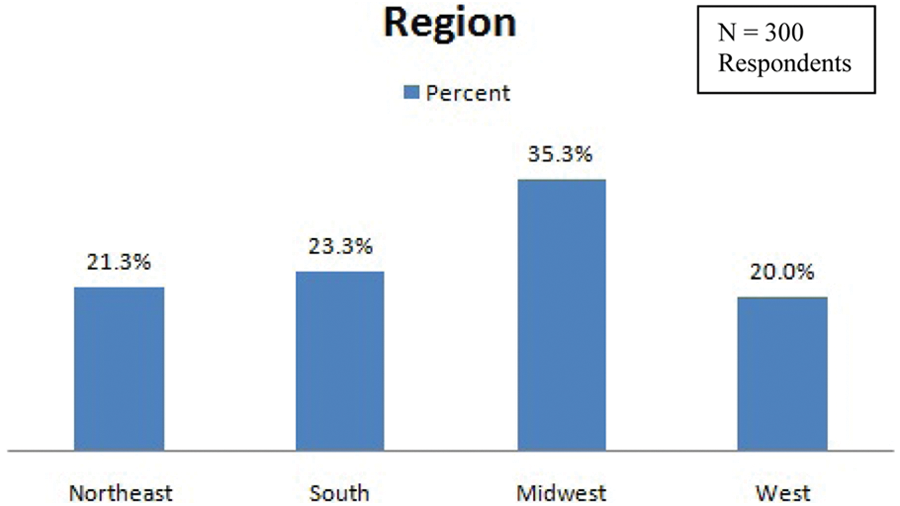
Geographic regional distribution of respondents.
The majority of the respondents were hospitals (83%). The remaining 17%, in order of representation, were independent diagnostic facility groups, physician group practices, single-physician offices, and mammography screening centers (Figure 2). Hospital facilities were further differentiated with respect to size according to bed number. Twenty-five percent were identified as having 50 to 149 beds. The remaining groups were fairly evenly distributed at 14% (less than 50 beds), 16% (250–349 beds), 18% (150–249 beds), and 19% (greater than 350 beds), respectively.
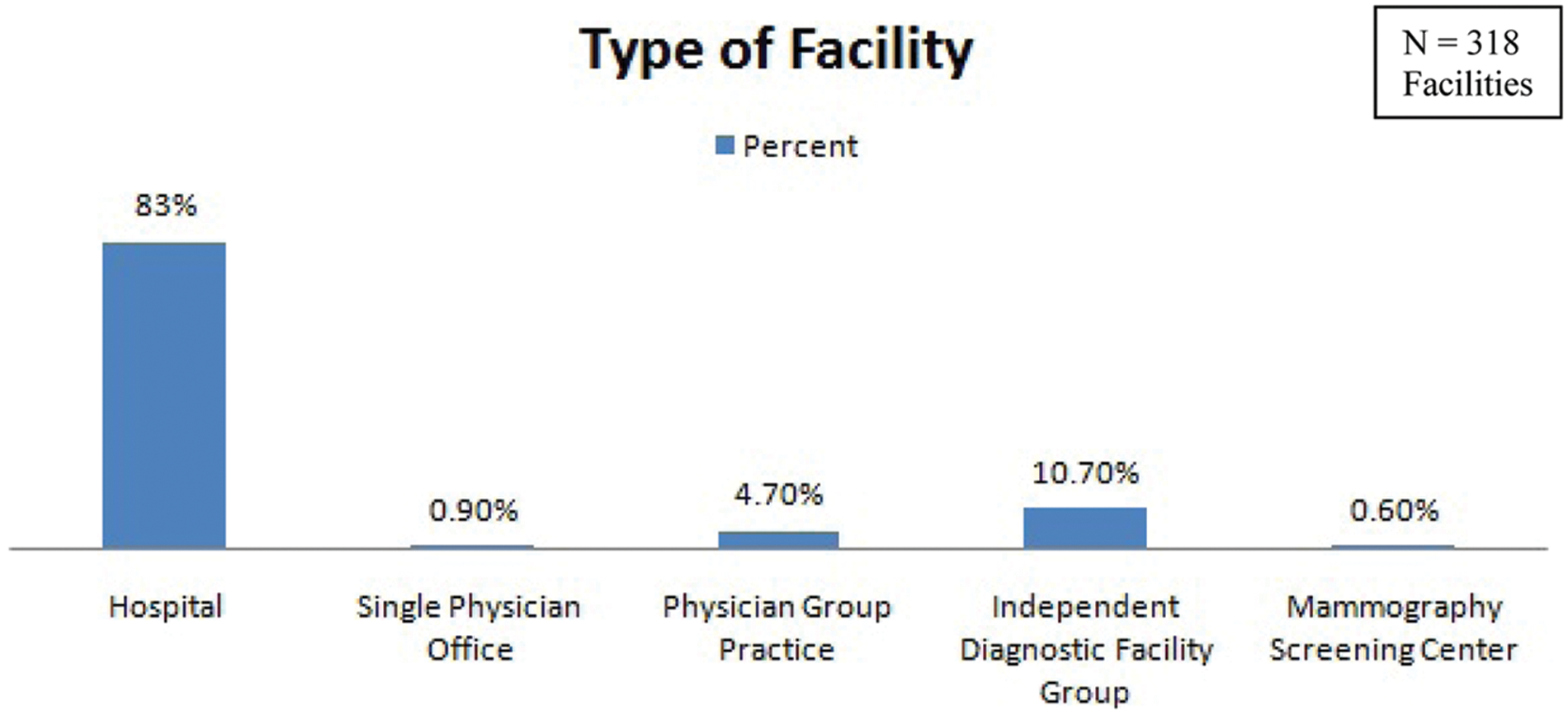
Distribution of responses by facility type.
Next, the respondents were asked to indicate if the sonography lab was accredited and by what agencies. Overall, 58% of the respondents indicated their sonography laboratory is accredited. The majority (48%) were ACR accredited. Accreditation status with ICAEL was indicated by 6.2%, whereas the AIUM and ICAVL were reported by 5.5% each. Some facilities reported accreditation status with more than one agency, and therefore total percentages do not equate to 100%. A considerable number (42%) of the respondents, however, did not report accreditation status through any of the above agencies.
Crosstabs for accreditation status were performed according to facility type and geographic region. The prevalence of ACR-accredited facilities represented the majority regardless of facility type. All of the responding mammography centers reported ACR accreditation. None of the above accreditation agencies were reported by respondents identified as single-physician offices (Figure 3). When comparing prevalence of accreditation type by national geographic regions, ACR was again the most predominant agency reported. Nationwide, the Northeast is most likely to have accredited sonography facilities, whereas the West is most likely to report no facility accreditation at all (Figure 4).
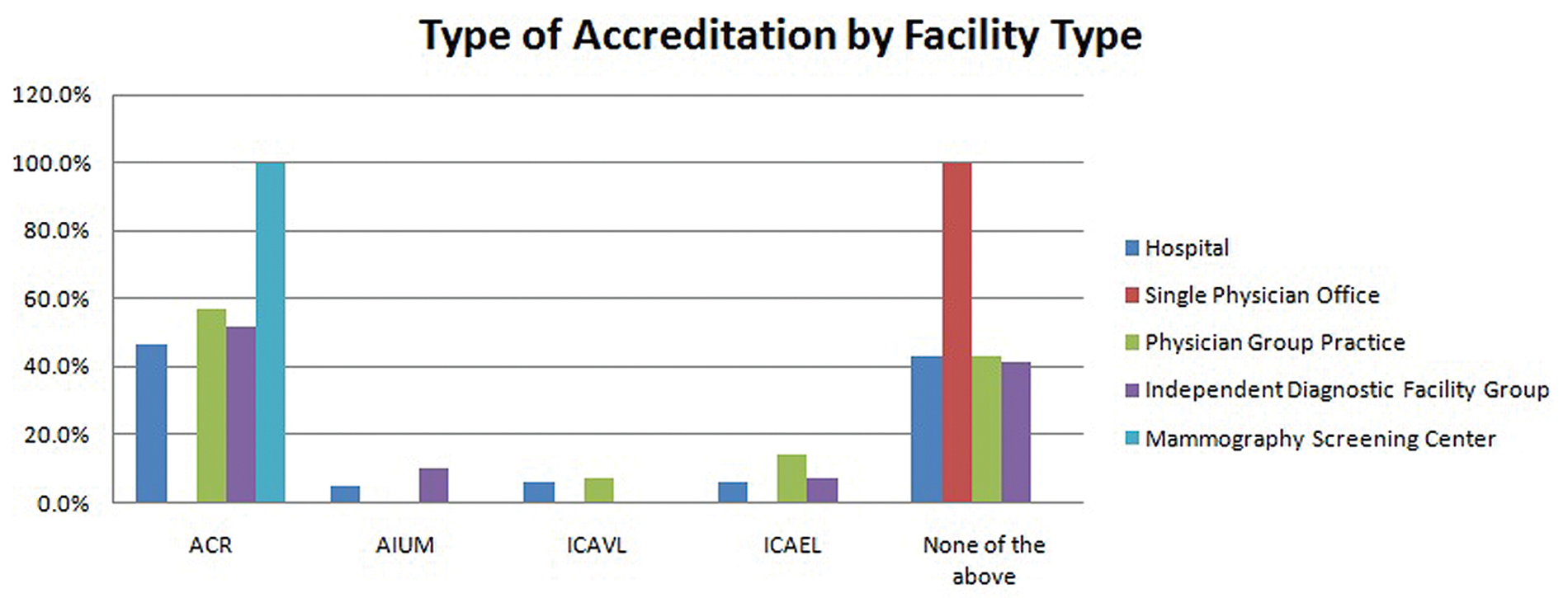
Type of accreditation reported according to facility type. ACR, American College of Radiology; AIUM, American Institute of Ultrasound in Medicine; ICAVL, Intersocietal Commission for the Accreditation of Vascular Laboratories; ICAEL, Intersocietal Commission for the Accreditation of Echocardiography Laboratories.
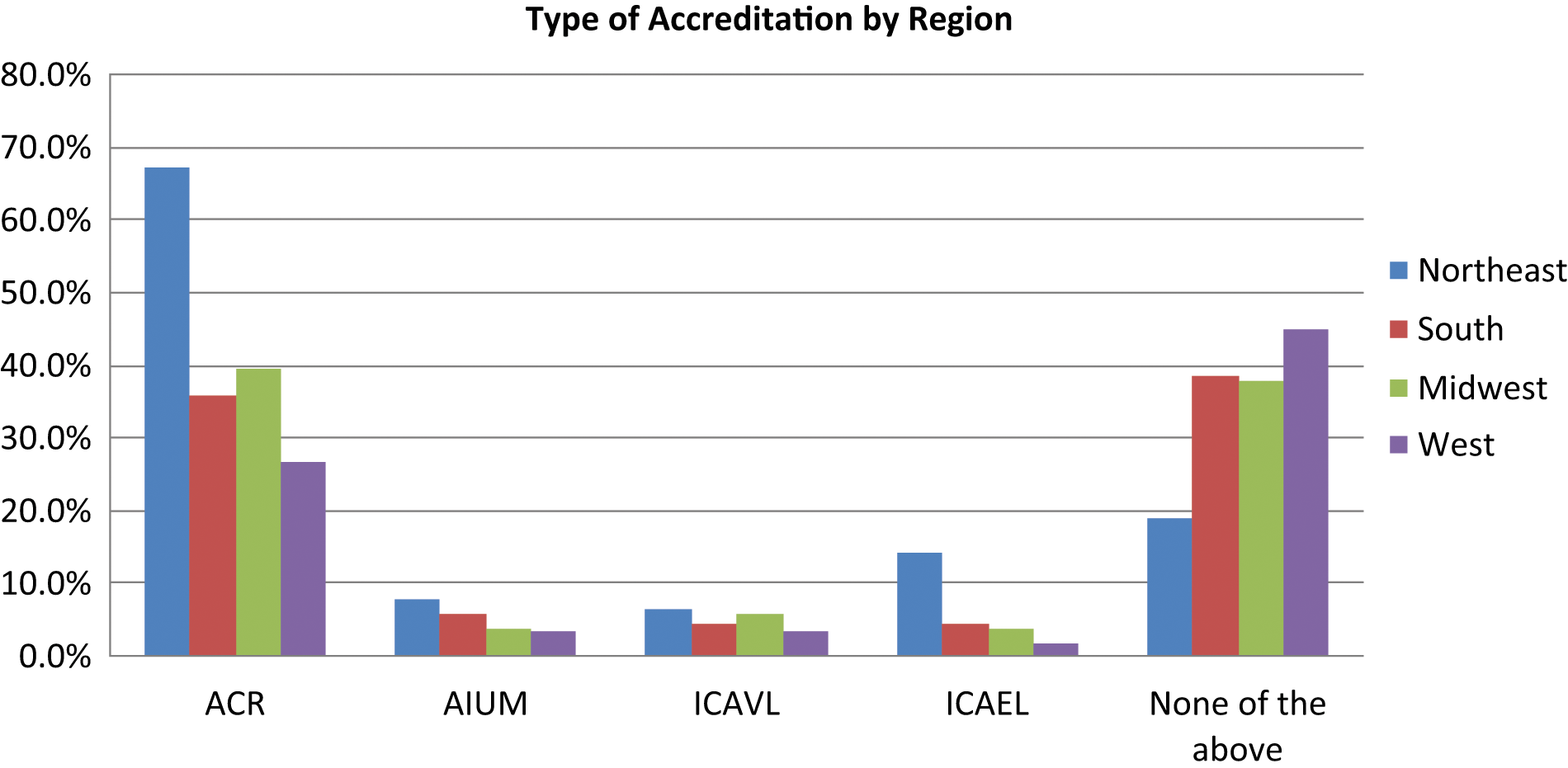
Distribution of type of accreditation status by region. ACR, American College of Radiology; AIUM, American Institute of Ultrasound in Medicine; ICAVL, Intersocietal Commission for the Accreditation of Vascular Laboratories; ICAEL, Intersocietal Commission for the Accreditation of Echocardiography Laboratories.
Sonographer Status
The reported total number of sonographers (defined as individuals performing any type of sonography examination) was 2398. Of this number, a total of 3022 sonography credentials were reported, which indicates multiple credentials were held by some sonographers. Next the respondents were asked to indicate how many of their sonographers maintained one of the following sonography credentials: Registered Diagnostic Medical Sonographer (RDMS), Registered Technologist (RT(S), ARRT), Registered Vascular Technologist (RVT), Registered Vascular Specialist (RVS), Registered Diagnostic Cardiac Sonographer (RDCS), or Registered Cardiac Sonographer (RCS). The RDMS credential was indicated for the majority (62%), followed by RVT (20%), RT(S) (11%), and RDCS (6%). The reported RVS and RCS credentials reported were less than 1% each.
A total of 286 sonographers (12%) were reported to have none of the above listed sonography credentials. The majority of these noncredentialed sonographers are in the 25 to 34 age range. Of this group, 184 (64%) were graduates of a two-year (minimum) allied health education program other than sonography.
Next the respondents were asked if minimum educational/certification mandates were to be tied to federal reimbursement, how many sonographers would need to obtain exam-specific credentials to perform in the following areas: Abdomen, OB/GYN, Vascular, Echocardiogram, and Other. Figure 5 demonstrates the greatest percentage of additional certifications that would be needed by those identified as credentialed sonographers. The write-in response to the “other” category was primarily described as breast certification. For those identified as noncredentialed sonographers, the greatest certification demand was almost equally split between Abdomen and Ob/GYN (Figure 6). It should be noted that three respondents indicated that vascular and cardiac services were in a separate department and were not represented in their responses.
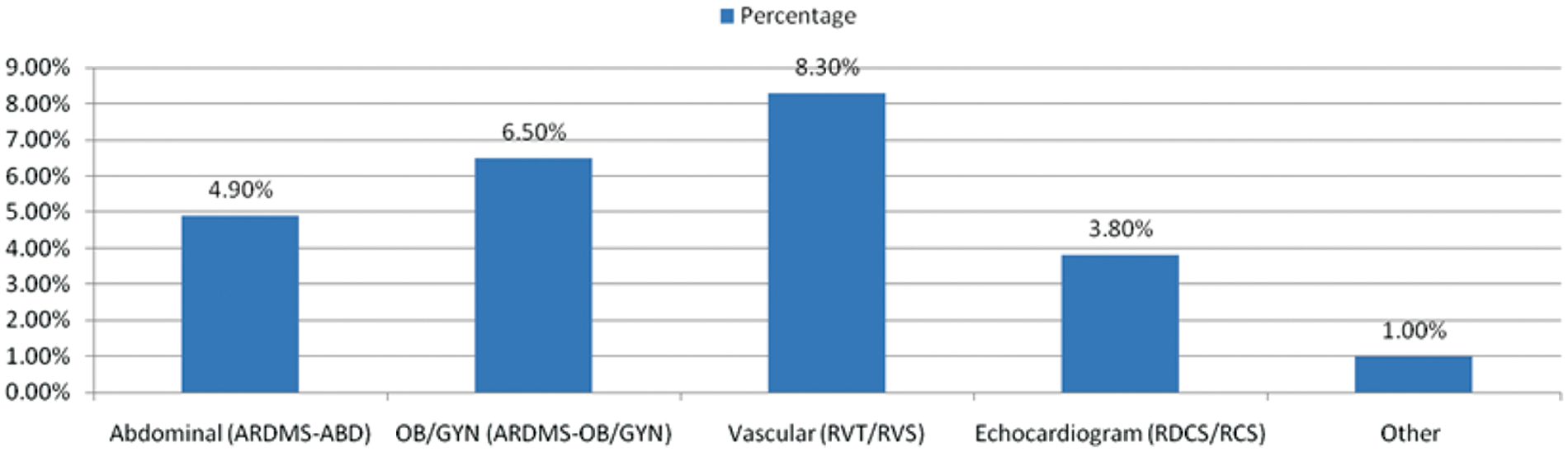
Percentage of additional certifications that would be needed by credentialed sonographers. Total number of credentialed sonographers = 2112. ARDMS, American Registry for Diagnostic Medical Sonography; RVT, Registered Vascular Technologist; RVS, Registered Vascular Specialist; RDCS, Registered Diagnostic Cardiac Sonographer; RCS, Registered Cardiac Sonographer.
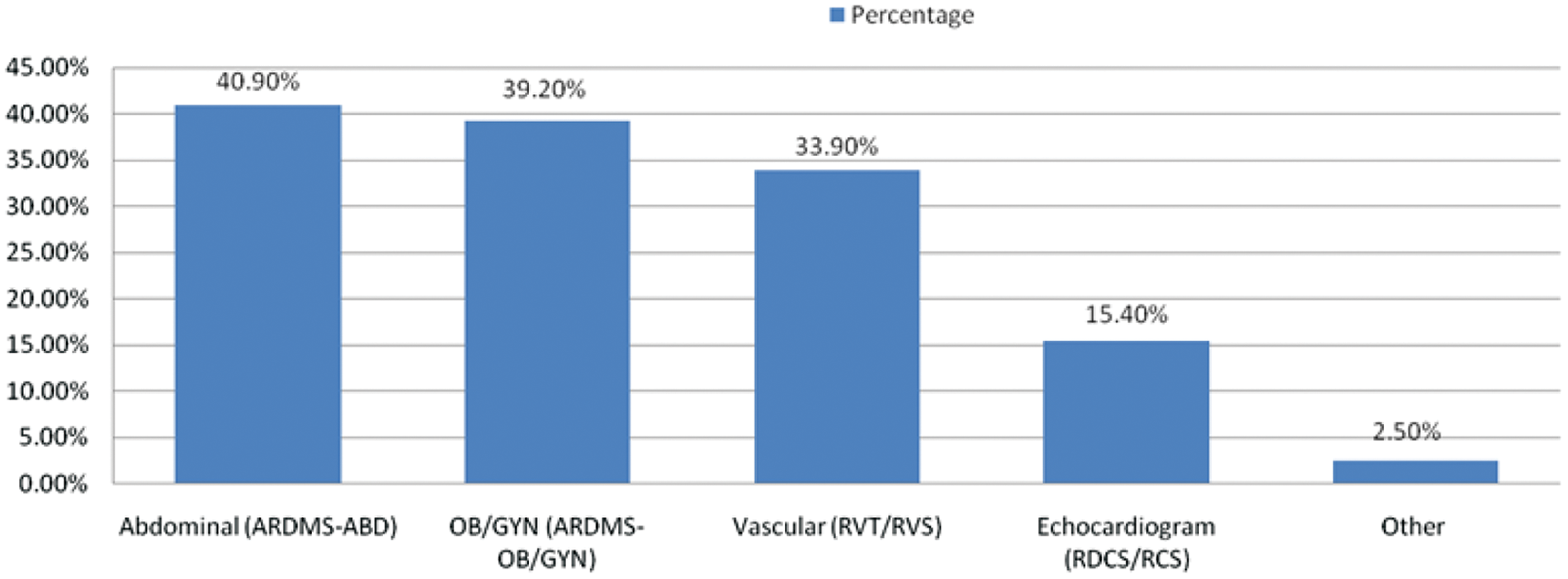
Percentage of certifications that would be needed by noncredentialed sonographers. Total number of noncredentialed sonographers = 286. ARDMS, American Registry for Diagnostic Medical Sonography; RVT, Registered Vascular Technologist; RVS, Registered Vascular Specialist; RDCS, Registered Diagnostic Cardiac Sonographer; RCS, Registered Cardiac Sonographer.
Discussion
The random selection from a database of hospitals, diagnostic facility groups, physician group practices, single-physician offices, and mammography screening centers garnered responses primarily from hospitals. However, there was a fairly even distribution of responses geographically across the nation and a good cross-representation of hospitals categorized by bed size.
The less than 1% response rate from single-physician offices and mammography screening centers does not provide information that could be generalized to the entire population of such facilities. Of the mammography centers responding, all reported accreditation through the ACR. This finding may be supported by the federal MQSA requirement that all mammography facilities be accredited. It should be noted that MQSA mandates for education and training apply to those who perform X-ray imaging of the breast—but not to those who perform breast sonography at those sites. Of more concern was the finding that none of the responding single-physician practices reported accreditation status through any of the listed sonography accreditation organizations.
Results of this study suggest that, among those reporting, laboratory accreditation is primarily obtained through the ACR. It can be assumed that, in accordance with ACR regulations, sonographers at those facilities will become credentialed within a designated amount of time. ACR does not, however, stipulate that all sonographers be required to obtain credentials for each type of examination performed (i.e., Abdomen, Obstetric, Gynecologic, Vascular, etc.). Although 48% of the respondents indicated ACR accreditation, 42% indicated no accreditation with the ACR, ICAVL, AIUM, or ICAEL. Should CMS require facility accreditation, there may be a significant impact on sonographer requirements as a condition of employment. It can be assumed that most facilities hold accreditation through a single organization, as evidenced by the fact that the total percentages, by category, were slightly more than 107%.
Although laboratory accreditation serves as one mechanism for some institutions to qualify for reimbursements, not all accrediting bodies stipulate that every sonographer in a lab be credentialed to achieve this status. However, if the CARE bill legislation is passed, lab accreditation status alone may not be enough for receipt of these reimbursements. Under a post–CARE bill environment, every sonographer will be required to be credentialed to be in compliance, making it even more imperative to identify these individuals and their training and educational needs.
The overwhelming majority of reported credentialed sonographers possess the RDMS certification. The percentage of RVT sonographers is surprisingly low, especially considering the new MAC mandates already under way in some parts of the nation requiring vascular sonography examinations to be performed by credentialed sonographers.
Approximately 12% of all sonographers are reported to have no sonography certifications. The most representative group of noncredentialed sonographers is ages 25 to 34 years. In addition, most noncredentialed sonographers (64%) are graduates of a two-year minimum allied health education program. Educators will need to keep these demographics in mind when formatting and targeting educational opportunities in diagnostic medical sonography. Current programs may want to consider curricular strategies to meet a potential need for currently practicing sonographers to become credentialed or to obtain additional credentials within a fixed allotment of time.
Limitations and Recommendations for Further Research
The interpretation of these findings is not without limitations. One limitation is the self-reporting methodology used in the surveys. The results can only be as accurate as the input from the respondents. A second limitation is that the entire population of those performing sonographic examinations was not represented. Of the 2000 facilities randomly selected from a database containing recipients of CMS reimbursement for diagnostic medical sonography examinations, 323 valid responses were received. A greater response rate would have strengthened the confidence level that these findings are representative of all current sonographers. Furthermore, although the survey was addressed to the sonography department administrator of each randomly selected facility, the respondent may not have included information from all labs (i.e., vascular, cardiac, general) within the institution.
A more comprehensive study of all sonographers currently practicing is recommended to better determine education and training. This information could direct the delivery of future educational offerings designed to meet the needs of those currently in the workforce. Further research on the 42% of institutions without lab accreditation is recommended to better understand what could be done to improve this statistic.
Conclusion
There is an increasing demand for sonographer credentials and facility accreditation associated with federal reimbursement of certain types of sonography examinations. In addition, two states have already enacted legislation requiring sonographers to be licensed and recognized by a national credential/certification body. Should the CARE bill or similar federal legislation make reimbursement contingent on the training and education of those performing these examinations, the impact on imaging facilities will be far reaching. Demand for credentialed sonographers will, in turn, challenge educational programs to meet the needs of those who are already working in the field. Educators will need to explore curricular alternatives to best fit the demographics of those who will be seeking coursework to meet current and future requirements. Until such time as a minimum standard is mandated, consumers may be wrongly assuming the quality of the sonography examination they may be receiving.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Society of Diagnostic Medical Sonography (grant number 241189).