
Abstract
A rare case of bilateral fetal meromelia with duodenal atresia (DA) was diagnosed on three-dimensional (3D) sonography. A 32-year-old G3P2002 with a large for date uterus, was reviewed at 26 weeks’ gestation. The 3D sonogram confirmed the presence of the humerus, olecranon process, and only the proximal third of the ulna bone, bilaterally. The distal ulna, radius, metacarpals, and phalanges were absent on both upper limbs. The bones of the lower limbs were present and appropriate for gestational age. Further evaluation revealed the “double bubble” sign, which is characteristic of DA within the fetal abdomen. The patient was induced 2 weeks later, due to intrauterine fetal demise. The suspected fetal anomalies were confirmed at birth. A high index of suspicion and a detailed sonographic evaluation are essential for detecting rare fetal anomalies, such as meromelia.
Congenital upper limb abnormality (CULA) is a complex spectrum that is classified based on the underlying mechanism and the severity of the abnormality. 1 Meromelia is characterized by incomplete development of at least one limb, resulting in partial absence of the affected limb. Conversely, amelia is denoted by the complete absence of the limb. Both conditions are manifestations of varying severities of the same entity, hence the name amelia-meromelia sequence.2,3
Meromelia is often sporadic, though there have been sparse reports of familial occurrences. 3 It may coexist with other skeletal abnormalities, but the condition is rarely described with nonskeletal abnormalities. The etiopathogenesis of meromelia is yet to be completely elucidated, but it is believed to be related to developmental arrest and congenital amputations, such as the amniotic band syndrome, which is associated with entangled fetal parts, resulting in amputations or deformities. 1 Meromelia has a reported incidence of 1.4 per 100,000 births; 4 prenatal sonographic diagnosis is therefore often missed due to its rarity, and the tendency to measure only a single femur length, during sonography. A prenatally diagnosed fetal meromelia co-existing with a nonskeletal abnormality using three-dimensional (3D) sonography is hereby presented.
Case Report
A pregnant patient, G3P2002 was referred to the fetal medicine section of a Nigerian teaching hospital. The gestational age (GA) of 26 weeks was assumed due to a large-for-date uterus. An earlier sonogram had already confirmed a singleton gestation. There was neither a background medical condition nor ingestion of medications other than haematinics during the pregnancy. There was no history of exposure to radiation before or during the pregnancy. The patient did not have aneuploidy screening done during the pregnancy.
Fetal biometry correlated to the 50th percentile for her GA. There was the presence of polyhydramnios, with an amniotic fluid index (AFI) of 33 cm. A fetal anatomy evaluation was performed, following current International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) 20 + 2 guidelines. 5 The sonographic evaluation revealed a suboptimal humeral length, with absent distal forearm and hand bilaterally (See Figure 1). A 3D skeletal rendering (see Figure 2) confirmed the presence of only the olecranon process and the proximal third of the ulna. The distal ulna, radius, metacarpals, and phalanges were absent. The elbow joints were in fixed flexion without demonstrable mobility on the four-dimensional (4D) sonogram. The femur, tibia, fibula, metatarsals, and phalanges of the lower limbs were appropriate for GA. Further evaluation revealed the double bubble sign, which represents the fetal stomach and dilated duodenal bulb within the fetal abdomen (see Figure 3). The increased AFI due to lack of fetal swallowing and the “double bubble” sign on sonography are pathognomonic of duodenal atresia (DA).
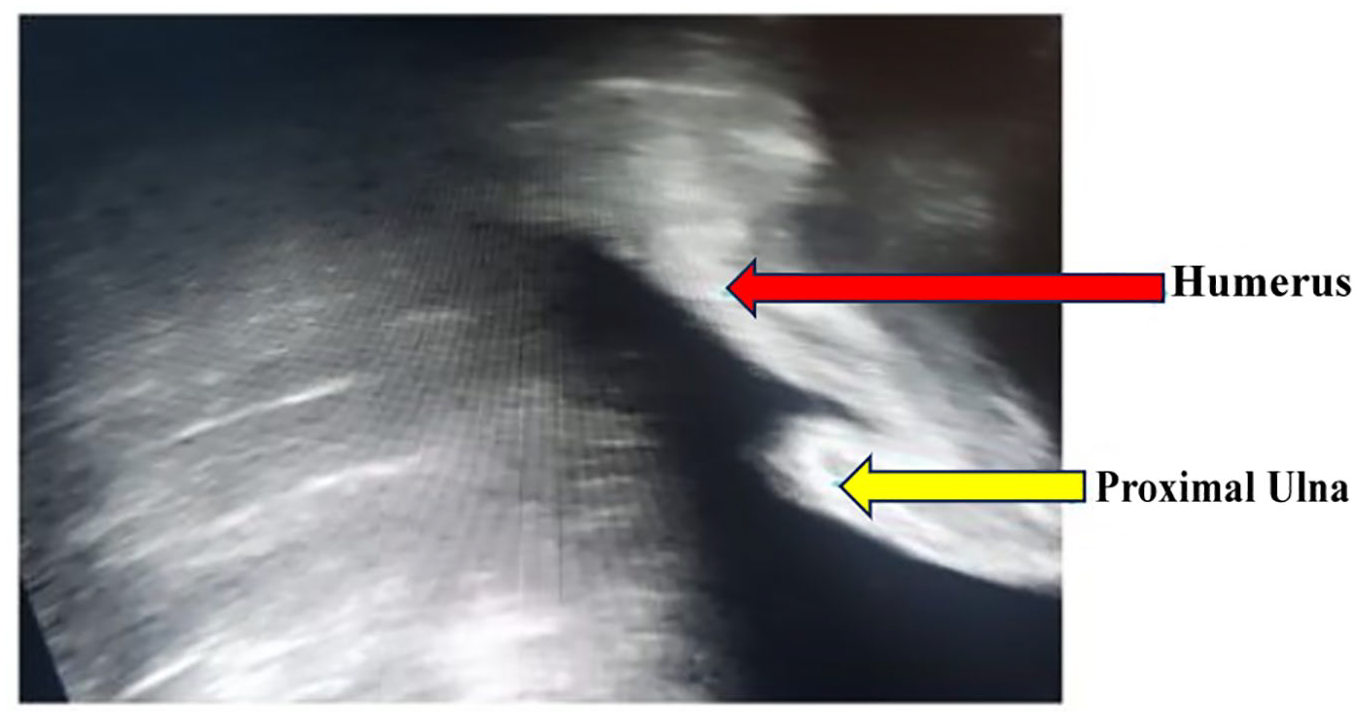
A gray-scale sonogram is provided that demonstrates the upper limb of the fetus, which is comprised of a short humerus and truncated forearm.
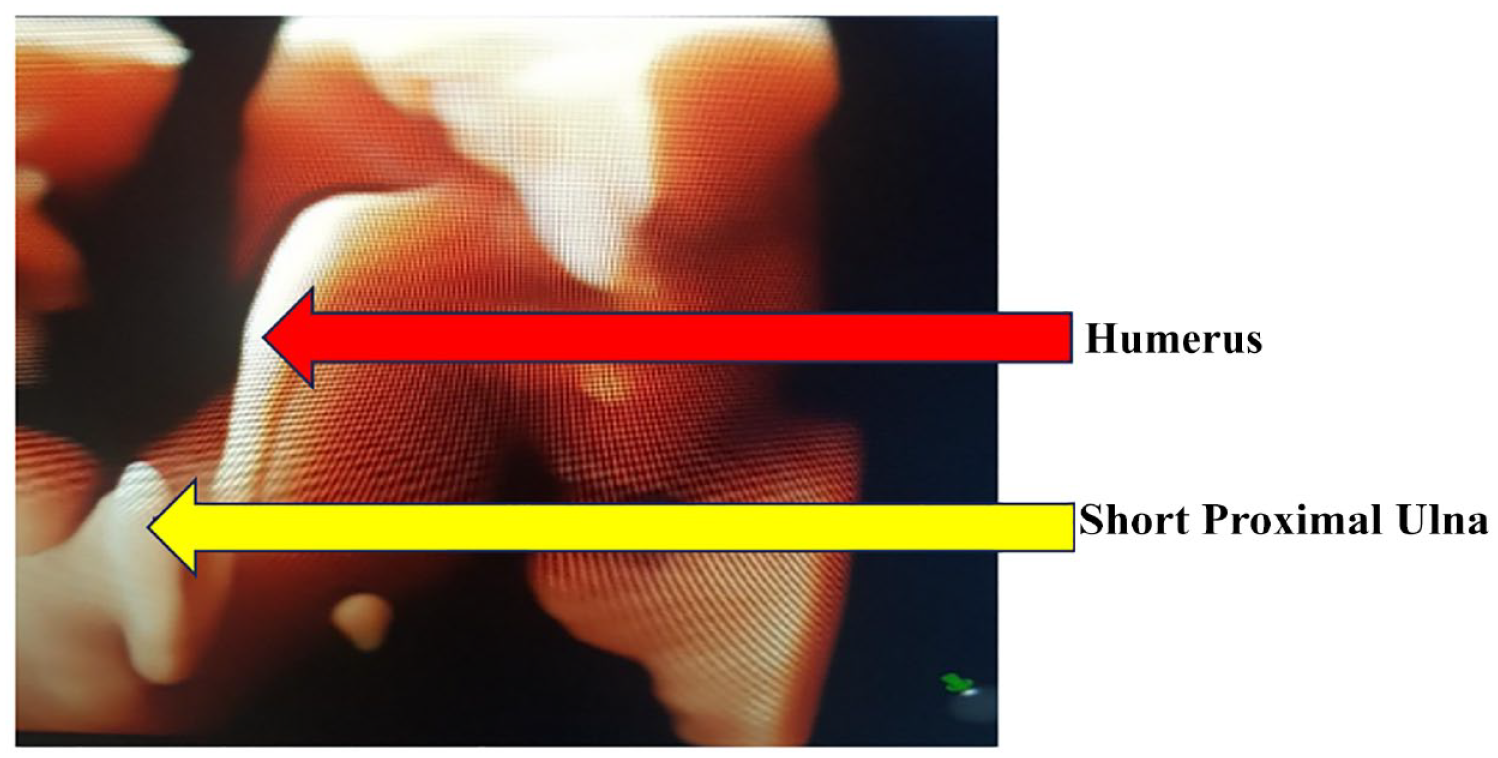
A three-dimensional skeletal rendering of the fetus’ upper limb demonstrated the humerus, proximal ulna, and the absent radius.
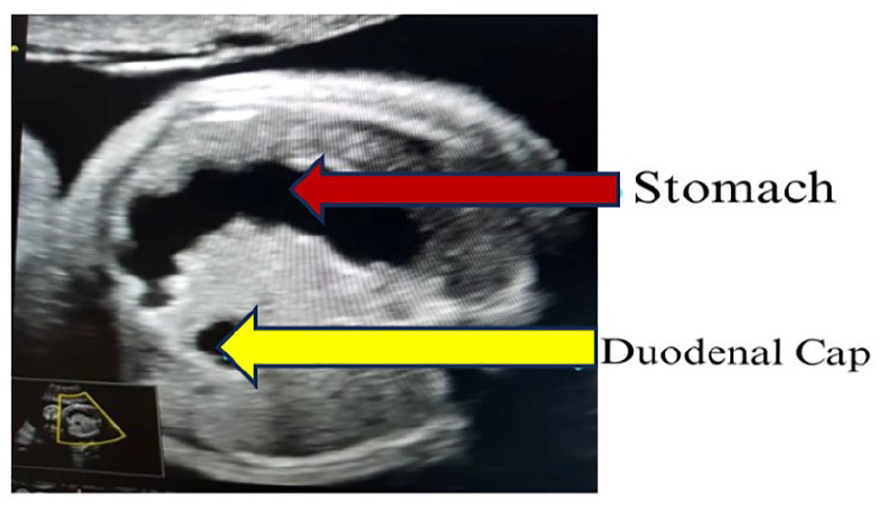
An axial section of the fetal abdomen shows the “double bubble” sign, which represents the fetal stomach and the dilated duodenal cap.
A diagnosis of bilateral fetal meromelia with DA was therefore indicated, based on the sonographic evidence. Prenatal genetic assessment was not made available in the host medical facility. The couple had extensive counseling concerning the diagnosis and postpartum care. Induction of labor was however undertaken at 28 weeks GA, due to intrauterine fetal demise, with the expulsion of a stillborn fetus, weighing 885 grams. Bilateral meromelia (see Figure 4), and DA were confirmed, on postmortem examination.

The photograph of the stillborn infant with direct evidence of bilateral meromelia.
Discussion
Congenital upper limb abnormality may result from malformations, deformations, or vascular disruptions such as the subclavian artery disruption sequence. 6 They are mostly sporadic and to a lesser extent occur in association with other skeletal, or nonskeletal malformations, as noted in this case. Development of the upper limb begins in the fourth week in utero, at which time, this process is vulnerable to disruptions that may result in developmental arrests at any level. 2 Based on the Frantz and O’Rahilly system, CULA may range from amelia, which is the complete absence of the limb, to various partial limb involvements such as hemimelia (absence of forearm and hand), acheiria absence of the hand, adactylia (absence of the metacarpals and phalanges), and aphalangia (absence of phalanges).7,8 The index case, a below-elbow meromelia, otherwise called terminal transverse hemimelia, which is the most common variant of CULA. 8 The case is peculiar, as there has been sparse reporting of a combination of meromelia and DA, in the literature, despite an extensive search.
Meromelia may occur as part of a syndrome, such as the Cornelia de Lange syndrome, Trisomy 18 (Edward’s syndrome), thrombocytopenia-absent-radius (TAR) syndrome, Trisomy 13 (Patau’s syndrome), Poland syndrome, or the Fetal hydantoin syndrome.8,9 Gestational age-dependent limb abnormalities have also been reported following chorionic villous sampling. 10
Duodenal atresia is an abnormality of the foregut due to suboptimal endodermal proliferation or a failure of the solid epithelial cord to recanalize 6 . It may occur in isolation or in combination with other anomalies such as the VACTERL association. Choudry et al reported that 57% of prenatally diagnosed DA were associated with other abnormalities. 10 Duodenal atresia may also occur as a component of a chromosomal anomaly, especially Trisomy 21. 11
With an incidence of 1–2/10 000 live births, DA is more commonly seen than CULA, and therefore more likely to be diagnosed. The characteristic “double bubble” sign also makes the sonographic recognition of DA more likely; though differential diagnoses such as jejunal atresia, ileal atresia, and abdominal duplication cysts should also be considered. 12 Duodenal atresia is associated with polyhydramnios; a large-for-date uterus may therefore be the trigger for detailed fetal evaluation, as in the index case.
Following the suspicion of any fetal limb abnormality, it is essential to measure the entire length, bilaterally, of all fetal long bones with sonography. Thereafter, measurement of the diaphyseal lengths of all the bones should be undertaken and compared with normative reference centiles, for the individual bones. Beyond the measurements however, it is also important to assess for echogenicity, fracture lines, and evidence of long-term attempts at healing of old fracture sites on the bones. In this instance, the missing distal segment of the ulna bone, and the completely missing radial bones, as further confirmed on 3D skeletal rendering, facilitated the recognition of meromelia. The 4D sonogram also demonstrated restriction of movement across the elbow joints. A magnetic resonance imaging (MRI) study may provide additional information for prenatal diagnosis of meromelia. The use of sonography is more cost-effective, with the additional benefit of assessing motion across the affected joints.
Only about 60% of newborns with CULA may survive the neonatal period. Postpartum imaging and vascular enumeration are indicated for such newborns, to plan treatment and to determine the appropriate prosthesis to improve aesthetics and functions. Some prostheses may however require serial revision due to lengthening of the residual limb in surviving children. Physical rehabilitation and occupational therapy are essential components of their care as well. Irrespective of the clinical outcomes, attention should be paid to the psychologic needs and mental wellness of expectant parents.
Conclusion
Prenatal diagnosis of meromelia is often missed, due to the rarity of the condition. The coexistence of DA makes this case report unique, as meromelia is not commonly noted with nonskeletal abnormalities. Proficiency in sonographic documentation is essential to provide an accurate prenatal diagnosis. In addition, a multidisciplinary team of medical professionals, as well as counseling are crucial for optimal management of an affected pregnancy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was not sought for this study because the case study was anonymized. Appropriate measures were taken to ensure the rights of the patient were preserved.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).