
Abstract
The use of assisted reproductive technology, specifically in vitro fertilization, has been shown to increase the risk for the fetus having a congenital malformation as compared with a fetus conceived naturally. Congenital malformations can be effectively diagnosed prenatally through the use of sonography and fetal echocardiography. This case study presents the sonographic prenatal detection of a vascular ring in the heart of a fetus conceived through in vitro fertilization. A right aortic arch with a left ductus arteriosus was identified in the three-vessel view during a detailed fetal echocardiogram. The use of prenatal sonography, specifically fetal echocardiography, led to the accurate diagnosis and appropriate treatment for the fetus.
Keywords
During fetal development, the aorta is formed through a series of arches that later regress leaving just the aorta. When the arches regress abnormally, they form congenital abnormalities such as a vascular ring. A vascular ring occurs when the aortic arch and its branches form around the esophagus and trachea instead of in front of it.1-3 This can cause severe obstruction of the airway. There are several variants of vascular rings, with the two most common presentations being a right-sided aortic arch with a left ductus arteriosus and with the other consisting of a persistent double aortic arch.1-5 A right aortic arch is formed when there is an aberrant left subclavian artery that originates from the descending aorta. The left subclavian artery has a left ductus arteriosus coming from its base, which joins the pulmonary artery in the front, forming a vascular ring around the esophagus and trachea. Aortic arch anomalies are known to be associated with chromosomal abnormalities and congenital heart defects. 6 This congenital abnormality cannot be detected prenatally with a four-chamber heart view,1,2,4,5 which highlights the importance of obtaining additional heart views during prenatal sonograms. A case is presented below of a fetus with a vascular ring abnormality. The need for the implementation of additional heart views during routine prenatal sonograms is discussed, as is the need for fetal echocardiography to be performed in high-risk pregnancies.
Case Report
A 33-year-old presented to a high-risk maternal-fetal medicine facility for a comprehensive fetal anatomy sonogram and fetal echocardiogram. The estimated gestational age of the fetus was 22 weeks 0 days based on the patient’s estimated due date. A curvilinear transducer with a frequency of 5 MHz was used on a Philips iU22 ultrasound machine (Philips Ultrasound, Bothell, WA).
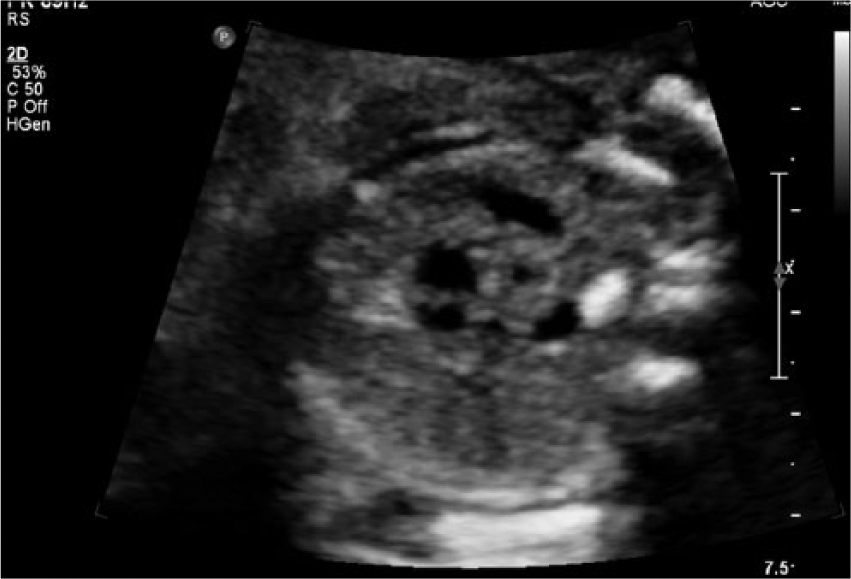
The comprehensive fetal anatomy sonogram showed that the fetus measured in the 35th percentile for gestational age. The abdominal circumference, femur length, head circumference, and biparietal diameter measurements suggested a gestational age of 21 weeks 0 days, which indicated that the fetus had a below-average percentile in growth. All the fetal anatomy appeared normal, despite measuring slightly small for gestational age, with the exception of the heart. A transverse view of the fetal heart four-chamber view showed no significant abnormalities and demonstrated a normal left ventricular outflow tract (Figures 1 and 2). The right ventricular outflow tract was imaged in the transverse plane and showed an increased space between the pulmonary artery and aorta (Figure 3). The three-vessel view showed the vessels wrapping around the trachea (Figure 4). Color Doppler imaging provided further detail and confirmed the presence of vessels wrapping around the trachea (Figure 5); the connection of blood flow surrounding the trachea was clearly imaged (Figure 6). For comparison, a normal three-vessel view of an unaffected fetus with color Doppler imaging (Figure 7) and a normal three-vessel/trachea view without color Doppler imaging (Figure 8) are shown.

Fetal sonogram in transverse showing the conventional four-chamber view of the heart with no visible abnormality.

Fetal sonogram in transverse showing the left ventricular outflow tract, which also is normal in appearance.

Fetal sonogram in transverse showing the right ventricular outflow tract, which shows the increased space between the pulmonary artery and aorta (arrow).
Fetal sonogram showing the three-vessel view in gray-scale with vessels visualized encircling the trachea.
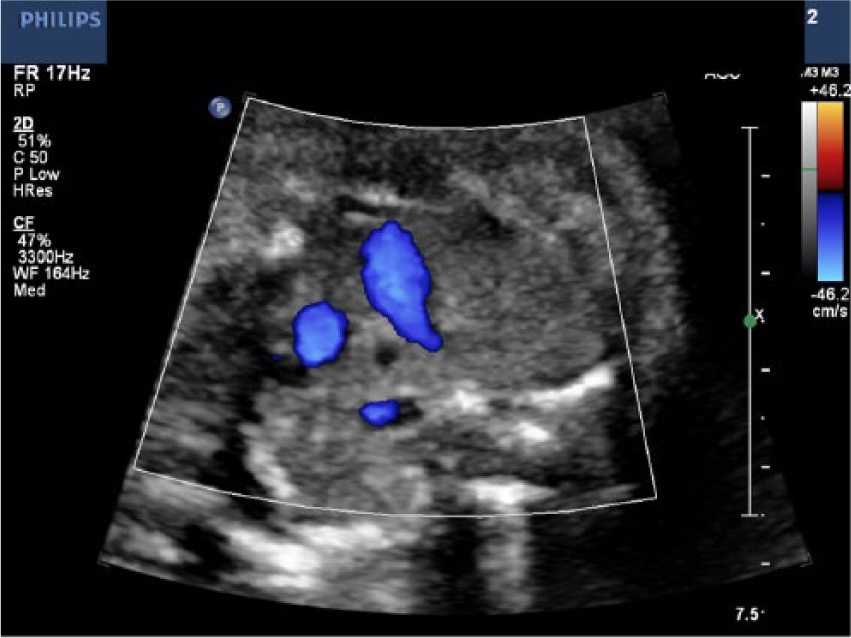
Color Doppler fetal sonographic image showing the three-vessel view, which visualizes the presence of blood flow around the trachea.
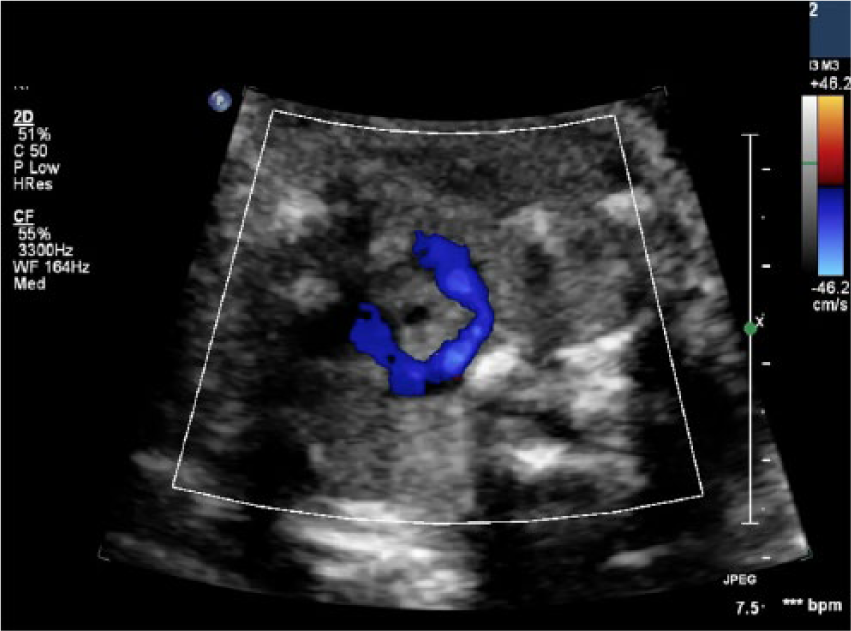
Color Doppler fetal sonographic image showing the full connection of the blood flow surrounding the trachea, consistent with a vascular ring.
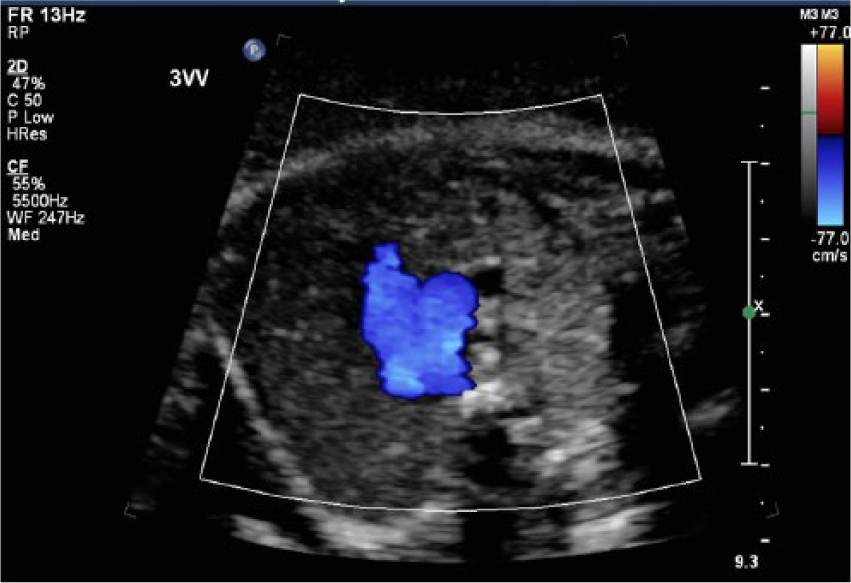

For comparison, a gray-scale fetal sonographic image showing the normal three-vessel/trachea view of a non–in vitro fertilization fetus (compare with Figure 4).
On the basis of the sonographic findings, the fetus was diagnosed with a vascular ring. The patient was sent directly to a fetal cardiac specialist, who immediately confirmed that the right aortic arch defect was present. Unfortunately, no additional follow-up information was available for this patient after management was transferred to the fetal cardiac specialist.
Discussion
The patient in this case was being seen at a high-risk maternal-fetal medicine facility because she had undergone in vitro fertilization (IVF) to conceive. A fetus conceived through IVF carries an increased risk of 41% for congenital malformations as compared with a non-IVF fetus. 7 Because of the increased risk of possible congenital malformations in an IVF fetus, including heart abnormalities, the examination protocol of the facility required a fetal echocardiogram to be done between 18 and 22 weeks of gestational age. The American Institute of Ultrasound in Medicine has defined fetal echocardiography as a “detailed sonographic evaluation that is able to identify and characterize fetal heart anomalies before birth.” 8 The American Heart Association has consolidated multiorganizational guidelines on what the basic fetal cardiac screening guidelines should be, in the publication “Diagnosis and Treatment of Fetal Cardiac Disease: A Scientific Statement From the American Heart Association.” 9 Most of these organizations agree that the criteria for gray-scale imaging in a fetal echocardiogram should include the following: four-chamber view, left and right ventricular outflow tracts, three-vessel and trachea view, short and long axis views of outflow tracts, aortic arch view, ductal arch view, superior vena cava views, and inferior vena cava views. 9 Of note, without the use of these additional fetal heart views in the patient presented, the vascular ring abnormality may have gone undiagnosed. This case provides compelling support for the implementation of additional heart views during routine prenatal sonograms, as well as the need for fetal echocardiography to be performed in high-risk pregnancies.
Diagnostic imaging, specifically sonography, is able to detect congenital heart abnormalities and give accurate classifications of each defect. Vascular rings may form in isolation or be associated with other congenital heart defects. There are two types of vascular rings. The first type consists of a right-sided aortic arch with an aberrant left subclavian artery and a left ductus arteriosus, as presented in this case. The second and more common type of vascular ring consists of a persistent double aortic arch,10,11 which has different forms in which both arches may be patent or atretic.10-12 If the arches are patent, the following may present: the right or left arch may be larger; a cervical arch may appear on either side; the thoracic aorta may have variable laterality; coarctation of the major arch may occur; or there may be discontinuity of the central pulmonary arteries. 12 For the most part, the apex of the right-sided arch will be more superior than the left arch.
Very few cases of prenatal detection and diagnosis of vascular rings have been documented in obstetric literature. A study reported by Patel et al. reviewed eight patients who had been prenatally diagnosed with vascular rings. 6 Four of these patients had a right aortic arch with an aberrant left subclavian artery and left ductus arteriosus, and the other four had a double aortic arch. In all eight cases, the vascular ring was identified similarly to the case presented, by cephalad transducer sweeps from a three-vessel view with and without color Doppler imaging. A fetus affected with either type of vascular ring will present after birth with feeding difficulties and respiratory distress. Associated with both forms is the genetic abnormality 22q11.2 deletion (near the middle of chromosome 22 at the location designated q11.2), otherwise known as DiGeorge syndrome. 13 Patients with DiGeorge syndrome can have a range of common signs and symptoms, which places the fetus at risk for neurodevelopmental delays, structural abnormalities, speech difficulties, cleft lip/palate, and increased risk for infection. Clinical outcomes from the series of eight patients ranged from surgical division of the vascular ring, elective vascular ring resection, and two patients with no intervention remaining asymptomatic up to 3 years. 6
Treatment for patients diagnosed with vascular rings varies, as the severity of this congenital heart malformation varies. Surgical repair will depend on the clinical presentation and, in most cases, is required as soon as possible on children who present with symptoms. 12 Surgery includes splitting the vascular ring through a small surgical incision on the left side of the chest between the ribs relieve pressure on the surrounding structures. The child may suffer from digestive issues due to increased restriction on the esophagus/trachea, which likely will alter the child’s diet to relieve discomfort. In other cases, careful observation of infants after birth may be done to see whether they present with any symptoms. The pressure of a vascular ring will vary from patient to patient, and surgery will be required only if the pressure is great enough. If surgery is performed, it normally relieves the symptoms. Respiratory issues may continue but decrease with time. 12 If surgery is not performed when needed, the patient may suffer serious damage to the trachea or even death.
Conclusion
The use of prenatal sonography, specifically fetal echocardiography, is the primary diagnostic imaging modality used in the detection of vascular rings. Following the American Institute of Ultrasound in Medicine guidelines 8 and the American Heart Association recommendations 9 for detailed fetal echocardiography can provide adequate documentation regarding congenital heart malformations that can lead to accurate diagnosis and treatment of such anomalies. Because vascular rings are not diagnosed from the routine four-chamber view of the heart, obtaining the additional views of the heart as suggested by the guidelines is vital in the detection and diagnosis of vascular rings. These detailed sonographic views allow for the ability to identify the relationship of the different arches in respect to the trachea, providing further information to allow appropriate preparation for treatment of the fetus upon delivery.
Footnotes
Acknowledgements
I thank Jessica Gamm, RDMS, RVT, BHS, and Cathy Arnold, RDMS, FE, for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.