
Abstract
A single umbilical artery (SUA) is one of the most common malformations in a fetus, with approximately a 1% occurrence rate. A retrospective study of 108 fetuses with a SUA was done to determine if the laterality of the SUA made a difference in fetal prognosis. An absent right umbilical artery was found in 42 (38.9%) of cases and an absent left umbilical artery in 66 (61.1%) cases. When correlated with fetal outcome, there was a closer association between an absent right umbilical artery with genitourinary anomalies, cardiac defects, and chromosomal abnormalities. There was a nine times greater likelihood (95% confidence interval of a 3 to 27 times greater probability) of a fetal anomaly with an absent right umbilical artery than with an absent left umbilical artery.
Keywords
Introduction
The existence of a single umbilical artery (SUA) cord was first described during the Renaissance era by Fallopia and Bahuin, 1 yet its association with aneuploidy or fetal anomalies was not reported until the mid-twentieth century. 2 Prenatal detection of a SUA was first identified using sonography by Jeanty in 1989.1,3 Significant advancements in the field of sonography have been made since Jeanty’s discovery; however, poor early antenatal detection of a SUA still remains.4–6
Multiple studies over the years have shown there is a significant increase (seven times greater) of fetal anomalies, growth restriction, mortality/morbidity, and chromosome abnormalities with a single umbilical artery, yet its early detection rate is far from adequate.7–10 Only a few studies were identified that described the siding of the SUA and its associated findings.1,2,11–13 Most of these studies were conducted before the year 2000, and many had inadequate sample sizes or incomplete sonographic evaluation.1,2,11,13 Several fetopathological studies have shown that early prenatal detection of a SUA by sonography was only 21% to 36% when compared to specimens from elective or spontaneously aborted fetuses.1,4–6 Several live birth studies were conducted during the 1990s that demonstrated sonography’s early prenatal detection accuracy rate was approximately 65%. This accuracy rate increased to 85% when the sonogram was performed between 17 and 36 weeks gestation.1,2,4,13,14 The early antenatal detection of a SUA plays a vital role in directing fetal management as well as providing an aid in maternal counseling and follow-up. 5 The goal of this study was to determine if the laterality of a SUA makes a difference in fetal prognosis as well.
Materials and Methods
A retrospective study was performed to help answer the specific question: In the fetus that has a single umbilical artery, will the absence of a right umbilical artery be a better prognostic indicator for congenital heart disease, genitourinary anomalies, and/or chromosomal abnormalities than the absence of a left umbilical artery? Institutional IRB approval was obtained prior to data collection. All gravid patients who were referred to a facility in the Western United States from January 2009 to July 2013 were evaluated. Only those fetuses that were sonographically determined to have a single umbilical artery were included. The exception to the inclusion criteria were fetuses with a gestational age less than or equal to 11 weeks and 0 days and those greater than or equal to 41 weeks and 0 days. All sonograms were performed by ARDMS OB credentialed sonographers using a Philips IU22 (Bothell, Washington) ultrasound machine with a C5-1 curved linear array transducer. Data and images were extrapolated from institutional electronic medical records and sonographic databases.
Clinical information was extracted from the patients’ electronic medical records, and the covariates of body mass index (BMI), diabetes mellitus, and maternal age were recorded. Gestational age at the time of the sonogram was also recorded to ensure the inclusion criterion was met. A key was made to de-identify all patient health information with a coded sequential numerical value. The siding of the SUA, the presence of any fetal abnormality(s), singleton versus multiple gestation, and any chromosomal testing that was performed were also recorded on the data sheet.
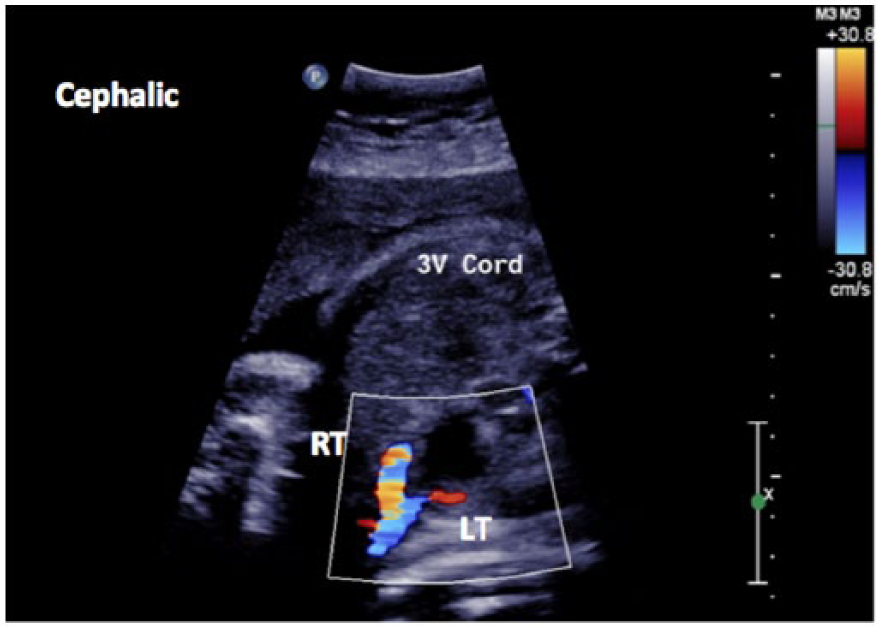
The imaging protocol used to determine the presence of a SUA was the transverse plane where the umbilical arteries are seen lateral to the fetal bladder (Figures 1 and 2). To determine correct SUA sidedness, the fetal position and situs were imaged and evaluated for accuracy. Upon review, if sidedness was determined to be inaccurate or inconclusive, the patient was excluded from the study.
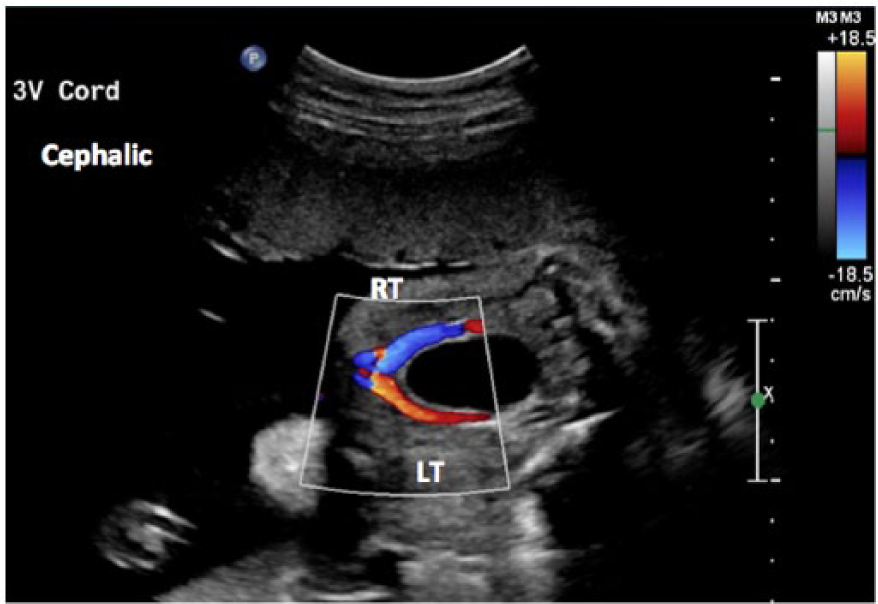
Color Doppler image correctly demonstrating a three-vessel umbilical cord lateral to the bladder.
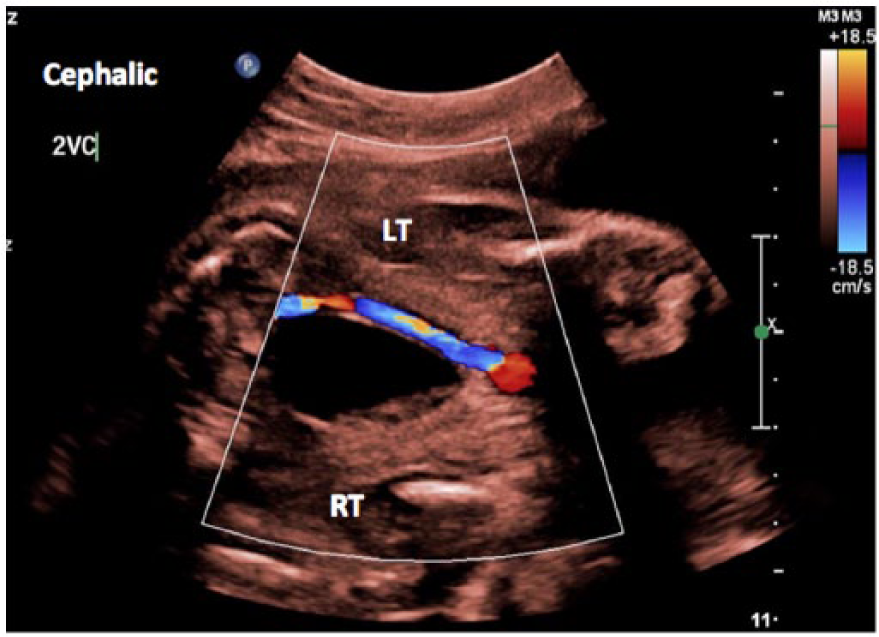
Color Doppler image (with B-mode tint) of a two-vessel cord at 30 weeks gestational age.
A multi-way cross-tabulation was constructed to display the observed frequencies of absent left vs right umbilical arteries and their observed frequencies of congenital heart disease, genitourinary abnormalities, and chromosomal anomalies. The cross-tabulation was analyzed by log-linear modeling and multiple correspondence analysis, accepted statistical methods to explore the associations between nominal variables in epidemiological studies.15,16
A significant association has been established between maternal obesity and increased risk of congenital fetal malformations. 17 Furthermore, the image quality of fetal structures is deleteriously affected by excessive abdominal fat, causing marked attenuation of the signal, which tends to be weaker in obese pregnant women because of the absorption, reflection, and scatter of the ultrasound waves. 18 It was not, however, possible to control for maternal obesity as a potentially confounding covariate in this study because after decomposing the multi-way cross-tabulation by maternal BMI (above and below 30 kg/m2), the cell frequencies were too low to conduct accurate statistical analysis.
Without controlling for obesity, the statistical assumption that the total sample size should be greater than five times the number of cells in the multi-way cross-tabulation (5 × 16 = 80) was satisfied; however, the assumption that the expected frequencies in every cell should be >0 was violated. The strategy of adding a delta factor of 1 to each cell was applied to avoid zero expected frequencies; however, this transformation may reduce statistical power, implying that although type I errors may be decreased, type II errors may be increased. 19
The strategy of collapsing the multi-way table into a two-way table was also applied, so that none of the cells contained frequencies <5. The odds ratio (OR) was computed from this two-way table to indicate the likelihood of observing a combination of defects in fetuses with an absent right artery relative to fetuses with an absent left artery; however, the OR did not approximate the relative risk of observing multiple defects because the data were not based on a randomized controlled trial or a cohort study, and the proportion of observed defective fetuses in the sample was >1%. 20
Results
A total of 108 fetuses with a single umbilical artery was observed in patients ranging in maternal age from 15 to 46 years, of which 36 (33.3%) were less than 25 years old, 54 (50.0%) were between 25 and 34 years old, and 18 (16.7%) were over 35 years old. The BMI of the gravid patients ranged from 20 to 51 kg/m2. About half (47.2%) of these patients were classified as obese (BMI ≥30 kg/m2). Fetal defects were not observed in two of the six patients who were diagnosed with diabetes mellitus.
Table 1 displays the multi-way cross-tabulation of the observed frequencies of absent left vs right umbilical arteries and their observed frequencies of the three categories of fetal defects. No defects were observed in 85 of 108 (78.7%) of the fetuses. A total of 23 fetal defects were observed, of which 10 of 23 (43.5%) were in obese gravid patients and 13 of 23 (56.5%) were in patients less than 25 years old. Of these fetal defects, 5 of 23 (21.7%) were isolated chromosomal abnormalities among a total of 66 fetuses (7.6%) with an absent left umbilical artery, while 18 of 23 (78.3%) were a combination of chromosomal abnormalities, genitourinary abnormalities, and/or chromosomal anomalies among a total of 42 fetuses (42.9%) with an absent right umbilical artery.
Multi-Way Cross-Tabulation of the Observed Frequencies of the Absence (–) or Presence (+) of Congenital Heart Disease, Genitourinary Abnormalities and Chromosomal Anomalies in Fetuses With Absent Left or Right Umbilical Arteries.
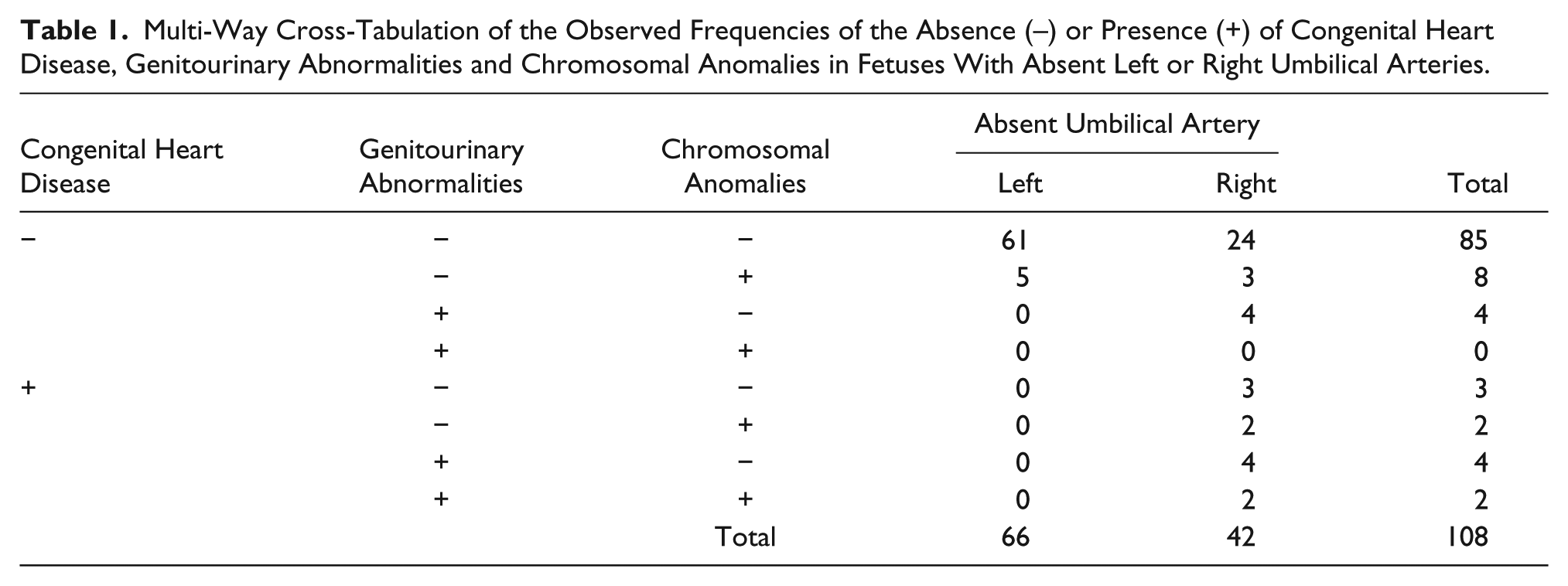
Based on the analysis of the two-way cross-tabulation (18/5)/(24/61), the OR = 9.2 (95% CI, 3.1–27.4). The OR implied that on average, the likelihood of observing a defect was about nine times higher in fetuses with an absent right umbilical artery relative to fetuses with an absent left umbilical artery. The 95% CI inferred that if 100 fetuses were observed, the likelihood of observing defects in 95 fetuses with absent right umbilical arteries would be about 3 to 27 times higher than observing defects in fetuses with absent left umbilical arteries.
A parsimonious log-linear model was extracted from the multi-way cross-tabulation after backward elimination of nonsignificant categories. The likelihood ratio (χ2 = 1.05, P = .994) indicated that this parsimonious model was not significantly different from the saturated model, implying that it was a good fit to the cross-tabulation. Significant two-way effects at α = 0.05 were identified between (1) the absence of the right umbilical artery and the presence of genitourinary abnormalities (10 fetuses; χ2 = 9.49, P = .002), (2) the absence of the right umbilical artery and the presence of congenital heart disease (11 fetuses; χ2 = 11.76, P = .001), (3) the conjoint presence of genitourinary abnormalities and congenital heart disease (6 fetuses; χ2 = 7.11, P = .008), and (4) the conjoint presence of chromosomal abnormalities and congenital heart disease (4 fetuses; χ2 = 5.68, P = .017). No statistically significant three-way or four-way effects were found.
The odds ratio and log-linear model only indicated that there was a significant probability of systematic associations between the absence of the right umbilical artery and the presence of multiple fetal defects; however, these methods did not reflect the structural patterns of the associations. A multiple correspondence map is therefore presented to illustrate these patterns (Figure 3). A window is opened to visualize the strengths of the associations between eight nominal categories in a two-dimensional graphical representation. The geometric orientation of the points across the two constructed axes (correspondence components) reflected the relative similarities of the categories. The more closely aggregated were the points, then the more closely correlated were the categories.
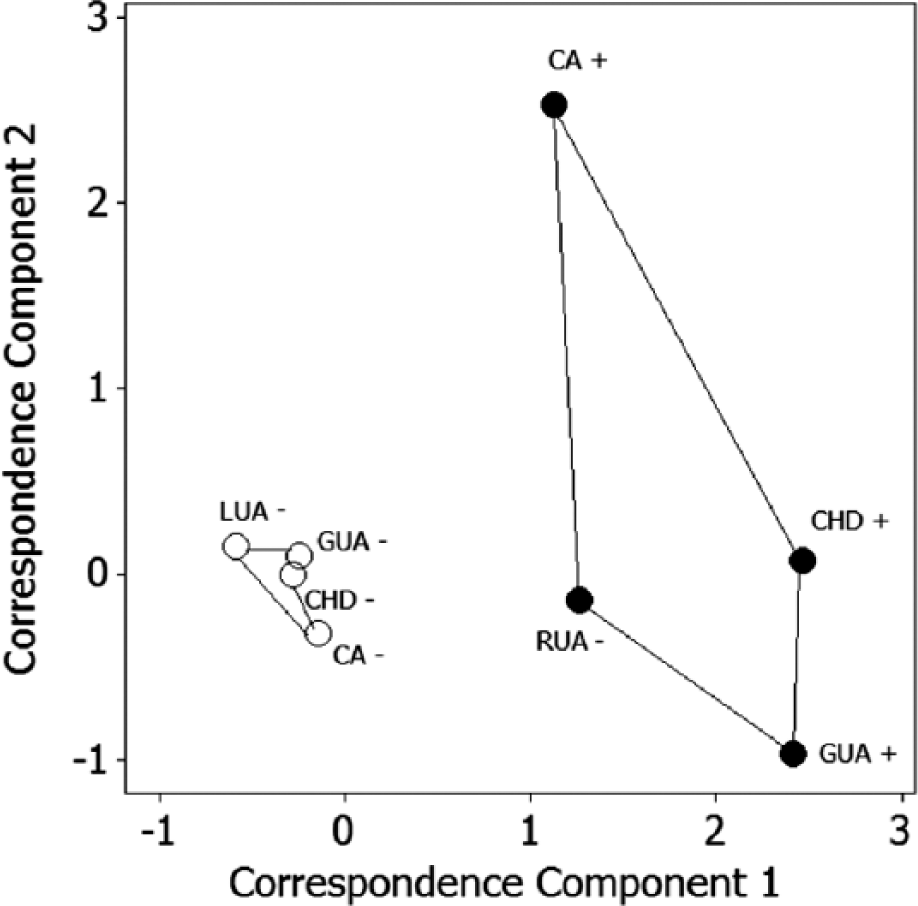
Multiple correspondence map of the associations between the presence or absence of congenital heart disease, chromosomal abnormalities, and genitourinary abnormalities in fetuses with absent right or left umbilical artery. CA, chromosomal abnormalities; CHD, congenital heart disease; GUA, genitourinary abnormalities; LUA, left umbilical artery; RUA, right umbilical artery; +, present; –, absent.
The validity of the correspondence model was reflected by the two components collectively explaining 73.4% of the variance in the data. Two clusters of points could be clearly distinguished. The points corresponding to the absence of the right umbilical artery and the presence of congenital heart disease, genitourinary abnormalities, and chromosomal anomalies were clustered broadly on the right hand side of the plot, on the positive axis of component 1, spreading across the negative and positive axes of component 2, reflecting their relatively loose association. The points corresponding to the absence of the left umbilical artery and the absence of congenital heart disease, genitourinary abnormalities, and chromosomal anomalies were clustered adjacent to each other, on the negative axis of component 1, near the pole of component 2, reflecting their relatively closer association.
These data suggest that statistical significant evidence exists to infer that among the retrospective sample of 108 fetuses observed with a single umbilical artery, the absence of a right umbilical artery appeared to be a better prognostic indicator for congenital heart disease, genitourinary anomalies, and/or chromosomal abnormalities than the absence of a left umbilical artery.
Discussion
A single umbilical artery is one of the most common malformations in a fetus, with approximately a 1% occurrence rate. 7 Even with the new discoveries in embryologic pathogenesis, the etiology of a single umbilical artery continues to remain elusive. There are three standard theories that have been put forth over the years.7,21 The first theory hypothesizes that one artery never develops during the early embryologic stage (agenesis). The second and most commonly accepted theory is that in the early developmental stages two umbilical arteries are indeed present, but for an unknown reason, one regresses (atrophies), leaving only one to persist. The third theory presents the possibility of the persistence of the original allantoic artery of the body stalk. Ascertaining which umbilical artery will persist, right (Rt) or left (Lt), is just as ambiguous as its embryologic event.
The more common persistence of a single right umbilical artery has shown to hold true over time and multiple studies. Many authors believe this may be due in part to its known larger caliber when compared to the left (Figure 4).1,2,11–13,22 If that is the case, why the left would persist over the right is an even more complex question than the evolution of a single umbilical artery. A Long-Evans rat embryo study, performed by Monie in 1970, introduced specific teratogens during early cord development to see if there might be a teratogenic reason for the left remaining. The findings demonstrated that this may indeed lend credence to the persistent of a Lt SUA rather than Rt. 7 Whether the Rt or Lt umbilical artery remains, even as an isolated finding, both are associated with a high incidence of perinatal morbidity (six times greater), intrauterine growth restriction (IUGR), low birth weight, prematurity, and more frequent delivery by cesarean section. 12 If additional anomalies are also found with a SUA, this increases the risk of chromosomal abnormalities (aneuploidy) to approximately 10%. 21 Some feel the answer for such poor perinatal outcomes may indeed lie within the coiling of the cord itself, its decrease in diameter, and the decrease in its protective layer, Wharton’s jelly, rather than the siding of the SUA.8,12,23–25
Color Doppler image of a three-vessel cord showing an example of a larger right umbilical artery.
The natural occurring helical coiling of the umbilical cord contributes to its strength, toughness, and stiffness (Figure 5). A normal cord coiling should have approximately 0.17 to 0.41 coils/cm, which is known as the umbilical coiling index (UCI).24,25 Sonographically, the UCI can be determined by measuring the length of one complete coil taken at mid cord. Dividing 1 by that length equals the UCI. A cord, whether two or three vessels, with a lower UCI (<0.17 coils/cm), known as hypocoiled, has a decreased ability to handle stress. This puts the fetus at risk for intrauterine fetal demise (IUFD), congenital anomalies, velamentous cord insertion, acute reduction of blood flow due to kinking, decreased fetal growth, low birth weight (<10th percentile), prematurity, perinatal morbidity, and reduced Apgar scores at birth.24,25 The single umbilical artery generally coils less around the umbilical vein than if two arteries are present (Figure 6).8,12 The umbilical cord diameter, as well as the thickness and presence of Wharton’s jelly, also contribute to its toughness to handle stress. Both increase with advancing gestational age well into the third trimester, when the diameter levels off and the Wharton’s jelly decreases. 8 Cord pathological specimens have shown a decrease in the diameter and Wharton’s jelly of the two-vessel cord (2VC) throughout all gestational ages, which has been speculated to be the leading causative factors contributing to cord torsion, resulting ultimately in fetal demise. 26

Gray-scale image showing normal helical coiling of an umbilical cord. The Umbilical Coiling Index (UCI) = 0.35 (1/2.83) (normal UCI = 0.17–0.41).

Gray-scale image showing a hypocoiled two-vessel cord; no coils can be seen along this segment.
The early diagnosis of a SUA by sonography plays a major role in determining management of the fetus as well as an aid in maternal counseling and follow-up. This detection rate must improve if better outcomes are to be generated, which in turn will propagate significant research. As noted by Gornall et al. 5 in 2003 and Abu-Rustum et al. 27 in 2010, the poor antenatal detection rate indicates that further training of sonographers is needed, along with raising the awareness of the implications of finding a SUA., With proper settings on advanced ultrasound equipment and proper training of sonographers, the 3VC or 2VC can be seen on almost all patients during the first trimester, regardless of habitus. Since this protocol has been implemented in our facility, there have only been a few fetuses where the number of cord vessels were indeterminate or could not be visualized. When verifying the cord vessels during the follow-up second trimester sonogram, only one false positive SUA was noted. Of the 108 patients imaged, 51 (47.2%) met the criteria for obesity (BMI ≥30 kg/m2), with 12/51 (23.5%) meeting the criteria for morbid obesity (BMI ≥40 kg/m2), one of which exceeded 50 kg/m2 BMI. Our study demonstrates that educating sonographers to properly adjust machine settings, including color and spectral Doppler, to obtain the number of cord vessels in a first trimester examination is possible, and indeed warranted, even on a difficult habitus.
A more detailed sonographic evaluation should be given at the time of the nuchal translucency (NT) sonogram during the first trimester. To ensure the most accurate results are obtained, qualified personnel in obstetrics (OB) should be performing this important diagnostic sonogram. Without exception, the ultrasound machine must have color and power Doppler capabilities. The protocol images should include but not be limited to the situs picture and the 3VC view in succession. The situs picture should be side-by-side images of the transverse thorax and transverse abdomen, labeling fetal position, anatomy seen (i.e., stomach, heart), and appropriate right and left side (Figure 7). The next image should be of the 3VC view using power Doppler, as this type of Doppler is more sensitive to low flow states and is not dependent on direction. The image should demonstrate the umbilical arteries coursing laterally to the transverse bladder, again labeling Rt and Lt side (Figure 8). A cross-sectional view of a free-floating piece of umbilical cord should not be taken to determine a 3VC at any point in the pregnancy, as a fused umbilical artery (FUA) may be present, which is more common than a SUA and is not associated with anomalies. 28 It is essential to take the images of situs and the 3VC in succession to avoid errors and ensure proper identification of the siding, particularly if a single umbilical artery is present. These images will also aid in the diagnosis of other possible anomalies present (i.e., situs inversus, cardiac malformations, absent stomach, etc.), as seen in Figure 7, and help the patient make decisions regarding genetic counseling and further testing. In turn, this will aid the primary medical doctor (PMD) to make decisions regarding future detailed imaging, obtaining sonograms sooner rather than later.
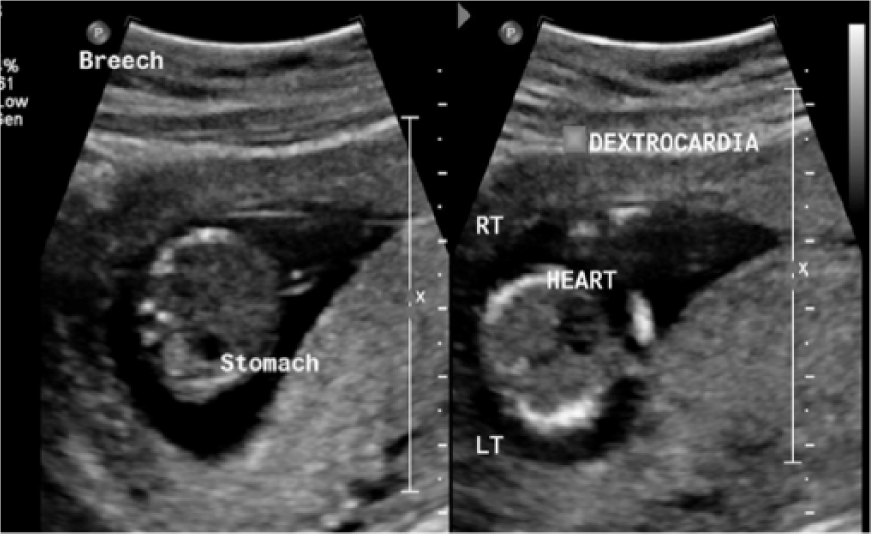
Gray-scale transverse images of the abdomen and thorax situs evaluation showing the stomach and heart at 12 weeks gestational age (with abnormal situs in this example).
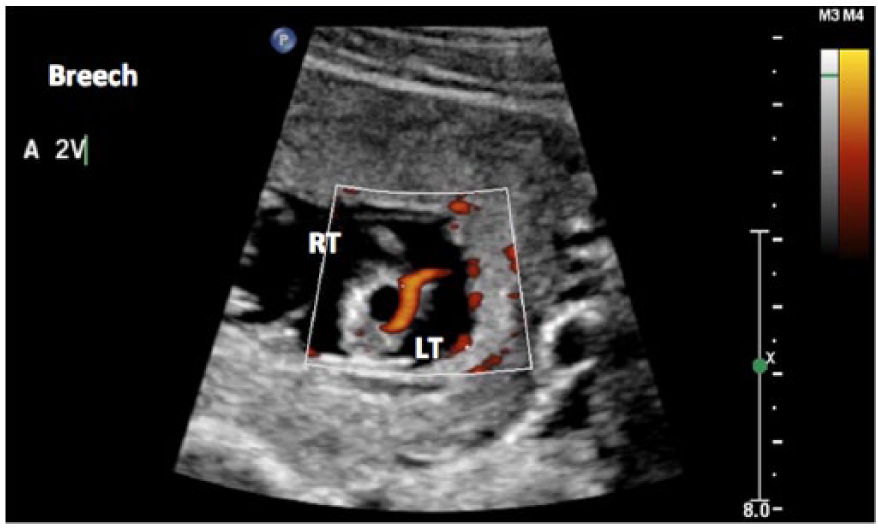
Power Doppler image of a single umbilical artery at 12 weeks gestational age.
To our knowledge, this study is the largest retrospective study done to date for determining SUA siding associated with fetal anomalies, comprising of 108 fetuses. An absent right umbilical artery was found in 42 (38.9%) of those cases and an absent left in 66 (61.1%) cases. The finding of an absent left umbilical artery occurring more frequently than an absent right agrees with prior studies done be Lubusky et al. 12 in 2007 (absent Rt, 41.2%; absent Lt, 58.8%), Geipel et al. 13 in 2000 (absent Rt, 30.4%; absent Lt, 69.6%), and Abuhamad et al. 2 in 1995 (absent Rt, 27%; absent Lt, 73%). However, unlike the aforementioned authors, our findings show that there indeed is a closer association, which is statistically significant (nine times greater), between an absent right umbilical artery with genitourinary anomalies, cardiac defects, and chromosomal abnormalities when compared to an absent left. Geipel et al., 13 Lubusky et al., 12 and Blazer et al. 11 suggested that there was no preferential siding of the absent umbilical artery with anomalies. The findings of Abuhamad et al. 2 showed that cytogenic and complex fetal anomalies occurred exclusively with an absent left umbilical artery. It is not completely certain why this discrepancy between our study’s findings and the other authors exists, but one must consider a few possibilities.
Though the studies by Fukada et al. 1 (1998), Abuhamad et al. 2 (1995), and Blazer et al. 11 (1995) produced extremely useful information, their fetal numbers were less than statistically significant for research (10, 77, and 46, respectively). It must be duly noted that those studies were performed in the 1990s, when much of ultrasound technology was still in its infancy. They did not have at their disposal the improved technology of ultrasound and color Doppler, especially in regard to tissue penetration, which exists today. Those authors did however set the stage to help answer the question not only of the association of a SUA with anomalies but if the absence of one artery was more significant.
The only exclusion to our criteria was a gestational age less than 11 weeks 0 days or greater than 41 weeks 0 days. Unlike our retrospective study, Lubusky et al. 12 (2007) preselected the patients who had a combination of maternal age, biochemical screening, and sonographic findings. His study was to answer the specific question if chromosomal defects were associated with the specific siding of a SUA. All sonograms were performed in the second trimester. No first trimester sonograms were performed in the study. One must question if the diagnosis of a SUA in the first trimester, with or without anomalies, may have changed the results of nonpreferential siding of the SUA with abnormal chromosomes or anomalies. It is important to note, however, that all chromosomal abnormal fetuses with a SUA had anomalies, as was noted in this study. With such findings, a first trimester sonogram documenting the number of cord vessels is strongly suggested, as the results may be ominous, particularly if other anomalies exist such as abnormal situs. Further counseling and decisions will then need to be considered by the patient.
Geipel et al. 13 in his prospective study from 1996 to 1998 diagnosed 102 fetuses with a SUA. Similar to our study, first trimester diagnosis was included as well as low- and high-risk pregnant women. Also similar to our study and other prior studies mentioned, Geipel et al. 13 demonstrated that all of the fetuses with chromosomal abnormalities (10) had significant anomalies. Yet unlike our study, which demonstrated a 95% CI of a 3 to 27 times greater probability of finding a defect with an absent right umbilical artery, his data suggest that there is equal distribution of anomalies between an absent right and an absent left umbilical artery. With such discrepancy to our findings, one must consider at least two possibilities. Sonographic resolution in the 1990s was not as detailed compared to the imaging systems used for this study that occurred between 2009 and 2013. This may lead one to believe that the diagnosis of the smaller left SUA may indeed have been difficult to assess in the first trimester, which could imply there may have been some missed data. Second, do environmental factors play a role in the development and siding of a single umbilical artery, as Fiddler and Pergament 29 have suggested? The Geipel et al. 13 study was performed in Germany and ours in the western United States, where almost half of our patients (47.2%) with a SUA were obese. This hypothesis may be difficult to prove but is worth consideration.
It is important to note that of the SUA fetuses with anomalies, 43.5% were seen in obese patients. This agrees quite strongly with Stothard et al. 17 (2009), who found a close association with obesity and anomalies, particularly congenital heart defects (CHD). This stresses the need of having properly trained sonographers who are adept in optimizing the machine settings for proper visualization of a SUA in difficult habitus patients in the first trimester. It is those difficult habitus patients who are at most risk for having a SUA and fetal defects. They deserve the same consideration and options as those who are at less risk yet easier to scan.
Several questions still remain to be answered. With the known smaller diameter of the left umbilical artery, and Monie’s 7 suggestion that certain teratogens introduced early on may result in eliminating the larger right umbilical artery, could it be those teratogens are the reason more fetal anomalies and a poorer perinatal outcome occur when there is an absent right umbilical artery, as our study has suggested? Do environmental issues play a role in a SUA developing? To what extent does obesity increase the likelihood of a SUA? Will we ever be able to clearly identify the cause of a SUA, whether absent right or left?
Conclusion
It is essential that the number of cord vessels, as well as the situs of the fetus, be diagnosed in the first trimester so that patients and doctors alike have the necessary information to make other important decisions, including genetic counseling and testing. If a single umbilical artery is noted, its siding should also be documented. The data from this study suggest that those fetuses that have an absent right umbilical artery are nine times greater to have other anomalies present. If the patient is obese, there is even a higher likelihood of finding anomalies. Proper equipment, training of sonographers, and thorough protocols are all key factors in making sure this diagnosis is not missed. Though our findings showed chromosome abnormalities were only associated with a SUA when other anomalies were present, genetic counseling still should be offered to all patients when an early diagnosis of a single umbilical artery is made, as some anomalies may not present until the second trimester. All patients with an absent right umbilical artery should be made aware of the greater probability of finding other anomalies, and genetic testing should be offered. All obese patients should be offered genetic counseling, a detailed sonogram, and fetal echocardiogram. They should be duly informed of the considerable likelihood of finding other anomalies. Though weight may be a sensitive topic, as medical professionals, we are obligated to be honest with all our patients, no matter what their size, and inform them of the implications their obesity plays in the outcome of their fetus.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported in part by a grant from the Sonography Research Institute of the Society of Diagnostic Medical Sonography Foundation.