
Abstract
Planar scintigraphy with 99mTc-pertechnetate or Meckel scan is the gold standard in the diagnosis of a bleeding Meckel’s diverticulum (MD) for pediatrics. However, several setbacks may occur during the interpretation of a scintigram, especially in cases of an atypical MD presentation. In this report, we highlight the importance of functional and anatomical image co-registration using a hybrid SPECT/CT scanner to precisely localize a MD lesion. An 18-month-old boy presented with severe hematochezia over 4 days with declining hemoglobin levels. He underwent a conventional 60-min dynamic planar imaging of the Meckel scan. Upon review of the Meckel scan, a suspicious increase in the 99mTc-pertechnetate uptake was observed at the right upper quadrant of the abdomen. Due to its atypical location at the right kidney, we could not differentiate between a physiological uptake of the right kidney or an ectopic gastric mucosa. The patient was imaged again using single-photon emission computed tomography (SPECT) and low-dose CT protocol with a hybrid SPECT/CT scanner, and the co-registration of both SPECT and CT images was able to confirm the MD, which was located anterior to the right kidney at the right hepatic flexure region. An exploratory laparotomy was then ensued to remove the bleeding MD. The patient was discharged after 3 days with no complications. In summary, this case illustrates that hybrid imaging modality and co-registration allow for a more definitive diagnosis, as well as a more precise localization of MD.
Introduction
Meckel’s diverticulum (MD) is a congenital gastrointestinal (GI) anomaly, with a recently reported prevalence of 0.3%–2.9% in the general population. 1 It is a remnant of the vitelline duct that is typically found on the anti-mesenteric margin of the ileum and is estimated to be located within 200 cm from the ileocecal valve. Meckel’s diverticulum is usually asymptomatic and discovered incidentally upon surgery. Statistics on lifetime risk of complications due to MD, for example, intestinal obstruction, bleeding, inflammation, and perforation were highly variable—ranging from 4%–40%.2,3 In the pediatric population, the most common complication of MD is GI tract hemorrhage.4,5 Acute major hemorrhage, anemia due to chronic bleeding, and self-limiting repeated episodes are all clinical forms of bleeding MD. The hemorrhage is believed to be caused by peptic ulcers in the ectopic gastric mucosa or, in extreme cases, by adjacent ileal ulcerations caused by acid secretion by the MD.
Planar metastable technetium-99 pertechnetate (99mTc-pertechnetate) scintigraphy, commonly referred to as Meckel scan, is regarded as the gold-standard imaging method for evaluating pediatric patients with suspected bleeding MD. The diagnostic accuracy of a Meckel scan for pediatrics was estimated to be approximately 90% and decreases with age.6,7 In a 2014 joint practice guideline published by major nuclear medicine societies, it was mentioned that planar imaging may be affected by anatomic/physiologic errors, for example, obscured diverticulum due to overlapping uptake on the small bowel, kidneys, ureters, and bladder. The use of single-photon emission computed tomography (SPECT) and hybrid SPECT/CT imaging could improve the detection of MD and the overall diagnostic accuracy, but their role remains unclear and warrants further investigations. 8
Based on the discussion above, we hereby demonstrate the practical utility of SPECT image co-registered with a low-dose CT image for a successful investigation of bleeding MD in a pediatric patient. This case report was written in adherence to the updated Surgical Care Report guidelines.
Case Report
An 18-month-old boy was referred to our institution in August 2020 due to hematochezia for 4 days. The bleeding was moderate in amount, fresh red, and not mixed with the stools. He was born full-term via emergency Caesarean section surgery due to fetal distress. Immunization was up to age. Otherwise, there was no history of fever, diarrhea, taking outside food, sick contact, water activity, traveling, or trauma. As for social history, the patient was left under the care of his grandmother as his parents had to work in a city located 336 km away from their hometown. Upon further history taking, it was revealed that the patient was introduced to a locally packaged milk product 1 week before the presentation.
Physical examination revealed his vital signs as follows: Temperature = 37°C; pulse = 160 BPM; blood pressure = 120/62 mmHg; capillary refill time = < 2 s; and weight = 8.2 kg (below third centile). He appeared well-nourished, alert, and active. Abdominal examination demonstrated a soft, non-tender, and non-distended abdomen with active bowel sounds. There was no palpable mass, and digital per rectal examination showed a well-formed anus with no evidence of hemorrhoids, abrasions, anal fissures, or abnormal lesions. The patient was then admitted under the impression of an intussusception. The differential diagnosis includes cow’s milk protein allergy, MD, and colitis.
In the ward, the hemoglobin level was noted to be decreasing in trend (11.3 > 10.7 > 9.1 g/dL). Other investigations were within the normal range. Plain radiographs and ultrasound findings showed normal bowel peristalsis, no free-fluid, no dilated bowel loops, no free peritoneal air, and no evidence of bowel intussusception. At this point, the patient’s parents were notified of his condition and were skeptical about undergoing an exploratory surgery without a confirmed diagnosis. A Meckel scan was then ordered to rule out the possibility of a bleeding MD. The surgical team was also notified for emergency surgery if the hematochezia worsens, in view of arteriovenous malformations.
Upon arrival to the imaging suite, the patient was injected intravenously with 99mTc-pertechnetate (29.97 MBq; 0.81 mCi) for planar scintigraphy. The imaging field was set to the anterior abdominal view (stomach to sub-pubic) and dynamically imaged at 60 frames/second, up to 1 h. The serial images demonstrated a stable focal radiotracer uptake at the right abdominal upper quadrant, which was seen in congruence with the normal physiologic activity of the stomach organ and increased in intensity over time [Figure 1]. However, because of its proximity near to the kidney level, we could not confidently determine whether it was caused by the normal excretion of 99mTc-pertechnetate to the right kidney or by an ectopic gastric mucosa. Given this, he was subjected to a SPECT/CT imaging with a low-dose, non-diagnostic, and non-contrast CT protocol for pediatrics (helical acquisition, tube voltage = 80 kV; and smart modulating mA = 30 mA–80 mA with 50% reduction), using a hybrid SPECT/CT scanner system. Based on the co-registration of both SPECT and CT images, we found that the uptake was compatible with ectopic gastric mucosa anterior to the right kidney, located at the right hepatic flexure [Figure 2]. Hence, the diagnosis of an MD was confirmed and pediatric surgery was consulted. Planar Meckel scan at (a) 5 min, (b), 20 min, and (c) 60 min after intravenous administration of 99mTc-pertechnetate. Images showed one focal at the right upper quadrant of the abdominal region. Hybrid SPECT/CT Meckel scan of (a) CT component, (b), SPECT component, and (c) SPECT/CT-fused image in trans-axial view. The final co-registered image showed the exact location of Meckel’s diverticulum anterior to the right kidney.

After studying the SPECT/CT images, the pediatric surgeon decided to perform an exploratory laparotomy. The surgical evaluation revealed a blind pouch MD at the anti-mesenteric border of the ileum; thus, Meckel’s resection and end-to-end anastomosis were made. Gross histopathology report revealed MD with no visible perforation and hemorrhage. Microscopic findings confirm the presence of heterotopic gastric mucosa with no significant increase in inflammatory infiltrates, ulceration, muscular layer disruption, dysplasia, and no malignancy [Figure 3]. Postoperatively, his vital signs were stable. He was also able to pass stool without blood and there were no episodes of vomiting. The patient was then discharged with syrup cefuroxime and paracetamol after 3 days.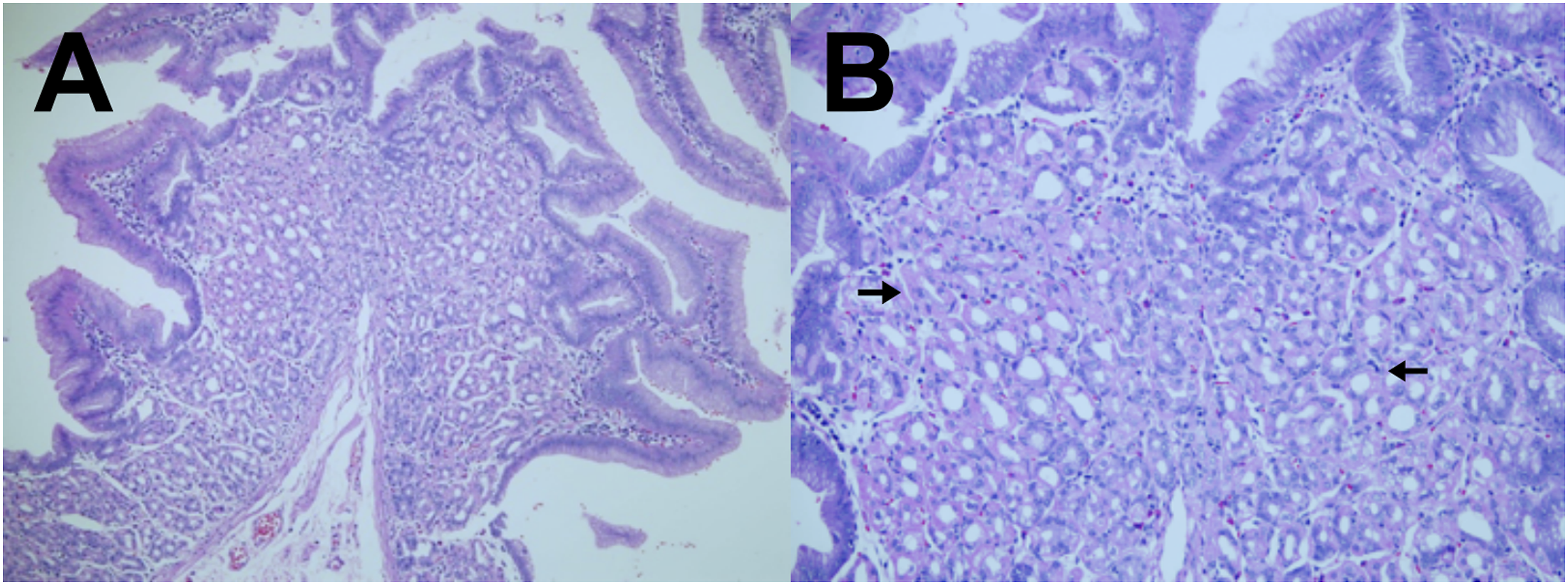
Discussion
The Meckel scan is well-known for its relatively quick execution, simple radiotracer preparation, and high diagnostic accuracy. Meckel’s diverticulum is presented in scintigrams as a focus with elevated 99mTc-pertechnetate activity, typically seen at the right lower quadrant of the abdomen.1,9 While the above description is compatible with most MD cases, there is still a high chance of ignoring an atypical presentation. In a retrospective cohort of 93 patients with positive Meckel scan and complete surgical record, it was discovered that 10.8% of MD patients have an atypical scintigram, whereby the lesion is located at the right abdominal upper quadrant. 9 An atypical planar Meckel scan image is generally more difficult to interpret because it could overlap with other organs and structures with normal physiological uptake patterns. 8 In children, the blood disappearance rate of radioactive pertechnetate could be prolonged due to renal immaturity. 10 Uptake seen in this region could also be due to urinary obstruction or vascular anomalies adjacent to the bowel loops. If present, these occurrences may mimic pathological uptake and serve as a diagnostic dilemma to many nuclear medicine physicians and radiologists in reporting to their surgical colleagues—especially in bleeding MD as it requires immediate attention and careful surgical planning.
The role of SPECT/CT imaging in improving the interpretability of an atypical Meckel scan, despite increasing in the medical literature, still requires more clarification as it is mostly available in case reports and lacks in prospective studies.1,8,11–13 The CT scanner found in a hybrid SPECT/CT system is not suitable in providing a primary CT diagnosis because of its relatively poor image quality but is sufficient enough to provide anatomical location. 14 The additional radiation burden from the CT component has also raised concerns but can be addressed using an appropriate low-dose protocol optimized for pediatrics.8,15 Nonetheless, the strength of this report from an educational standpoint is that SPECT/CT imaging is a practical troubleshooting technique that could be implemented together with a low-dose protocol as a standard diagnostic workup for atypical MD. In our case, the co-registration of both SPECT and CT image component was proven advantageous in confirming the presence of a bleeding MD, which could potentially be interpreted as a false-positive MD. With hybrid imaging units becoming more accessible in Southeast Asia, it is anticipated that nuclear medicine physicians in this region will increase their utilization for MD-related examinations.
Conclusions
As a conclusion, we have proved that the patient is presented with a bleeding MD as shown on the SPECT and CT image combination. The usage of hybrid SPECT/CT, although uncommon in standard practices, provided definitive diagnosis via additional anatomic information which helped in accurately localizing the MD and differentiated it from a normal radiotracer activity.
Footnotes
Acknowledgments
NT is the recipient of the 2020–2021 USM Graduate Student Financial Assistance (GRA-Assist) sponsorship and the FRGS Graduate Assistant Scheme (Research). The authors would like to thank Mr. Muhammad Yusri Udin for his technical assistance during the patient preparation and image interpretation. The departments and authors would also like to thank other participating physicians/investigators involved during the management of this patient.
Author Contributions
NT, NACJ, and NMN managed the patient. NT, VWST, YYL, and NMN prepared the manuscript. NT and NMN edited and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We acknowledged the 2020 Fundamental Research Grant Scheme (FRGS) funding by the Ministry of Higher Education Malaysia (203.PPSP.6171279). The funder had no role in the data collection, analysis, interpretation, or writing of the case report.
Ethical Approval
Ethical approval was not sought for this case report because it is not required as per university guidelines. This study was completed following the Declaration of Helsinki.
Informed Consent
The patient’s legally authorized representatives (parents) were informed that his data would be submitted for publication and gave their written informed consent.
Availability of Data
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.