
Abstract
Workplace violence is considered the act or threat of violence, exemplified by verbal threats and or physical threats perpetrated to an employee in the workplace. As part of the ongoing survey research being conducted, workplace violence events (WVEs), specific to sonographers and vascular technologists, were explored. These threats were further categorized based on the four types of WVE proposed by the Injury Prevention Research Center in 2001. Qualitative analysis of this survey data and voluntary comments, provided by study participants, were identified as condescending behavior, and being bullied as major workplace concerns. Further qualitative assessment of the comments resulted in identifying the added risk of Customer/client (Type 2) and Worker-on-worker (Type 3) WVEs, which are considered forms of verbal abuse. This information needs to be considered by each sonographer and vascular technologist and whether it is an issue in their workplace. In addition, a comprehensive workplace violence prevention program is advocated to address workplace incivility and promote worker health, safety, and well-being. Providing annual training is not enough, as workers need to have policies and resources readily available to address WVEs when they occur. These policies and resources should specifically address WVEs perpetrated by patients and co-workers.
The health care workplace has a long history of hierarchical systems of leadership and reporting, which became even more complicated during the 2020–2021 pandemic. Likewise, patients’ and families’ perceptions of health care and its delivery were severely challenged, due to the pandemic, and added immense pressure on the system. Patients’ perceptions of care delivery were based on pre-pandemic norms and as policies began changing during COVID-19, patients and families’ feelings often spilled over into acts of incivility and even violence. In parallel, health care employees and their co-workers having been the focal point of this anger may have resorted to forms of verbal abuse and violence, as an outlet the workplace.
The US National Institute for Occupational Safety and Health (NIOSH) defines workplace violence as “. . . the act or threat of violence, ranging from verbal abuse to physical assaults (PAs) directed toward persons at work or on duty.” 1 Reporting on this rise in workplace violence events (WVEs) has been complicated due to employees fear of health care leaders’ response and already working with fewer co-workers. In essence, ignoring WVEs and hoping that abuse will get better may have been a way of hoping to prevent employee turnover. Nursing research has documented this rise in WVEs and specifically provided empirical evidence of the variety of incivilities to which nursing staff members have been subjected. One such study reported that between 35% and 80% of health care workers have been physically assaulted at one point in their professional career. 2 A study involving two large hospital systems in the United States found a 49% career prevalence of type 2 violence, with a 12-month prevalence of 39%. 3 Yet only 19% of events were officially reported by the employees. 3 As such, underreporting makes it difficult to provide an accurate estimate of the magnitude of the problem. A comparable study of nurses found that 80% of nurses felt unsafe when providing care to psychiatric patients and others during their workday. 4 Although working in a psychiatric environment is highly intense, it does underscore the stress and level of insecurity that can be experienced by health care workers, providing patient care. These stressors have the potential to negatively impact physical and cognitive work performance and could result in injury. We wanted to learn how these types of WVEs might be impacting diagnostic medical sonographers and vascular technologists. A pre-pandemic set of qualitative interviews were conducted by Patton, she interviewed four managers and nine medical imaging technologists. 5 In that study, she explored some of the possible factors that interviewees felt contributed to their workplace conflict. Patton’s analysis found that the antecedents, effects, and management of workplace conflict were affected by three key factors: emotional intelligence, perception of injustice, and sense of empowerment. 5 Patton also explored the notion that a lack of managing workplace conflict had a negative outcome for workers, regardless of the type of conflictual issue. 5 In this work, it was required that participants be registered with the American Registry of Radiologic Technology and nine of the cohort identified as such and were staff level workers. 5 This study was unique and informative but lacked sonographer-specific experiences. A more recent study by Moody looked at interprofessional conflicts between medical imaging work areas. In this qualitative set of interviews, seven of the nine participants worked in sonography or vascular technology. 6 Moody found that many of his participants had been through some type of conflict resolution training, but still expressed a sense that their moral compass was challenged by their work duties. 6 As in the previous study, Moody’s work also underscores the need for management to help restore civility across work groups.
Based on a paucity of data on workplace violence, specific to the lived experience of sonographers and vascular technologists, it seemed important to include these types of questions on the fourth survey of factors related to work-related musculoskeletal injuries, in the longitudinal cohort of sonographers working of in the United States and Canada. In this questionnaire, we asked Likert-type response questions about health and safety in the workplace and provided options for extended responses. This subanalysis is part of the ongoing series of research being conducted on work-related musculoskeletal injuries among sonographers and vascular technologists.7,8
Survey Results From Questions About Workplace Violence
The deployment of survey four included questions that focused on workplace safety climate and culture, as well as questions on policies and procedures, workplace violence, and experience of discrimination. The survey closed in July 2023 with 1239 responses; of those, 1190 were complete. The early and unfiltered findings were as follows, with regard to experiences at work:
26.1% of respondents had been the target of condescending or demeaning behavior.
17.9% had been bullied, threatened, or harassed on the job.
14.6% indicated their workplace is somewhat or very unsafe.
11.5% have experienced age discrimination.
6.6% have experienced gender-based discrimination.
6.0% have witnessed or experienced physical violence.
5.5% have been sexually harassed.
3.9% have experienced racial/ethnic discrimination.
3.6% have experienced religious or cultural discrimination.
These data were then examined as a subset of qualitative analysis that was nested in a larger study of the fourth survey. 9 This specific qualitative analysis of free responses provided about WVEs was reviewed through the lens of the four categories proposed by the Injury Prevention Research Center (2001) 10 and utilized widely by NIOSH (2023), 1 which are:
Type 1: Criminal Intent.
Type 2. Customer/Client: the customer/client relationship to include patients, their family members, and visitors.
Type 3. Worker-on-worker: Worker-on-worker violence is often directed at persons viewed as being “lower on the food chain” such as supervisor to supervisee or doctor to nurse, although incidence of peer-to-peer violence is also categorized here.
Type 4. Personal relationship: The perpetrator has a relationship to the employee outside of work and that relationship spills over to the work environment.
These definitions and categories were used in developing an additional code book to perform the analysis of the extended responses, specific to comments about potential WVEs. Participants were responding to this prompt: Please use the space below to share any additional comments or suggestions you have regarding priorities for addressing the workplace health and safety climate and culture of ultrasound users. This resulted in 187 responses, of which 35 were determined to pertain to WVE. Relevant responses were categorized as verbal assault (VA) or PA and Type (1-4) (See Table 1).
A Sample of the Participant Responses to Addressing the Workplace Health and Safety Climate and Culture of Ultrasound Users, That Concerned Workplace Violence.
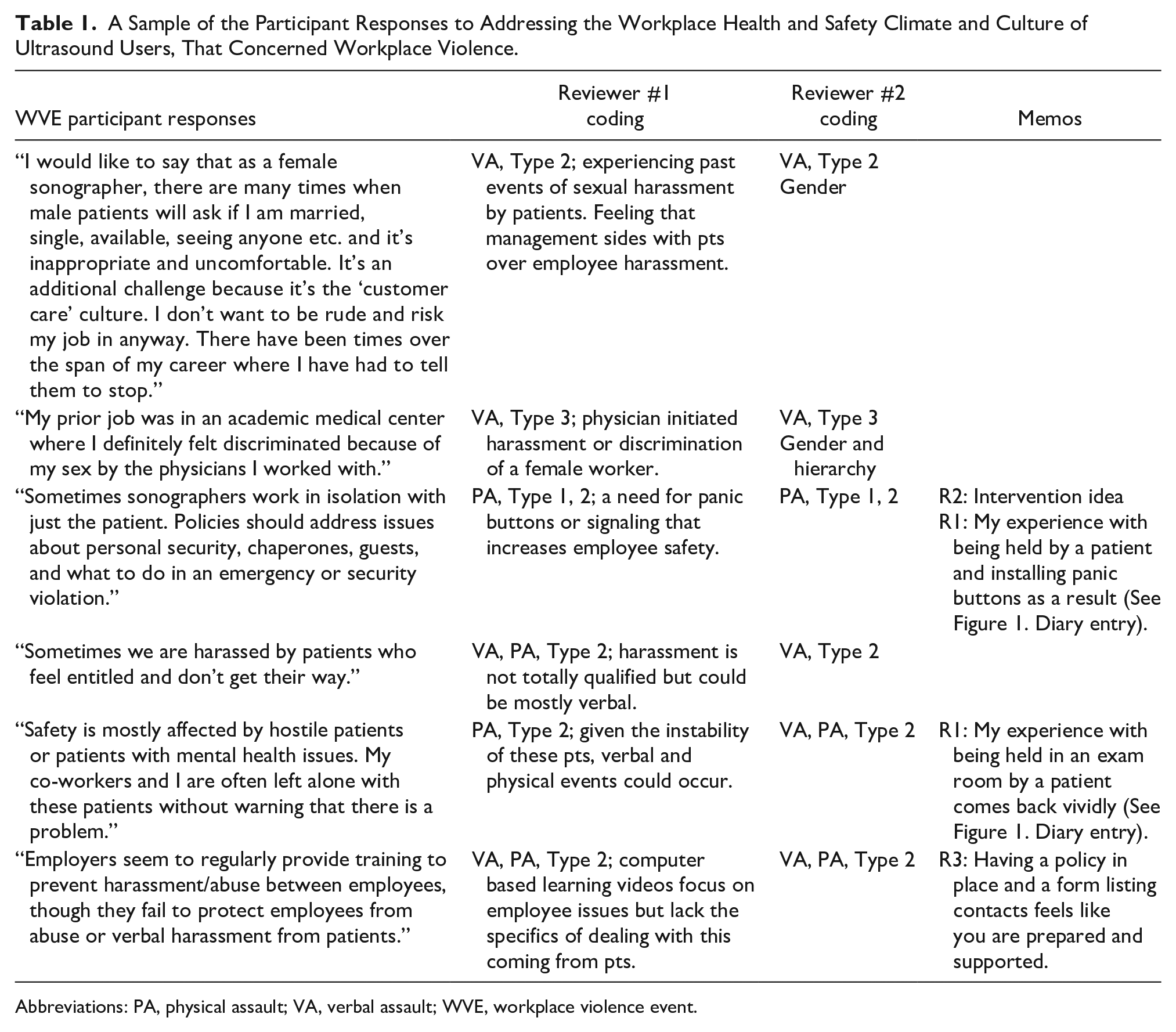
Abbreviations: PA, physical assault; VA, verbal assault; WVE, workplace violence event.
The total breakdown of dual coding resulted in two examples of Type 1, 19 examples of Type 2, 11 examples of Type 3, and one example of Type 4 (note: some examples received more than one Type code). Many of the examples were categorized as VA-verbal, but a number were categorized as PA or VA and PA. These data were also triangulated with data from the memo section and diary entries by the investigators (See Figure 1).
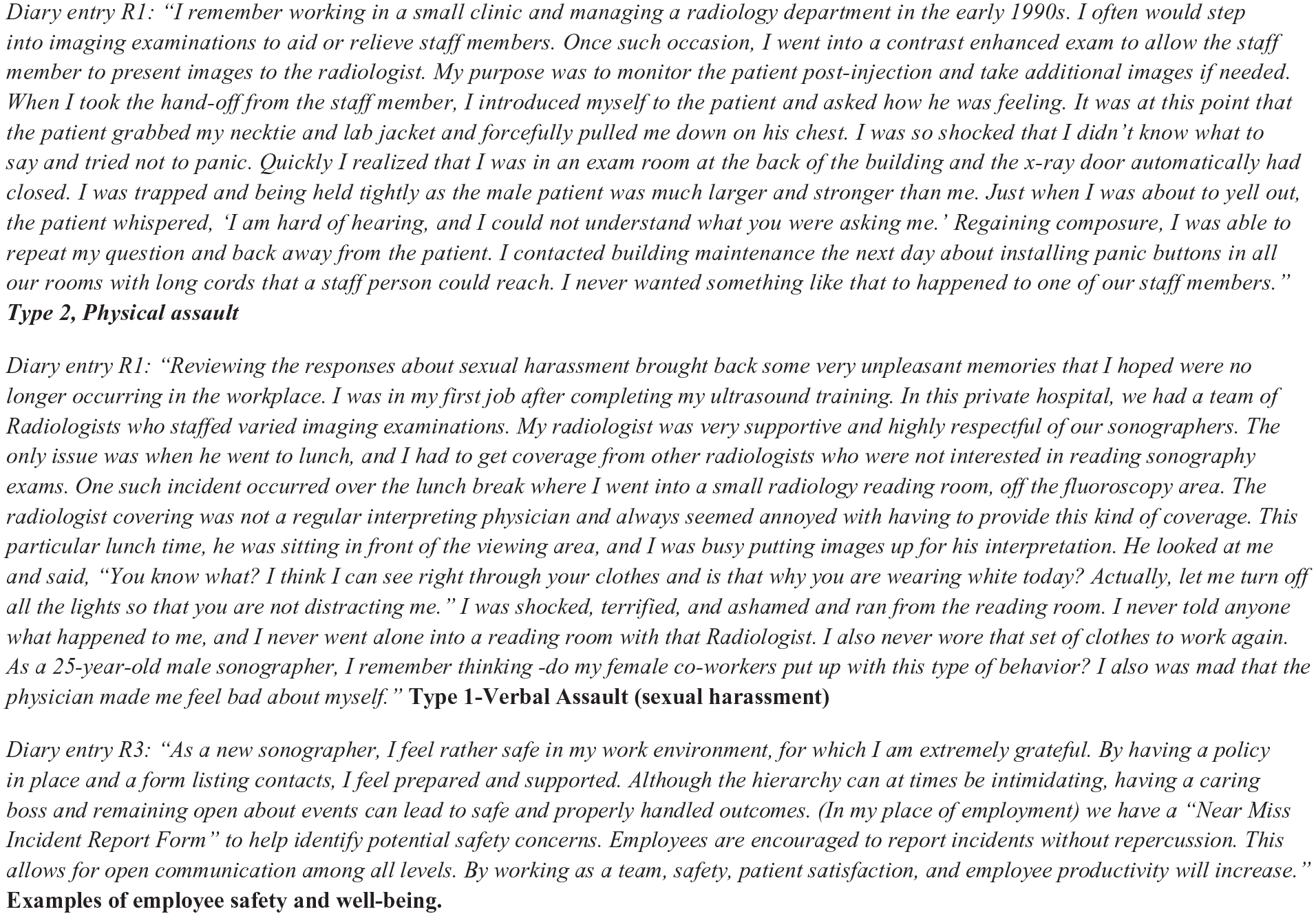
Researchers’ diary entries during the analysis of survey information provided on the topic of workplace violence and threats.
Taking Action to Combat the Use of Workplace Violence and a Lack of Safety
Although these data are a lower percentage of participants reporting WVEs, the fact that these survey comments were provided was shocking and rather distressing. Any incidents of this nature are alarming and need to be taken seriously and neutralized to protect sonographers and vascular technologist, as they complete their work. Most sonographers and vascular technologists are women, and women are at risk factor for experiencing workplace violence. According to a 2019 US Justice Department report, female workers had higher rates than male workers of nonfatal injuries due to workplace violence that resulted in days away from work, across all occupations (5.1 females vs 2.3 males cases per 10 000 full-time equivalent [FTE] workers). 11 Looking specifically at health technologists/technicians, the incidence rate was 14.9 per 10 000 FTE, more than four times the average incidence rate across all occupations. 11 Based on 2015 to 2019 data, the rate of emergency department-treated injuries from workplace violence was 7.1 per 10 000 FTE workers. 11 Tiesman et al 12 reviewed 400 publicly available media reports, of COVID-19-related WVEs, during the first 8 months of the pandemic. Four percent of the reports they reviewed (n = 15) concerned WVEs in the health care industry. 12 Eight of 15 involved physical and non-physical violence, five physical violence only, and two involved only non-physical violence. 12
Given all this very important information, it makes sense to come up with actionable steps to mitigate WVEs and avert both physical and verbal threats. One solution from nursing is the implementation of a comprehensive workplace violence prevention program (also recommended by NIOSH).13,14 This may seem to be a daunting task, but it can easily begin by prioritizing the discussion and formative steps to reduce WVEs, in monthly staff meetings. Allowing sonographers and vascular technologists to share their experiences (in a safe and protected space) may allow for comparing what is happening locally to the data being shared in this article. As a collective group, identifying how to provide resources with staff, plan to get immediate assistance, and have administrative support are vital first steps in developing the program. Other parallel solutions could be the installation of panic buttons or alarms at the reception desk, exam room, and adjoining hallways.15,16 Regardless of the management structure in health care facilities, these incidents of aggressive behavior and incivility must be reported and acted on by leadership. Staff need to feel supported and protected from patient and coworker-initiated incivility. In the case of Type 1 or Type 4 threats of violence, this can be addressed through existing institutional systems (e.g., Title IX, security officers, etc.). It is important to underscore the zero tolerance for sexual harassment of students and staff and a criminal investigation into allegations of sexual harassment or sexual violence does not relieve the school of its duty under Title IX to resolve complaints promptly and equitably. 17 Obviously, these institutional systems and supports should be reviewed as part of the discussion of a comprehensive workplace violence prevention program. What may not be as obvious is the need for mitigating Type 2 and 3 threats, which may be verbal in nature. Ideating as a staff and leadership on the proper response to these verbal threats should include discouraging continued incidents and deescalating this from more physical manifestations. When the staff, co-workers, and management commit to a comprehensive workplace violence prevention program, it becomes a major contributor to protecting and promoting the health and safety of all workers. In some states, the WVEs being experienced by health care workers are being addressed with legislation and of a more national basis, by the Joint Commission.18,19
Conclusion
Workplace violence events are occurring across the health care system and include events being perpetrated by patients and staff in some sonography workplaces. The reporting of the various types of WVEs is critical to better understand the frequency and level of threat occurring in the workplace. This small amount of survey data provided by sonographers and vascular technologists points to the need to support recommendations made by others for comprehensive workplace violence prevention programs, embedded in organizations with strong safety cultures 19 (for additional WVE resources, please click on the QR code for Supplemental Attachment I).
Utilizing staff meetings to further elucidate the kinds of WVEs that are being experienced by staff and how they compare to this report is an important step to addressing this threat to worker health and safety. Although health care leadership is hierarchical and sometimes removed from the day-to-day interactions experienced by staff, management must be involved in mitigating WVEs. A successful and ongoing comprehensive workplace violence prevention program requires that all levels of staff and management come together to support and neutralize these incidents. Proactively identifying methods to address all types of WVEs is important and methods for resolving them for becoming more intense threats. Reviewing existing security resources such as emergency alarms, security officers, and human resources are all part of a robust response to reducing WVEs.
Sonographers not only need to feel safe while at work but also need to feel supported when reporting incidences that occur. Manager involvement in identifying resources is critical, but as mentioned earlier, a part of the problem is that staff will not report events. Some of this is due to fear as well feeling the need to keep up with the patient-centered, customer service–driven environment.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793241260433 – Supplemental material for Addressing the Issue of Potential Workplace Violence Events for Sonographers and Vascular Technologists
Supplemental material, sj-docx-1-jdm-10.1177_87564793241260433 for Addressing the Issue of Potential Workplace Violence Events for Sonographers and Vascular Technologists by Kevin D. Evans, Katherine Smith and Carolyn M. Sommerich in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors thank their research team members, Dr Shawn Roll and Dr Ryan Walsh for supporting this subset of work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.