
Abstract
Objectives:
Sexual assault is the most prevalent and hidden global problem. The condition is worse in developing countries like Ethiopia. Therefore, this study described the survivors’ characteristics, clinical profiles, and management of cases of sexual assault at the One-Stop Service Center for survivors of sexual assault at a referral hospital in Western Ethiopia.
Methods:
A facility-based retrospective cross-sectional descriptive study was conducted to assess 203 cases of sexual assault managed at the One-Stop Service Center for survivors of sexual assault in Wollega University Referral Hospital from January 2019 to March 2022. Data were collected using a pre-tested structured checklist. Data were organized using Epidata version 3.1, cleaned, and exported to SPSS version 25 for analysis. The results were presented in tables.
Results:
Of 203 cases of alleged sexual assaults during the study period, 142 (70%) and 61 (30%) of survivors were raped and attempted rape, respectively. The age of survivors ranges from 3 to 28 years with a mean age of 15.7 ± 4.7 years. One hundred ninety-four (95.6%) were females. Seventy percent of them were students. Most of the survivors, 173 (85.2%), were assaulted by a person known to them. Only 74 (36.5%) present to the hospital within 72 h. Genital injuries were documented in 153 (75.4%). More than half, 112 (55.2%), were brought to the hospital by the police officers. In this study, 34 (16.7%) of survivors were admitted and 10 (4.9%) needed surgical procedures. Serology for syphilis, hepatitis B virus and HIV were reactive in 5 (7.1%), 1 (0.5%), and 1 (0.5%) respectively. The pregnancy test was positive in 12 (7.1%) of survivors. One (0.5%) study participant died in the intensive care unit.
Conclusion:
In this study, children and adolescents were the most vulnerable group, and survivors’ presentation to the hospital was delayed. They presented to the hospital with variable complications, including minor genital and/or extra-genital injuries, sexually transmitted infections, unwanted pregnancy, fractures, and multiple organ failures leading to death. Therefore, it is recommended that all concerned stakeholders work on the prevention of sexual assault in the study area. Legal protection for these survivors and students should also be strengthened. It is also recommended to evaluate the execution of existing national and international policies and programs toward sexual assault to develop contextual policies and guidelines.
Introduction
Globally, lifetime prevalence of gender-based violence (GBV) against women has been reported to be increasing. GBV can happen to any age group, at any place, or committed by anybody. Among the different forms of GBV, rape is the most common type.1–3 The prevalence of rape varies from region to region. It is 3.3% in South Asia and 21% in sub-Saharan Africa. 1 In Ethiopia, GBV is common among married and unmarried women. 4 According to the 2016 Ethiopian Demographic Health Survey (EDHS) report, more than one-third of ever-married women reported some form of GBV. 5
Sexual assault is a major form of sexual violence affecting women. It includes rape, attempted rape, sexual abuse, and sexual exploitation.6,7 According to the World Health Organization (WHO), a sexual assault survivor is any person, irrespective of age, reporting any type of non-consensual sexual activity, whether attempted or completed. 8 Sexual assault carries different risks to the survivors, including but not limited to physical injuries, sexually transmitted diseases, unwanted pregnancy with its complications, psychosocial trauma, and suicide.9–11 However, it is usually underreported. Survivors usually prefer to keep their painful experiences to themselves. This is because of fear of the assailant or social reaction, poor decision, poverty, or lack of information on where to report.10–12
The nature and forms of sexual assault may vary with time and from place to place. In Ethiopia, there are different centers giving services to survivors of sexual assaults. One-Stop Service Center for survivors of sexual assault in Wollega University Referral Hospital is the only center giving referral services for the survivors in the Western part of Ethiopia. Therefore, this study is aimed to determine survivors’ characteristics, clinical profiles, and management of cases of sexual assault managed at this center.
Methods and materials
Study setting and period
The study was conducted from 5 January 2019 to 25 March 2022 at the One-Stop Service Center for survivors of sexual assault in Wollega University Referral Hospital, Western Ethiopia. The hospital is located in Nekemte town 331 km west of Addis Ababa. The center was established with financial support from United Nations Population Fund (UNFP) to give service to survivors of sexual assault in the Western part of Ethiopia. It is giving free services, including but not limited to medical evaluation, treatment, psychosocial support, and legal aids. The center is run by a team of gynecologists, nurses, psychologists, public health experts, pharmacists, laboratory technologists, and legal advisors:
Study design: A facility-based retrospective cross-sectional descriptive study.
Source population: All clients getting reproductive health services at Wollega University Referral Hospital.
Study population: All survivors of sexual assault are managed at the One-Stop Service Center for survivors of sexual assault in Wollega University Referral Hospital.
Inclusion and exclusion criteria
All cases with complete documentation were included in the study while others were excluded.
Data source
The patients’ medical records were included in the study. Then, the data were retrieved from the logbook at the center. Accordingly, 210 documents were identified. From these, 203 documents were found to contain all study variables and thus included in the study.
Operational definitions
Sexual assault: A major form of sexual violence that includes at least rape, attempted rape, and sexual abuse.
Rape: An act of non-consensual sexual intercourse, including the invasion of any part of the body with a sexual organ and/or the invasion of the genital or anal opening with any object or body part.
Attempted rape: Efforts to rape someone which do not result in penetration.
Assailant: A male or female, group or institution that inflicts, supports, or condones violence or other abuses against a person or group of persons.
Survivor: A person who has lived through an incident of sexual assault.
Data collection procedures
Two nurse professionals and one public health expert were recruited and trained to collect data. A logbook review was done to collect the data. Data were collected using checklist which was developed by reviewing different works of literature.1,3,4,6–19 A pretest was conducted on 10 (5%) of the samples. All checklists were checked for completeness by the principal investigator.
Statistical analysis
The data were coded and entered into Epi Data version 3.1, and then cleaned and exported to Statistical Package for Social Sciences (SPSS) version 25 for data analysis. Descriptive statistics like frequency and percentage were computed for data presentation. Finally, the results were presented in tables.
Results
In this study, a total of 203 survivors of sexual assault were included. The age of study participants ranges from 3 to 28 years with a mean age of 15.7 ± 4.7 years. One hundred ninety-four (95.6%) of study participants were females while 9 (4.4%) were males. One hundred fifty (73.9%) and 53 (26.6%) of study participants were from rural and urban areas, respectively. More than half, 109 (53.7%), of them live with their families. One hundred forty-two (70%) of the study participants were students (Table 1).
Socio-demographic characteristics of survivors of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.

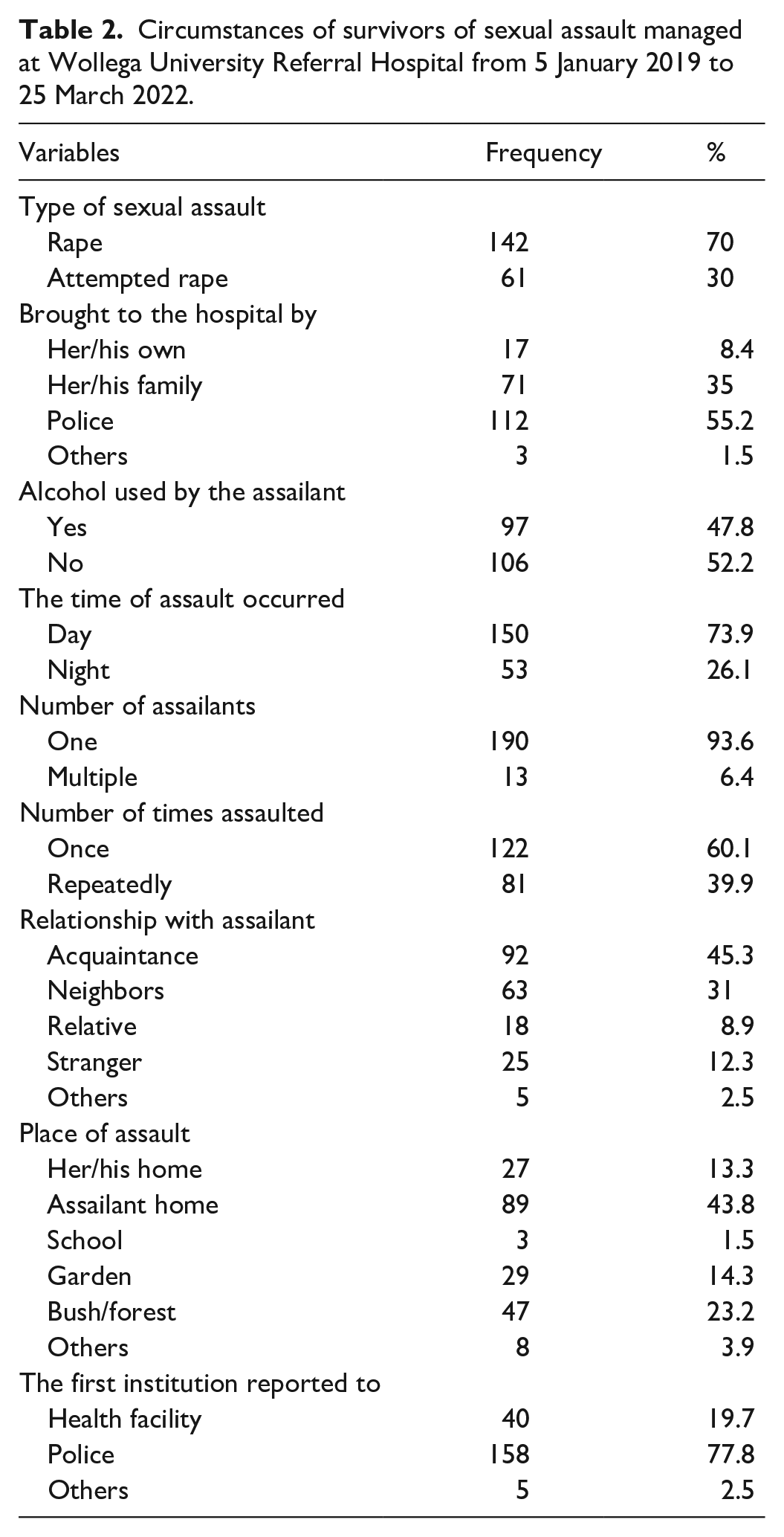
In this study, 142 (70%) and 61 (30%) of sexual assaults were rape and attempted rape, respectively. One hundred twelve (55.2%) of study participants were brought to the hospital by the police. The assailants used alcohol in 97 (47%) of the study participants. One hundred fifty (73.9%) of the assaults were committed during the daytime. Thirteen (6.4%) of the assaults were committed by multiple assailants. One hundred twenty-two (60.1%) of the study participants were assaulted once, while 81 (39.9%) were assaulted repeatedly. Ninety-two (45.3%) of the study participants were assaulted by acquaintances, followed by neighbors 63 (31%). Eighty-nine (43.8%) of the assaults were committed at the assailant’s home (Table 2).
Circumstances of survivors of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.
In this study, the time interval between the incident of sexual assault and presentation to the hospital ranged from a few hours to many days. Only 29 (36.5%) of the study participants present to the hospital within 72 h. Genital injuries were documented in 153 (75.4%) of the study participants. Of those study participants in whom the genital injuries were documented, 149 (97.4%) had a hymeneal tear. Only 35 (17.2%) of study participants had non-genital injuries. Bruises were the most common non-genital injuries (14 (40%)) (Table 3).
Injuries and time of presentation of survivors of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.

Abbreviations: RVF: Rectovaginal fistula.
Regarding laboratory investigations performed, the pregnancy test was done for 168 (82.8%) study participants. From this, 12 (7.1%) were found to be pregnant. Of the total study participants tested for sexually transmitted infections (STIs), 1 (0.5%), 5 (7.1%), and 1 (0.5%) were found to be reactive to HIV, syphilis, and hepatitis, respectively. A wrist x-ray was done for all study participants. A vaginal or anal swab for sperm analysis was not done at all (Table 4).
Laboratory investigation performed for survivors of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.
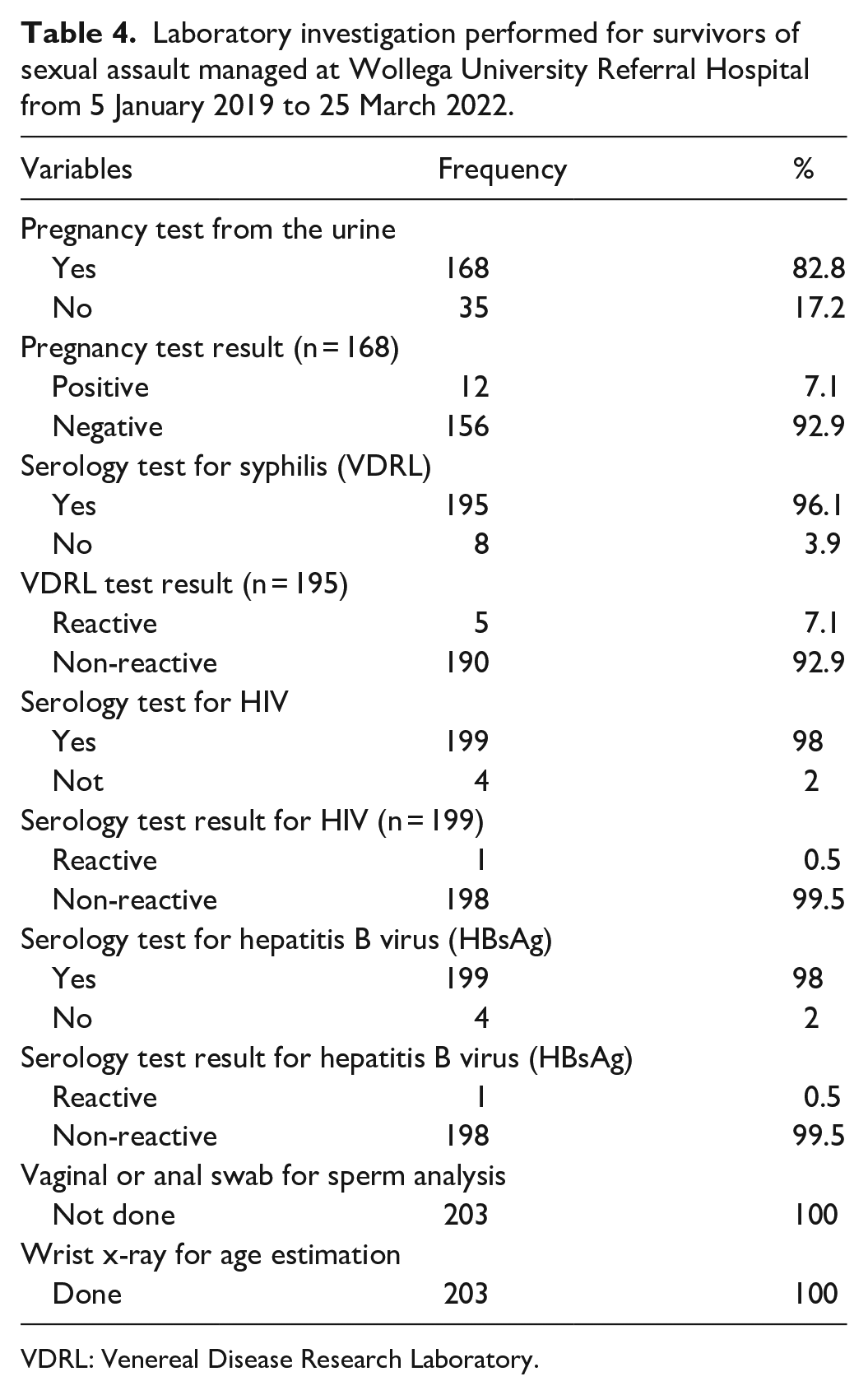
VDRL: Venereal Disease Research Laboratory.
In this study, prophylaxis for HIV, 51 (68.9%), and other STIs, 70 (94.6%), were given. But prophylaxis for hepatitis virus was not given to eligible study participants. Emergency contraception was provided for 49 (50%) of eligible study participants. Surgical procedures were performed on 10 (4.9%) of the study participants. The majority, 197 (97%), of study participants obtained psychosocial support during their visit to the center. To process legal issues, a medical certificate was provided to 171 (84.7%) of the study participants. Thirty-four (16.7%) of the study participants were admitted to the center for at least 24 h to receive care and psychological support. Three (1.5%) of the total study participants were admitted to the intensive care unit. One (0.5%) patient was dead in the intensive care unit (Table 5).
Prophylaxis and care provided for survivors of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.

STIs: sexually transmitted infections.
Discussion
Sexual assault is the most underreported crime in the world. 6 Data on types of sexual assault, interventions provided, and related complications are obtained from hospital-based studies.1,3,6 Accordingly, we analyzed a total of 203 cases of sexual assault managed at Wollega University Referral Hospital from 5 January 2019 to 25 March 2022.
In this study, the age of study participants ranges from 3 to 28 years, with a mean age of 15.7 ± 4.7 years. The majority, 88.1%, of them were teenagers. In the study conducted at Gandhi Memorial Hospital, 73% of study participants were below 18 years. 13 Another study at Saint Paul’s Hospital Millennium Medical College in Addis Ababa, Ethiopia, showed that 82.4% of study participants were teenagers. 3 This might be explained by the fact that teenagers are particularly vulnerable because they are still dependent on older individuals and their relatives for most of their needs. 14 Another possible reason for this observation is that children are less likely to offer resistance to their assailants. 19
In Ethiopia, homosexuality is forbidden by law. 16 However, in this study 4.4% of the survivors were males. This is similar to other studies at Saint Paul’s Hospital Millennium Medical College in Addis Ababa, Ethiopia (4.3%), 3 and Jimma University Medical Center (4%). 16 This indicates how sexual assault is becoming a huge medicolegal issue in the study setting and Ethiopia in general.
In this study, most of the survivors, 85.2%, were assaulted by a person known to them (acquaintances, neighbors, and relatives). This is similar to a study conducted at Gandhi Memorial Hospital in Addis Ababa, Ethiopia (87.8%); 13 Lagos State University Teaching Hospital, Nigeria (83.5%); 15 and University Hospital Brazzaville, Congo (83%). 17 But the current finding is higher than the study conducted in Kenya (76%). 18 The psychological complications of sexual assault carried out by assailants known to survivors could result in more damaging outcomes than being assaulted by a stranger. Such incidents could also destroy the ability of survivors to trust people.15,19
This study reveals that the time interval from the incident of sexual assault to presentation to the hospital ranges from a few hours to several days and weeks. Only 36.5% of the study participants present to the hospital within 72 h. More than half of the study participants, 51.7%, present to the hospital 5 days after the incident. Similar studies conducted in Addis Ababa, Ethiopia, showed that 28.3% of study participants present within 72 h of the incident. 3 Another study conducted in Jima, Ethiopia, showed that 20.9% and 50% of study participants presented to the hospital within 72 h and after 5 days, respectively. 16 The delayed presentation is because of the high percentage of children and teenagers (88.1%) in the current study who might not report until the parents notice the condition. It can also be explained by the fear and embarrassment that they envisaged. 13 This delayed presentation made the provision of emergency contraception and prophylaxis for STIs very difficult. Most health care interventions for survivors can only be delivered when the survivors present in the first 1–5 days of sexual assault to prevent complications. 6 In this study, emergency contraception is only provided for 50% of eligible participants. Similarly, only 8% of study participants in Jima received emergency contraception. 16
In this study, more than half of the survivors (55.2%) were brought to the hospital by police officers. This might be the reason why patients’ presentation to the hospital within 72 h was only 36.5%. A similar study at Jimma University Medical Center showed that 72.2% of the survivors were brought to the hospital by police officers. 16 This implies that survivors give priority to the legal aspect than the health-related complications of sexual assault.
In this study, genital injuries were documented in 75.4% of the study participants. This is similar to the study conducted in Jimma University Specialized Hospital (75.4%) 6 and Addis Ababa (71.8%). 3 This finding carries a higher risk of acquiring HIV and other STIs, particularly in the setting where patients came to the hospital late and routine prophylaxis is not provided. 20 Two percent of study participants with genital injuries had a rectovaginal fistula. This was not reported in similar studies.3,6,16
Comprehensive management of sexual assault involves clinical care, provision of prophylaxis for STIs, psychosocial support, and collecting pieces of evidence for the medicolegal process. 21 Provision of post-exposure prophylaxis to HIV-negative persons presenting within 72 h of sexual assault is recommended. 6 In this study, prophylaxis for HIV was provided for 68.9% of study participants. It is also lower in similar other studies conducted in Ethiopia.3,21 Prophylaxis for other STIs (gonorrhea, syphilis, chlamydia, and trichomonas) was provided for 94.6% of eligible participants in our study. But none of them received prophylaxis for hepatitis B virus.
In this study, the legal certificate was given to 84.7% of survivors. This is higher than the study conducted in Saint Paul’s Hospital Millennium Medical College in Addis Ababa, Ethiopia (45.5%) 3 but lower than the study done in Jimma University Medical Center (98.9%) (16). A legal certificate helps the survivors to get an appropriate legal service which discourages the act of sexual assault.
Unlike other hospital-based studies,3,6,13,17 in this study there was a patient who died from complications (genital and non-genital injuries) of sexual assault. There were also cases with severe forms of physical injuries, including rectovaginal fistula and fracture.
Limitations
In this study, the sample size was not calculated. The other limitation is it is that this study is hospital-based, making generalization difficult. There could also be recall bias from survivors who were children. The sensitivity of the issue could result in bias. In addition, the psychiatric complications were not addressed.
Conclusion
In this study, children and adolescent girls were the most vulnerable group and survivors’ presentation to the hospital was delayed. They presented to the hospital with variable complications, including minor genital and/or extra-genital injuries, sexually transmitted infections, unwanted pregnancy, fractures, and multiple organ failures leading to death. Therefore, the authors recommend all concerned stakeholders work on the prevention of sexual assault in the study area. Legal protection for these survivors and students should also be strengthened. It is also recommended to evaluate the execution of existing national and international policies and programs toward sexual assault to develop contextual policies and guidelines.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221126328 – Supplemental material for Sexual assault cases managed at a referral hospital in Western Ethiopia: A retrospective cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221126328 for Sexual assault cases managed at a referral hospital in Western Ethiopia: A retrospective cross-sectional study by Temesgen Tilahun, Rut Oljira and Ayantu Getahun in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge Wollega University Referral Hospital for facilitating the process of data collection. Our appreciation also goes to the supervisors and data collectors.
Author contributions
T.T., R.O., and A.G. were involved in all components of this research, including conception, design, and supervision of data collection; data analysis; and write-up of the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The data sets are available from the corresponding author on a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethical clearance was obtained from the Research Ethics Review Committee of Wollega University with the number WU/RD/571/2014. The letter was written to Wollega University Referral Hospital. The hospital was informed of the objectives of the study and permission to get access to patient documents. All methods were performed per the relevant guidelines and regulations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
In this study, the need for written informed consent was waived by the Ethical committee due to the retrospective nature of the study.
Trial registration
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.