
Abstract
Background
Critical care environments are potentially high-risk areas for staff harm due to procedural demand and increased incidence of delirium/dependence. The principal types of harm and temporal trends have not yet been quantified.
Methods
Retrospective analysis of a multicentre dataset prospectively collected over a five-year period. All patient safety incidents reported to a regional network project were analysed; those recorded as staff harm were extracted, quantified and assessed by thematic analysis to identify key areas of harm, temporal trends and incident rates.
Results
Staff harm accounted for 7% of all reported patient safety incidents over the study period. Incident rates remained static, ranging annually from 2.6 to 3.7 episodes/1000 patient days. Assaults on staff accounted for the highest proportional contribution on thematic analysis, which was a consistent annual finding. Sharps injuries and manual handling incidents were also notable contributions. Temporal trends for each theme remained static over the study period implying limited reduction in staff harm despite implementation of national guidance and local initiatives.
Conclusion
Staff harm is a consistent issue for those working in critical care. Assaults on staff appear to be the highest contributor on thematic analysis. These data imply significant reduction in harm can still be achieved and can be used to design and implement interventional measures.
Introduction
Although caring for seriously unwell patients can be a very rewarding occupation, staff working in critical care units face a number of risks to their own health. Patients are of the highest acuity with regard to illness and in addition have higher rates of delirium, obesity and agitation than standard medical and surgical inpatient environments.1–4 In addition, patients have a higher rate of exposure-prone interventional procedures. 5 It follows that critical care staff are likely to be at increased risk for potential occupational injuries specific to these factors, such as sharps injury, mucous membrane exposure and musculoskeletal manual handling injuries. Employers are required by statute to control these risks. 6 In addition, maintaining a healthy and motivated workforce is also clearly important for providing safe patient care. Unfortunately, data collection on this challenging topic is limited and practice development often subsequently reactive, rather than proactive.
Patient safety incident reporting is designed to highlight concerns regarding harm or potential harm to patients. However, over a five-year period of analysis we noted that 7% of all incident reports from critical care units in the North West of England described harm suffered by staff. We decided to analyse these reports further to characterise and identify the frequency of common risks to critical care staff and provide data on temporal trends. Our aim was to identify common and persistent risk patterns in order to focus prospective efforts on controlling these risks, in an attempt to reduce harm and improve staff safety.
Methods
We performed a retrospective analysis of a multicentre, voluntary, prospectively collected, critical care incident reporting dataset. Incidents were prospectively reported by staff from up to 30 critical care units in the North West of England between 2009 and 2013; the staff used incident reporting software to record a free text description of the incident and to provide a classification of the incident at the time of occurrence. The free text descriptions of the incidents together with any manager's report were all stored by hospital trusts for submission to the UK National Reporting and Learning System.
The critical care units provided us with Excel spread sheets that contained the date of the report, the free text description of the incident reports and, where available, the manager's summary and action report. The units also provided us with annual reports of their ways of working and clinical activity. The text of the incident and manager's report allowed the incident to be placed into one or more of a number of main incident groups, one group being ‘injury to staff’. A detailed description of the initial classification process is currently available on the Greater Manchester Critical Care Network website. 7 The classification was either carried out by a senior member of staff on the reporting unit who then sent the completed database table to the lead investigator for checking or the incidents were classified by the lead investigator (ANT). Training material for classifiers was provided on an open access website and augmented by a one-day course for classifiers facilitated by the lead investigator. 7
In return, we provided each unit with annual reports describing a summary of their incidents, with accompanying comparative, anonymised regional data from other units for all patient safety incidents. These reports included incidents involving staff harm. We also calculated the rate of incident reports per 1000 patient days, from the number of patient days as defined by the UK Department of Health's minimum dataset for critical care. 8 Apart from providing these reports, there were no specific quality improvement projects during data collection to improve staff safety over the period of the study; individual trusts were left to analyse the comparative data and implement measures as they saw fit.
For this specific project, we extracted incidents classified as staff injury from the complete dataset of patient safety incidents in order to reclassify them into more detailed subgroups than those in the original dataset. A descriptive process for this subcategorisation can also be found on the network website. 7 In brief, we retrospectively analysed all incidents highlighted as staff injury by initial classification and performed subsequent thematic analysis, in order to subcategorise and analyse trends. Thematic analysis and subcategorisation were performed by the first (ANT) and second author (DH). Disagreements were resolved by consensus. All incidents were reviewed by the lead author prior to inclusion in the final dataset. Five units had actively removed incidents classed as injury to staff from their datasets in line with previous guidance. 9 Returns from these units were not used to calculate incident rates but incidents where they had inadvertently reported staff harm were used in the thematic analysis. Statistical analysis took the form of descriptive data interrogation only and calculation of reporting rates. Median values with interquartile ranges are provided for data without normal distribution.
Results
Thirty critical care units submitted incidents from the three critical care regional networks in the North West of England. Units joined and left the reporting process such that 16 units submitted incident reports during 2009 and 24 units provided reports during 2013. Five units filtered most staff harm incidents from their reports prior to submission as previously described.
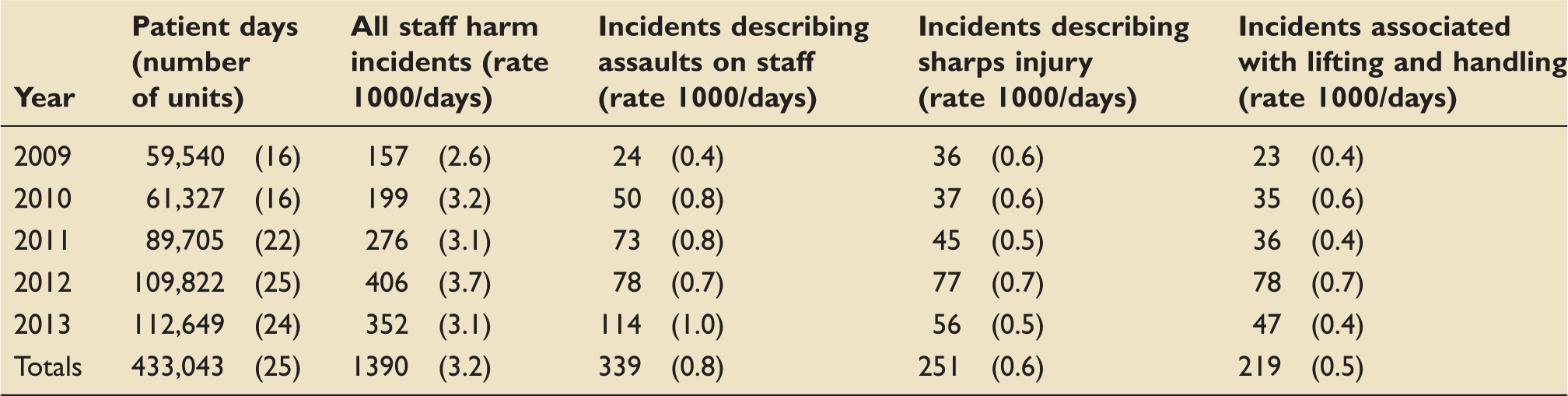
In total 19,945 incident reports were produced and categorised over the five years, of which 1390 (7%) were initially classified as involving harm to staff. The original text for these incidents contained a median of 203 characters per report (IQR 116–277); manager's reports were provided in 1028 of staff harm incidents (74.0%); these summary and action reports contained a median of 154 characters (IQR 66–255). There was a median of 3.5 incident reports regarding staff harm per 1000 days (IQR 2.5–4.2/1000 days) for individual units.
Numbers of staff harm incidents reported per year stratified by number of units reporting and number of patient days in these units (there were an additional five units that removed most of the incidents associated with staff injury). The table also shows the numbers and rates/1000 patient days for all incidents describing staff harm and numbers and rates of the most common types of staff harm.
Total numbers of different types of physical assaults on staff together with the body areas of staff affected and characteristics of patients associated with the assaults.
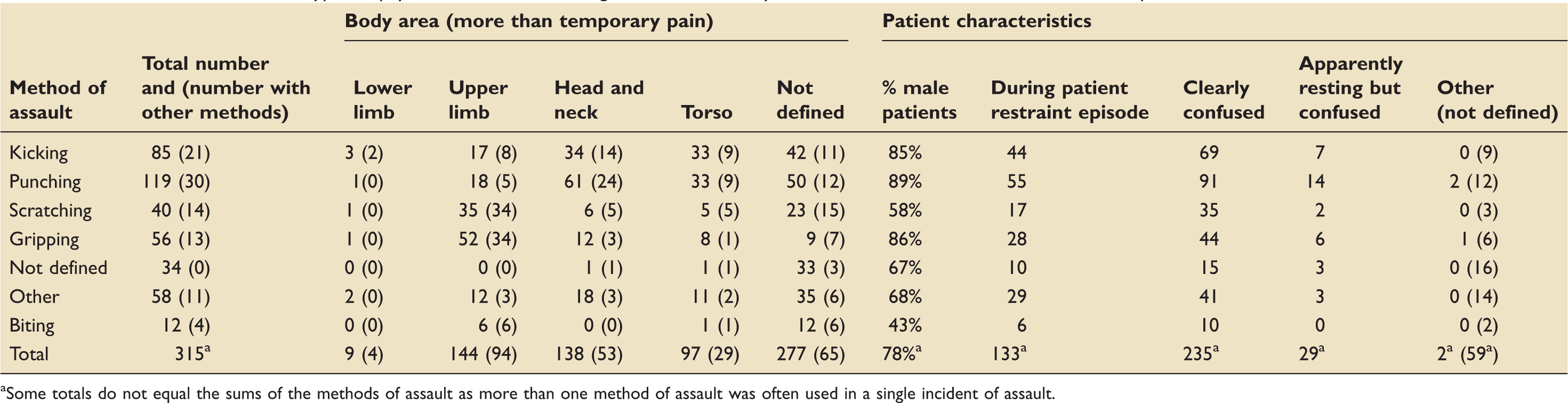
Some totals do not equal the sums of the methods of assault as more than one method of assault was often used in a single incident of assault.
Within the complete dataset of patient safety incidents (19,945 incidents), there were 885 incidents (4.4%) associated with organic confusion. Security staff were contacted in 389 of all incidents (2.0%); in all cases involving security, there were no free-text descriptions to suggest their presence had been a hindrance or that they had contributed to staff or patient harm. There was only one episode of patient harm described during assaults on staff: bruising to the arm of a patient with a known coagulopathy. A total of 131 (0.6%) incidents were associated with patient restraint. Attempts to prevent removal of essential medical devices or oxygen accounted for over half of these restraint episodes (71/131, 54.2%).
With respect to manual handling incidents, nursing and health care support workers were involved in 200 of 201 incidents where the staff harmed during the incident were adequately described. Of the total 219 manual handling incidents, 40 (18.3%) involved non-patient activity, 93 (42.5%) involved re-positioning in bed, 27 (12.3%) restraining confused patients and 35 (16.0%) transferring the patient or assisting mobilisation. Of the 177 episodes directly involving patients, 44 (24.9%) described patient confusion and 30 described the patient as obese (16.9%). With regard to consequences, more than temporary pain was described in 73 of 219 manual handling incidents (33.3%), implying a third of cases had implications for future working practice, be that a short period of respite or longer term occupational health assessment. A proportion of the incidents resulting in more than temporary pain had documented aggravating previous injuries (24 cases – 32.9%). Manual handling incidents predominately occurred in staff working independently (105 incidents – 47.9%). Incidents occurring in staff working as a pair were recorded on 42 occasions (19.2%) and in a team on 62 occasions (29.7%). Problems with medical equipment were specifically highlighted in 26 manual handling incidents (11.9%) and problems with staff shortages in 13 incidents (6.0%).
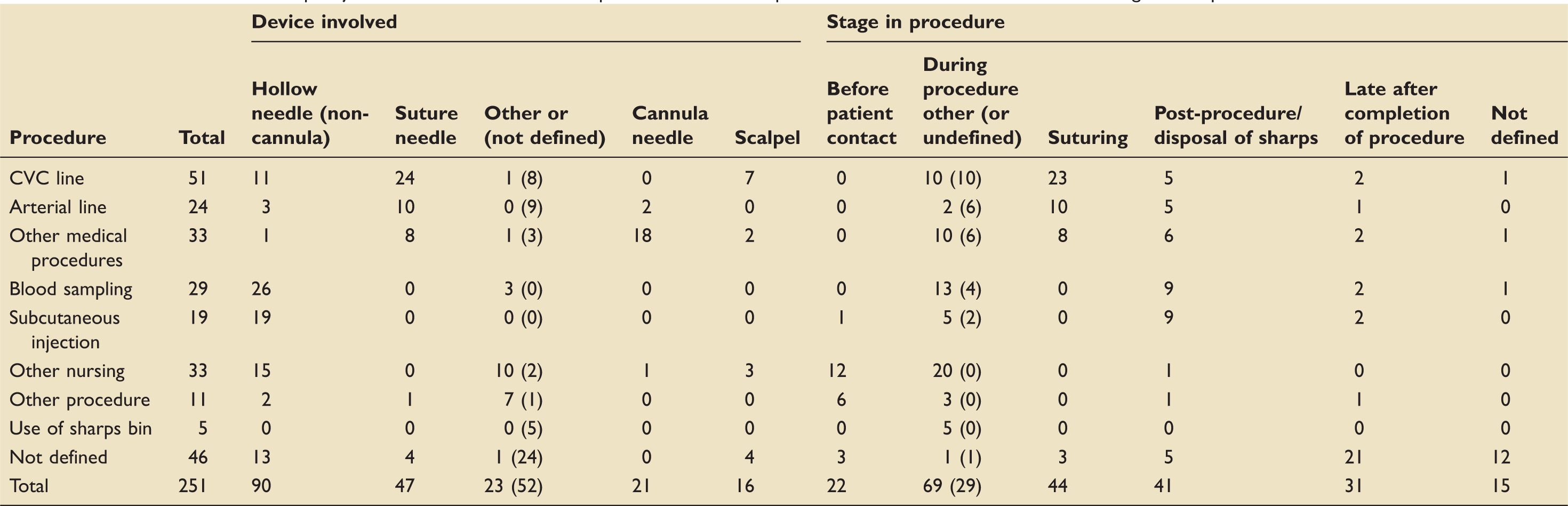
Shows the number of sharps injuries associated with different procedures; for each procedure, the devices involved and the stage in the procedure are also defined.
There were 151 reports of other contamination of staff with body fluids: 107 (70.9%) reports described eye contamination, eight oral contamination, 28 facial contamination, eight other areas. Of the 151, patients were described as confused in 14 (9.3%) incidents and high risk in 21 (13.9%) incidents. In the 145 incidents where the procedure was defined, 48 (33.1%) occurred during unplanned ventilator disconnections, six during planned disconnections, 20 during blood sampling and the remaining occurred in a wide range of other procedures. Protective equipment was described as being used unsuccessfully in 14 incidents and described as not used in the vast majority (130–86.1%) of cases. Contamination was with sputum or ventilator tubing fluid (65 incidents); blood (46 incidents); and urine, gastric contents or other body fluids (40 incidents). Fluid was pressurised by coughing, mechanical ventilation or pressurising syringes. There were 18 additional cases of eye injury due to chemical exposure.
With respect to the 144 incidents describing trips and falls, 18 involved slipping on floors being cleaned (placement of warning signs was described in 13 incidents), 43 involved spillages, commonly at bed areas, around sinks and in the sluice. Tripping over wires was described in 15 incidents.
With respect to other injuries, 63 incidents described collision with moving objects (30 of these objects were medical equipment including eight oxygen cylinders and six beds or X-ray machines) and 54 collision with static objects (frequently movable objects around the bed space). Sixteen described burns and scolds, 12 incidents described electric shocks, six due to faulty equipment or damaged cables and six most likely due to static discharge.
Discussion
The original guidance for patient safety incident reporting specifically excluded incidents involving staff injury. 9 However, the alternate reporting process does not feedback information about staff harm to clinical teams in critical care and as such fails to highlight increasing trends or factors in need of attention/action. 10 In an area with limited published data, this study reports incidence rates, thematic analysis and temporal trends regarding staff injury in critical care over a five-year period and offers valuable insight into the severity and nature of the issue. These data also highlight several issues amenable to intervention and subsequent potential reduction in staff harm.
Our study has several limitations, mostly as a consequence of the free-text reporting system. The descriptions of staff harm in our reports frequently missed important information about genesis of the incident or how it was controlled. Reports also never provided information about longer term outcomes and the immediate consequences were frequently poorly described. These deficiencies are in part because the reporting system does not provide a structure to support the collection of this information. Some examples of how the collection of follow-up information could be facilitated are available on the Greater Manchester Network website; these structured tables would also facilitate the investigation of the incident reports.
With respect to sharps injury, the annual rate remained relatively constant over the five years of incident reporting. Critical care has previously been identified as a high-risk environment for viral transmission. Even potential exposure to infection through sharps injury may have serious consequences for staff and adverse implications for patients. 11 There are actions that can reduce the chance of acquiring such an infection, including education and training programs regarding sharps safety and improving the provision of equipment. The relatively small number of injuries associated with cannula needles suggests the European Directive Health and Safety (Sharps Instruments in Healthcare) Regulations 2013, ensuring the use of guards for these devices, will have a modest influence on the total rate of sharps injury. 12 Other parts of the directive should provide some force to the implementation of best practice in prevention of sharps injuries, as such critical care units should ensure they are compliant. A detailed review of all sharps injuries would produce a better idea of the causative factors and an ongoing review would demonstrate the effectiveness of interventions to reduce these injuries.
The increase in staff injury caused by assaults, almost entirely from patients, between 2009 and 2013 may reflect a greater understanding of the dangers of excessive sedation in critical care and an increasing reluctance to use chemical restraint.13,14 National guidance on the management of aggressive or violent patients is available, particularly in emergency departments. 15 However, this guidance is mainly focussed around de-escalation of potential conflict in well patients, with either limited organic illness or specific mental health issues. It does not address the key issues specific to critical care, where staff should be judicious in limiting administration of sedative medication but patients can often be delirious when awake and dependant on removable medical devices. There has been much progress in raising awareness of delirium in a critical care environment over the last decade; many researchers are now focussing efforts on producing guidelines and decision tools to identify, categorise and manage delirium which will no doubt impact on the clinical approach to the agitated or aggressive patient.16,17 In addition, the spectrum of delirium encompasses the hyperacute patient, who often presents an acute risk to self and staff. This is not an uncommon scenario in our clinical experience. There is a need for guidance specific to critical care around this particular high-risk situation. This could be described as a series of steps starting with preventative policies that should be part of routine practice (for example to manage delirium and uniform policies), followed by steps to manage the patient who is increasingly confused and aggressive (including managing the environment, removal of invasive lines where possible and communicating with relatives and appropriate staff). There should then be an agreed management plan should the situation deteriorate, setting out which drugs could be used and over what timeframe. Finally, there should be defined follow up of staff, patients and relatives. From these data, the use and type of chemical restraint appears to vary widely. National guidance on medication use did not seem to be routinely followed in the few incidents where the choice of sedative drug was described within the incident report. 16 The use of structured patient safety incident reporting to provide a detailed description of the aetiology, management and consequences of episodes of acute delirium and psychosis in critical care could minimise this data loss and make the most of each important opportunity to improve care of aggressive or confused patients. An example of such a structure is given in our website. 7
Although less common than transmission following sharps injury, blood-borne viruses may be transmitted via mucus membranes and broken skin.18,19 Most episodes of eye and other mucosal contamination described in the incidents within this study could not have been anticipated as they occurred during unplanned ventilator disconnections or as a consequence of pressurising syringes. However, the lack of protective equipment used is perhaps a concern. It may be possible to improve the utility and quality of eye protection (14 episodes occurred despite the use of such equipment). Rigorous enforcement of eye protective equipment would be required to prevent the described incidents. Such enforcement could, however, make patients more confused and reduce the situational awareness of staff, so off-setting the benefits of eye protection.
Chronic back pain is the most common reason for retirement due to ill health in nursing staff. 20 Manual handling incidents are highly likely to contribute to this burden and as such should be interrogated, reflected upon and negated through quality improvement measures and other educational interventions. The incidents reported within this study suggest that manual handling of confused patients is potentially challenging, staff shortages can directly impact on the incidence of injury and equipment should be readily available to manage obese patients. There were a surprising number of incidents describing staff moving patients on their own; manual handling teams may have a more practical role in critical care. 21 A multifaceted approach of equipment provision, training and ensuring best practice compliance should form the basis for manual handling in critical care. 22
Many other injuries, for example slips and falls and collision with moving or static objects, could be preventable through basic safety measures and additional support for housekeepers/domestic workers within critical care. Having clear guidance as to responsibilities for clearing spills may be important as could training on the use of oxygen cylinders and syringe pump holders. There is an opportunity to develop footwear specifically for use in a critical care environment that would withstand roll over injuries and minimise slips.
Conclusion
In summary, the rate of self-reported staff injury in critical care has remained static between 2009 and 2013 ranging between 2.6 and 3.7 episodes/1000 patient days. This is despite the introduction of variable local, national and regional guidelines. Of all these incidents, assaults to staff have consistently contributed the highest proportion on thematic analysis.
The circumstances of these injuries are very poorly recorded and this prevents us learning from them. What information is available suggests that the rate of injuries could be significantly reduced by educational, practical and clinical interventions. Such interventions would need to be followed by further study cycles with the aim of cataloguing continual reduction in harm.
Footnotes
Acknowledgements
We would like to acknowledge the contribution of and the members of staff from the critical care units throughout the North West of England who were involved in highlighting, documenting and investigating reported incidents involving staff harm.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.