
Abstract
Objectives:
The objective of this systematic review was to synthesise literature pertaining to patient and family violence (PFV) directed at Intensive Care Unit (ICU) staff.
Design:
Study design was a systematic review. The data was not amenable to meta-analysis.
Data Sources and Review Methods:
Electronic searches of databases were conducted to identify studies between 1 January 2000 and 6 March 2023, limited to literature in English only. Published empirical peer-reviewed literature of any design (qualitative or quantitative) were included. Studies which only described workplace violence outside of ICU, systematic reviews, commentaries, editorials, letters, non-English literature and grey literature were excluded. All studies were appraised for quality and risk of bias using validated tools.
Results:
Eighteen studies were identified: 13 quantitative; 2 qualitative and 3 mixed methodology. Themes included: (i) what is abuse and what do I do about it? (ii) who is at risk? (iii) it is common, but how common? (iv) workplace factors; (v) impact on patient care; (vi) effect on staff; (vii)the importance of the institutional response; and (viii) current or suggested solutions.
Conclusions:
This systematic review demonstrated that PFV in the ICU is neither well-understood nor well-managed due to multiple factors including non-standardised definition of abuse, normalisation, inadequate organisational support and general lack of education of staff and public. This will guide in future research and policy decision making.
Introduction
Healthcare professionals are exposed to violence 16 times more often than in any other field of employment. 1 Violence is a serious workplace problem especially in public health, and in high-risk areas such as emergency departments, psychiatric wards and intensive care (ICU). 2 To add insult to (real) injury for staff, impetus for change has been thwarted by the 21st century emphasis in healthcare on public relations and customer-centred services at the expense of staff. 3
Workplace violence is defined pragmatically here as an incident where an employee is abused, threatened or assaulted by patients or their relatives or friends, in circumstances arising out of – or in the course of their employment, irrespective of the intent for harm. 4 This includes, but is not limited to physical violence and abuse (e.g., throwing equipment, hitting, kicking, grabbing) and non-physical violence (e.g., shouting and verbal abuse). 5 We note that this definition focuses on patient and family-perpetrated violence (PFV), unlike broader definitions of workplace violence which encompass violence perpetrated by fellow staff.6 –10 In this review we focus on PFV, which we consider a distinct phenomenon with distinct causes and solutions.
While PFV has increasingly received attention with implementation of a range of workplace interventions, these have been focused on nursing home, mental health and emergency departments, 11 with relative neglect of ICU despite its recognition as a high-risk setting. 3 While a systematic review 12 evaluated occupational violence and aggression in both urgent and critical care in rural health settings, it did not address ICU exclusively, thus obfuscating specific needs of the ICU setting.
Much of the research to date has focused on nursing staff, as evidenced by a cross-sectional study (n = 3416) of membership of the New South Wales Nurses and Midwives’ Association, among whom 85% experienced PFV. 13
This review was an attempt to shed light on this occupational hazard and to explore strategies to improve workplace safety. The modified research PICo (Population, Interest, Context) question was: How do we understand aggression displayed by patients and families towards staff in ICU?
The primary objective of this systematic review was to synthesise literature pertaining to patient and family aggression directed at ICU staff.
Methodology
The systematic review followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) protocol 14 and was registered with PROSPERO (CRD42023434566).
Search strategy
Electronic searches of databases including PubMed, Medline, PsycINFO, Embase and Emcare were conducted using mesh and tree text terms, designed to identify studies between 1 January 2000 and 6 March 2023. In addition to the database searches, other articles were identified from the reference lists of included papers and systematic reviews (see Supplemental File 1.1. for search terms). The search was limited to literature in English only. For literature in languages other than English, we attempted to find an English language version.
Eligibility criteria
Inclusion
Published empirical peer-reviewed literature were reviewed to identify studies of any design (qualitative or quantitative) which included workplace violence including assault and aggression of ICU staff (including nurses, allied health, doctors, ward persons, administrative officers) by patients and families.
Exclusion
Studies which described workplace violence outside of ICU were excluded unless ICU data was included in the paper. Systematic reviews, commentaries, editorials, letters, non-English literature and grey literature were excluded.
Study screening
Primary database search and manual screening was undertaken by the first author (VS), with subsequent rounds (including full paper screening) by all authors, with disagreement reconciled with consensus of all three authors (see Figure 1).
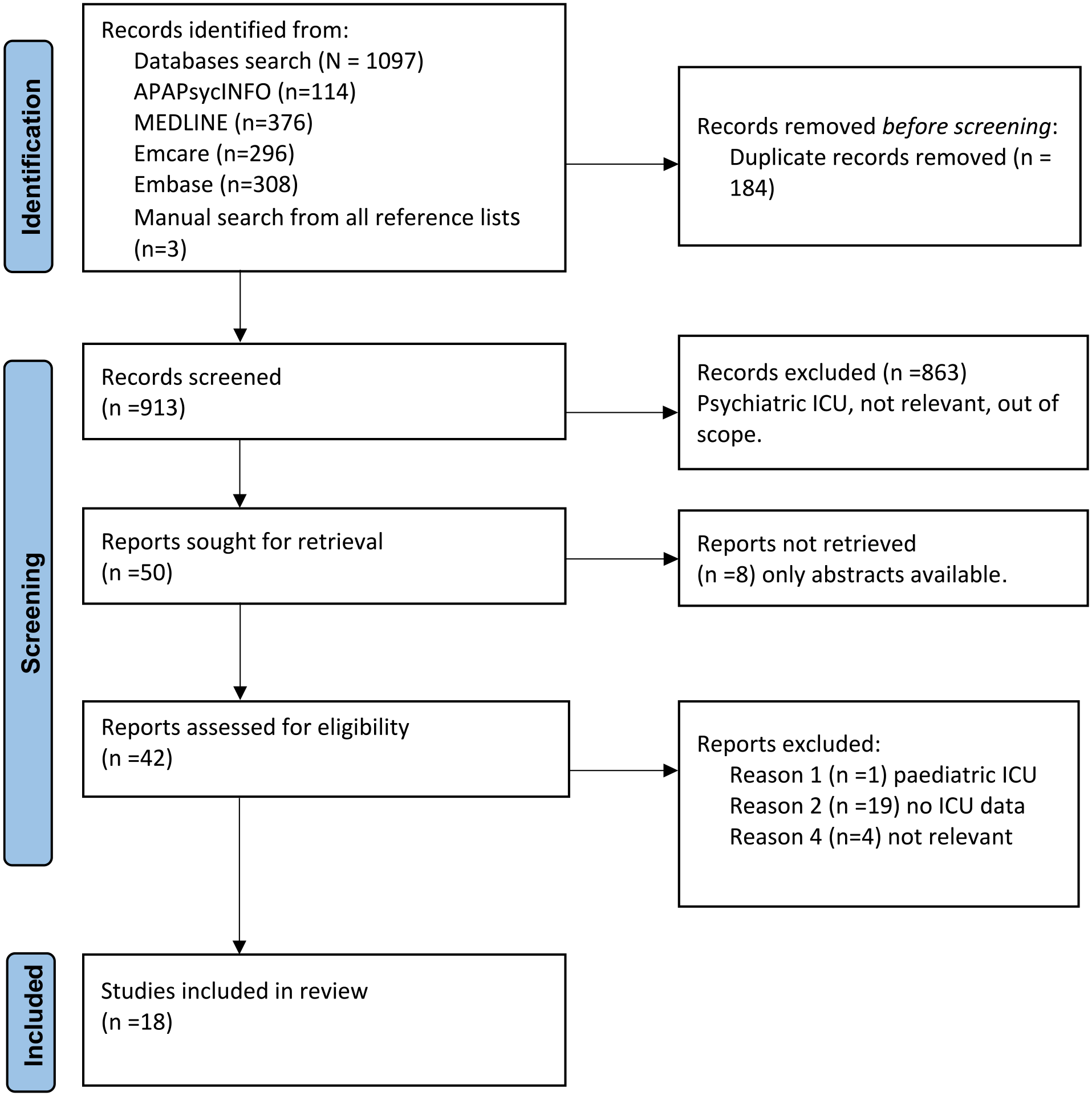
PRISMA flowchart.
Quality assessment
Included articles were independently assessed for quality and bias by authors VS and KL. Differences were resolved by discussion with author CP until consensus reached and final rating determined. Quantitative studies were appraised for quality using Alberta Heritage Foundation for Medical Research Standard Quality Assessment Criteria (KMET). 15 The checklist includes study design and appropriateness, method of subject selection, random allocation and blinding, outcome measures, statistical methods (including confounding and estimates of variance) and reporting of results and conclusions. A formula is used to derive a final rating score, expressed as a percentage, with >80% being generally considered as high quality in absence of any validated cut-off scores for quality.16 –18
Qualitative studies were rated using Attree and Milton (2006) checklist 19 inclusive of research aims and objectives, appropriateness of study design, sampling methods, data collection, analysis and results, reflexivity, value and usefulness of the study and ethical considerations. Each item is rated from A (no or few flaws) to D (significant flaws threatening the validity of the entire study), with the final quality score (A–D) determined by the majority grade.
Risk of bias was assessed using the Agency for Healthcare Research and Quality (AHQR) tool 20 which provides an overall bias rating of high, medium or low, based on the number of ‘yes’ or ‘no’ responses to each question in the rating tool.
Data extraction and synthesis
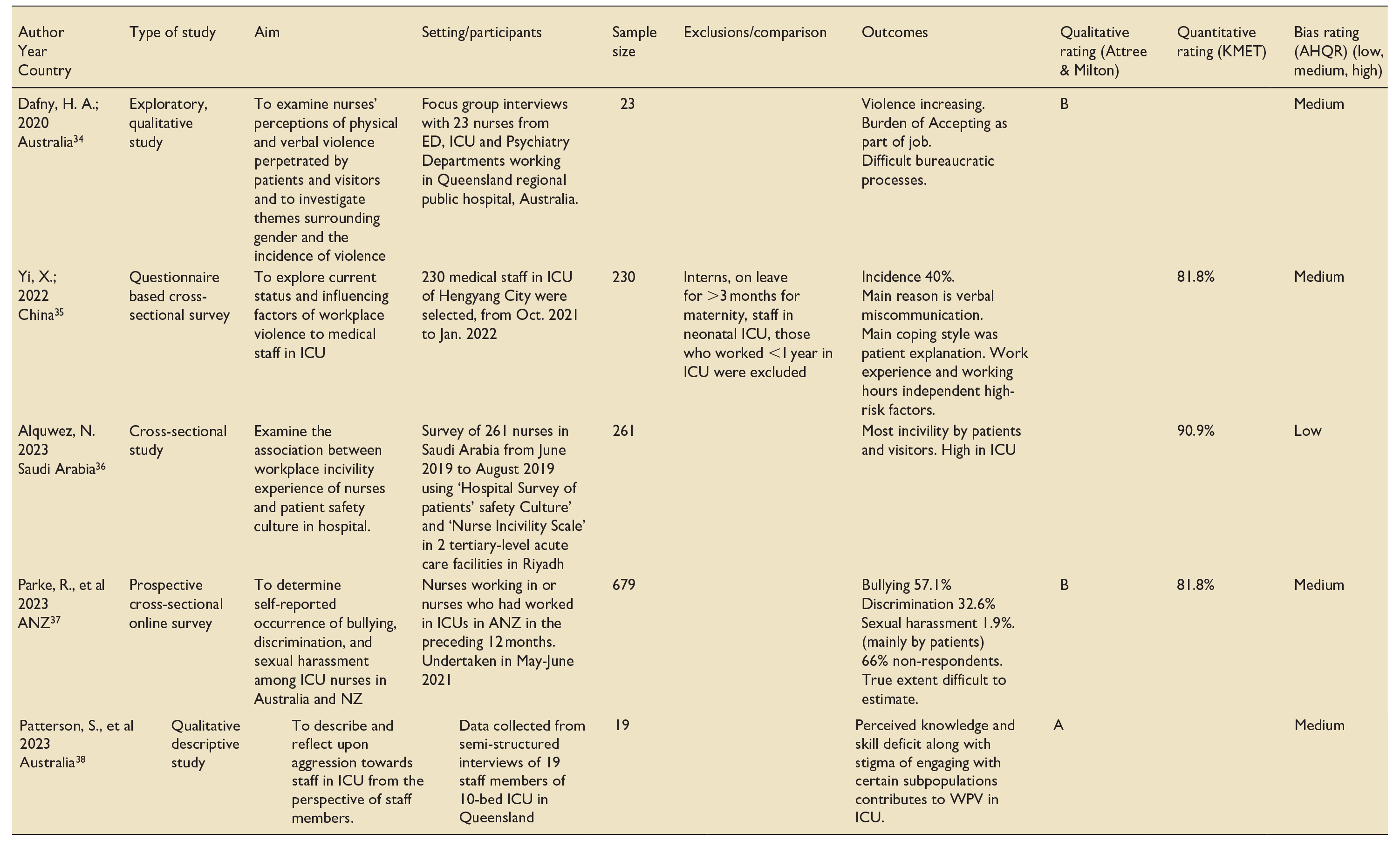
A table was created for the extraction of relevant data, including author details, year of study, country of study, characteristics of participants, study design, comparison group, outcome measures, risk of bias and methodological quality and score (Table 1).
Data extraction: Included studies.
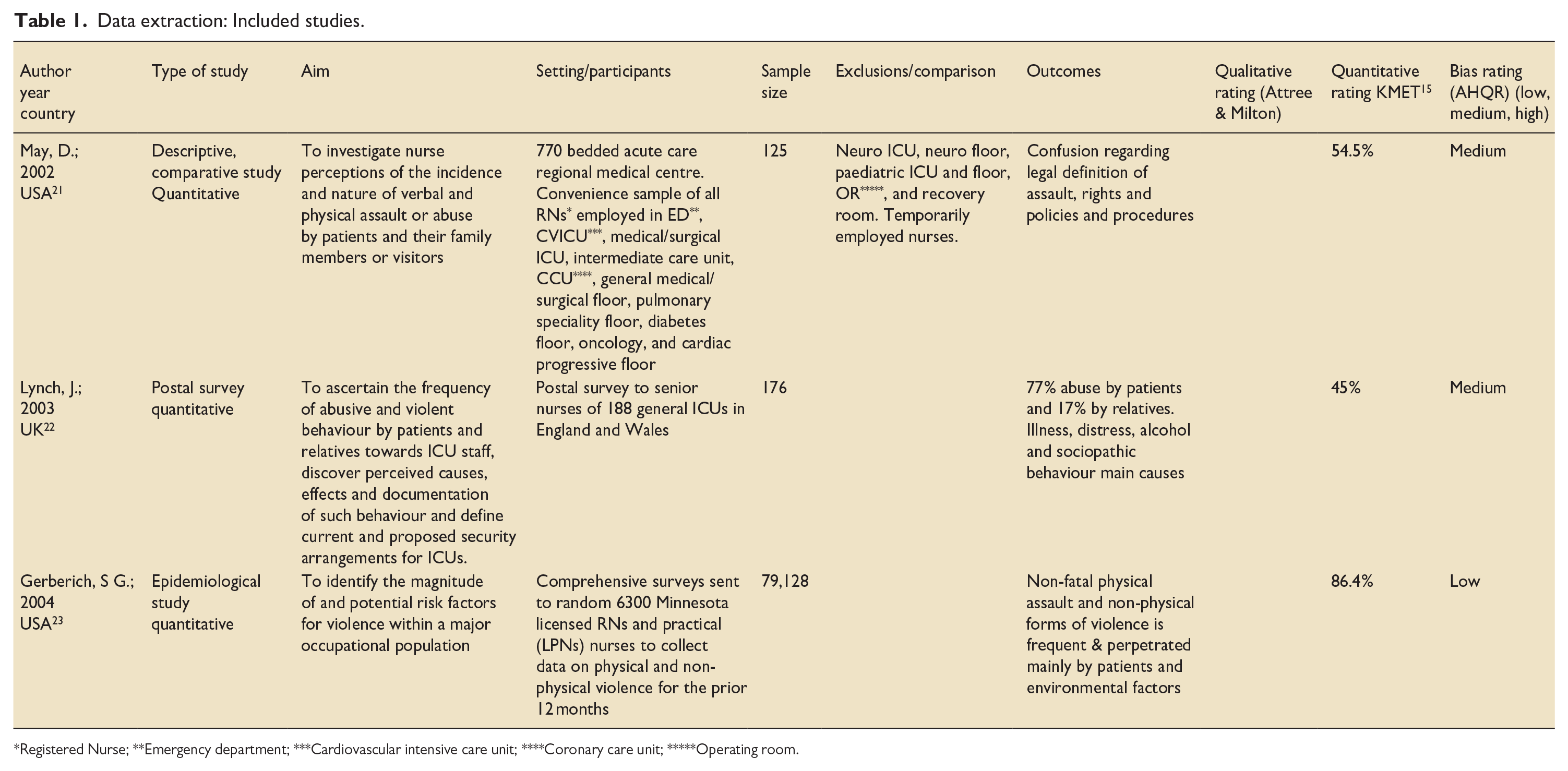
Registered Nurse; **Emergency department; ***Cardiovascular intensive care unit; ****Coronary care unit; *****Operating room.
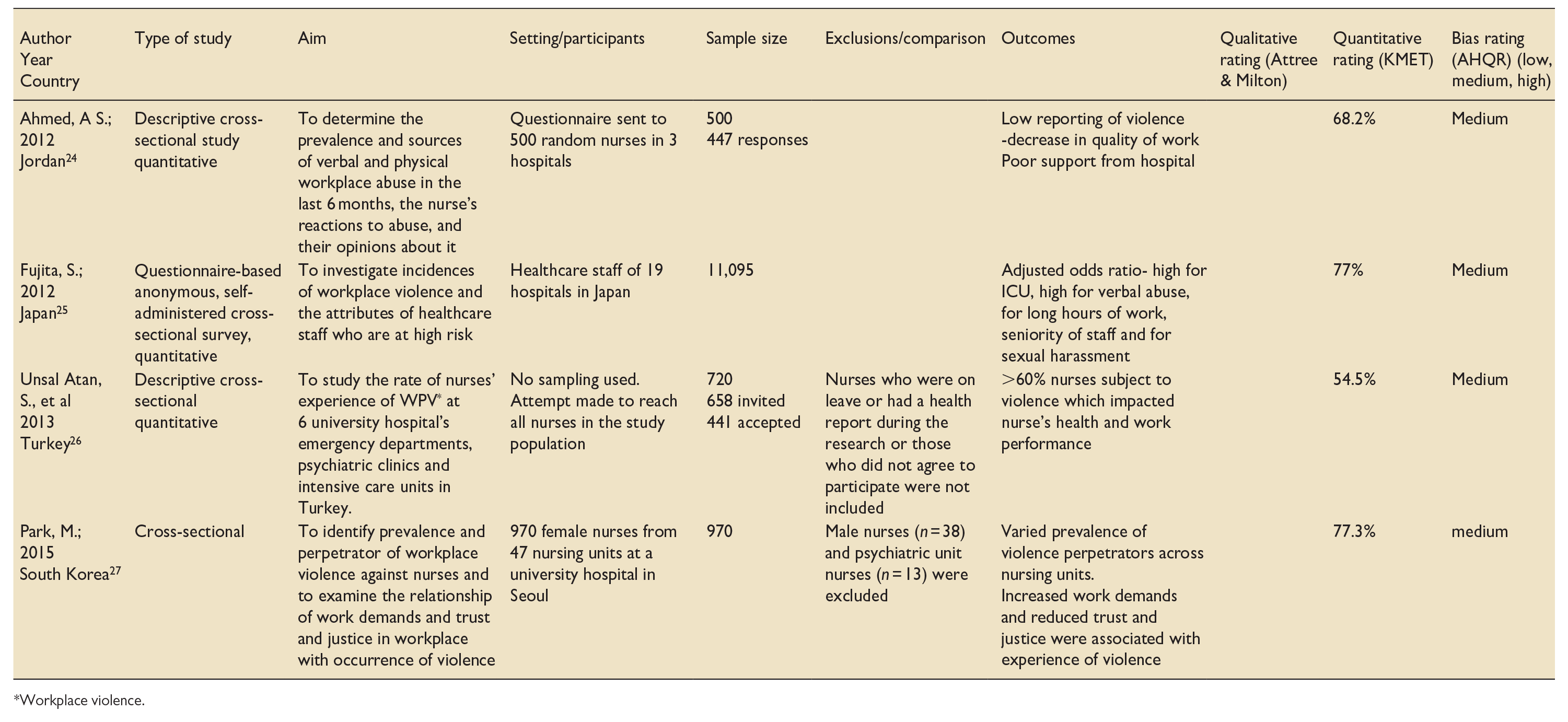
Workplace violence.
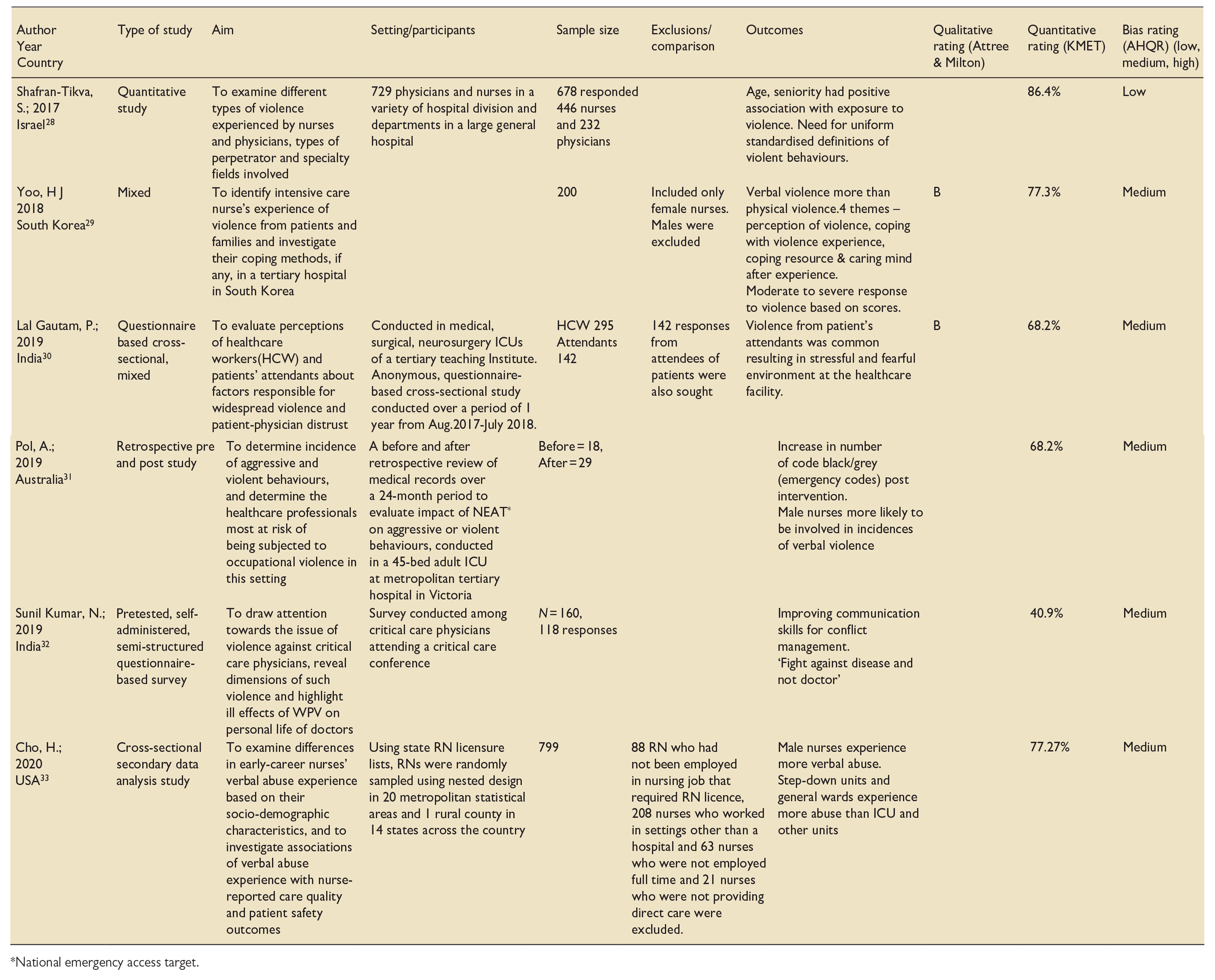
National emergency access target.
We used the method of thematic synthesis. VS undertook primary open coding of included texts (Results and Discussion). Subsequent development of descriptive themes, followed by consolidation and interpretation to generate analytical themes was undertaken by all three authors. 39
Statistician input was sought for feasibility of meta-analysis.
Results
This literature review included 18 studies: four from USA, three from Australia; two each from India, South Korea; and one each from China, Jordan, Turkey, Saudi Arabia, Japan, UK and Israel; with one combined study from Australia and New Zealand. Of the studies included, 13 were quantitative, 2 were qualitative and the remaining 3 mixed-method studies.
Of 18 included studies, 10 focused on nurses at various stages of their careers,21,23,24,26,27,29,33,34,36,37 7 on a range of workers including nurses, doctors and other hospital employees22,25,28,30,31,35 with one dedicated to doctors. 32 Only 7 studies focused only on ICU22,29,31,32,35,37,38 with the remaining 11 studies included various units in the hospital including ICU.21,23 –28,30,33,34,36
Of 18 studies included, 5 were rated high quality16,17,18 (>80%) using KMET quantitative rating; 7 scored between 60–80%, 4 studies between 40–60%. The three qualitative studies scored between A and B on Attree and Milton qualitative ratings. 19
Thematic synthesis yielded a number of themes which included:
What is abuse and what do I do about it?
The studies identified showed a lack of understanding, identification and recognition of PFV which was normalised or considered part of job.29,34,37,38 Several studies reported lack of standardised definition of what constitutes PFV, which can include ‘being kicked’, ‘pinched’, ‘spat upon’, ‘cursed at’, ‘yelled at’, ‘threatened with harm’ to ‘swearing’, ‘reviling’, ‘punching’, ‘scratching’, ‘throwing an object’.21,24,26,28,29 Similarly, studies showed poor understanding of legal implications of PFV including the differences between ‘assault’ and ‘abuse’, and reporting policies and procedures.21,26,37
It is common, but how common?
Determining the prevalence of PFV is constrained by this lack of definition. Studies suggested that verbal abuse was the most common form (50–90%) of aggression.21,22,24,26 –30,32,33 Main perpetrators were male patients followed by visitors or carers.23,24,35
Who is at risk?
ICU nurses, who work around-the-clock at patient bedsides, experience more PFV. 28 Several studies suggested the prototype victim of PFV was a female nurse,14,15,19,22 –26,28,30,33 with proposed reasons including maternalistic attitudes towards patients,22,24,28 and the gender bias for sexual harassment.21,22,24,28,38 In contrast, one paper suggested that male nurses experienced more PFV because they were perceived as bodyguards. 34
Three studies28,33,35 reported an association between seniority and experience of PFV, although the reasons for this are unclear. On the one hand there was a positive association between doctors’ rank and exposure to PFV; yet being older reduced risk for both doctors and nurses. 28
Patient factors
ICU is an area which provides high quality care for very sick patients, and uncertainty of recovery adds to stress of families and staff equally but for different reasons. Notably, with regards to potential sources of family stress, staff perceived that patients with unexplained conditions, poor prognosis, extended hospital stays, unexpected complications and unexpected deaths were responsible for aggression. 30 Admission from ED to ICU with a variety of diagnoses and acuity of illness was also associated with more aggression. 31 Patient mix, specifically absence of adult male patients influenced PFV. 25 While staff (nursing staff) perceive causes of patient violence to be related to ‘distress’ ‘alcohol or illegal drugs’ ‘psychiatric illness’ and ‘sociopathic personality’, 22 no studies reported psychiatric assessments or diagnoses of aggressive patients.
Workplace factors
A range of workplace factors appeared to be related to PFV. PFV occurred most frequently on night shifts 30 and in settings with higher work demands (workload), staff (nursing) shortages, higher hospital costs24,30,37 leading to higher levels of stress for the families, and public, metropolitan and level 3 ICUs. 37 Workplace practices including longer working hours, constant and direct interaction with patients, posed risks for all types of aggression including physical aggression, verbal abuse and sexual harassment. 25 Lack of staff training causing skill and knowledge deficits was also evident with staff reporting feeling ill-prepared to work with aggressive patients, whose management they relegated to mental health services. 38
Impact on patient care
This was minimally studied. One study found that PFV was significantly associated with negative perceptions of unit-level patient safety 36 ; another study reported that junior nurses who experience verbal abuse are less likely to report high-quality care and favourable safety ratings. 33
Effect on staff
Negative impacts of PFV on staff wellbeing and work productivity and quality were wide-ranging. Psychological effects ranged from psychological and somatic symptoms to frank mental health disorders such as Post Traumatic Stress Disorder and Depression with impact on family life and social life.23,24,26 Occupational effects included increased sick leave, decreased job satisfaction, consideration of quitting the profession and attrition of staff.24,26
The importance of the institutional response
Inadequate support from management was noted in 9 of 18 studies identified.22,26,29,30,31,33,34,37,38 PFV in the ICU had a significant effect on perception of employer or organisation with effects of inaction including distrust 34 and an expressed need for legislation to tackle PFV. 32 There was strong agreement among studies that more concerted efforts from organisations was required to work towards employee satisfaction, increased public awareness and upskilling and supporting staff in dealing with PFV.24,26,29,30,32,34 There was perception of overemphasis on the institution and patient rights over that of employees. 21
Current or suggested solutions
Many remedies were proposed including education of staff and general public, improved reporting of incidences, better security, Code Black teams (emergency response team for aggressive behaviour), restricted access to the ICU for visitors.21,29,30,31,32,33,36 ‘Zero Tolerance Policy’, ‘Hospital Protection Act 2008’ and Doctor’s Protection Act 2010 in India were legislative solutions.30,32
Discussion
In this systematic review we synthesised the available literature on aggression displayed by patients and families towards staff in the ICU. As far as we are aware, this is the only systematic review on this topic. The representation of studies across the USA, Australia, South Korea India, China, Japan, Saudi Arabia, Turkey, Israel and UK suggests that this is global problem not limited to certain cultural settings, although in the absence of cross-cultural studies, we do not know how culture influences either manifestations of aggression or solutions. The quality and bias ratings, paucity of studies on crucial issues such as patient diagnoses contributing to aggression, and the impact of PFV on patient care, and general lack of amenability of the data to meta-analysis suggests that this is an under-researched topic. Notwithstanding this, the richest source of data lay in the qualitative studies. Our thematic synthesis yielded a number of observations, many of which posed further questions. These included: (i) what is abuse and what do I do about it? (ii) who is at risk? (iii) it is common, but how common? (iv) workplace factors;(v) impact on patient care (vi) effect on staff; (vii) the importance of the institutional response; and (viii) current or suggested solutions.
One of the most troubling observations is that this global problem in healthcare is common, but its proper documentation remains elusive. According to the World Health Organization (WHO) Attacks on Health Care Intiative 2019–2022, of 594 reported attacks on healthcare workers resulting in 959 deaths and 1561 injuries in 19 countries, 62% intentionally targeted healthcare.40,41 While this may be a global problem, it is a problem undefined, and therefore unstudied and unsolved. Lack of international consensus of definition of PFV, in both legal and clinical contexts provides an impediment to both reporting and data collection, as well as remedy in raising staff awareness and garnering adequate systemic responses including prosecutions where appropriate. Future research might be directed to international collaboration on recognising and tackling PFV, with first steps being a consensual definition of PFV to improve epidemiological understanding of PFV. What is also needed is collaboration with our legal colleagues, starting with a review of prosecutions in this space.
While the literature shows tentative links between PFV and patient safety and quality, there is no doubt about effects on staff welfare and productivity. Echoed in other more general studies of workplace violence in healthcare settings, failure to address the problem has consequences both for staff in terms of psychological and physical harm, but also for the facility, mediated by job satisfaction, job commitment, sick leave, staff turnover, and associated economic costs. 42 The Price-Muller Turnover Model 43 indicates that organisational commitment has a mediating effect on relationship between job burnout and turnover intention, with higher burnout scores associated with stronger turnover intention.44 –46
We have identified a number of putative risk factors for PFV that warrant further empirical investigation of odds ratios for aggression, in order to inform prevention strategies. It was found that nursing occupation, female gender, junior ranking, long-working hours were potential risk factors for PFV. The main perpetrators were male patients followed by visitors or carers. Patient complexity and poor prognostic factors that likely fuel family stress and accordingly aggression, are likely important but need further examination. Moreover, better understanding of patient variables such as delirium and psychiatric diagnoses is also required. Further to the issue of international consensus, collaboration and data gathering, a potential model for taking this area of research forward can be found in the Sprint National Anaesthesia Projects (SNAPs) conducted not only in the UK, but in Australia and New Zealand. Although craft-specific, the SNAPs capture data related to commonly occurring phenomena over a few days, then analyse and report on the data in peer-reviewed papers in clinical journals. 47
It was generally found that there was a lack of institutional support or policies dealing with PFV. Or even if these were in place, they were either unknown or difficult to navigate. Organisations need to consider their health and safety obligations and duty of care to staff in this context of harm and Post Traumatic Stress Disorder, 48 with particular attention to the workplace factors that either promote or mitigate against risk for PFV, including policies such as family access and visitation policy 49 and unit size and design ensuring visibility of care and emergency exits. 50 These systemic changes needed to be echoed by political will for change including legislation enforcing both remedy and penalty.51 –53
A range of targets for staff training have been identified here and elsewhere. These include staff training on topics such as patient and family communication skills, trauma-informed care, de-escalation skills and resilience training.54 –57 Although identified in emergency departments, but of equal relevance here, is the need for accessible experiential training in de-escalation.58 –60 Further to education and support, collaboration between ICU and mental health utilising novel initiatives such as a liaison-psychiatrist embedded within the ICU 61 might be pursued.
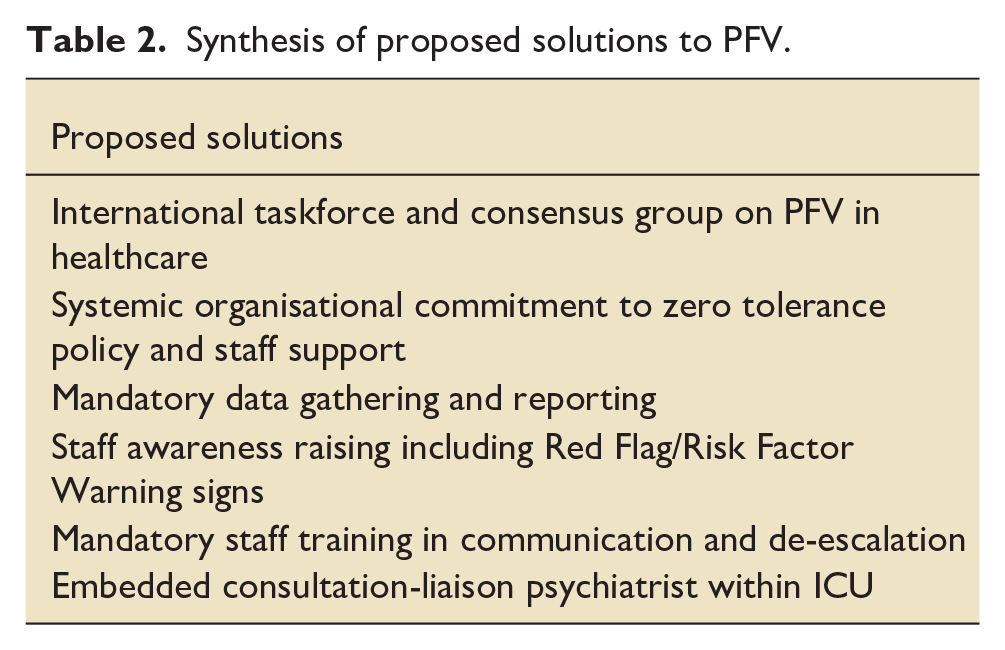
We summarise the solutions proposed in Table 2.
Synthesis of proposed solutions to PFV.
Limitations
As with any systematic review, there is inherent limitation in terms of missed literature due to exclusion of grey literature, non-English literature, editorials and letters. Further, subsequent to completion of the review, relevant studies meeting eligibility criteria may have been missed. Another factor effecting the quality of the systematic review is the quality of the included studies, with highest quality found in qualitative studies, with quantitative not amenable to meta-analysis. Consistent quantitative data across several studies was lacking. For example, assault incidence was mostly reported as anecdotal survey data only, with quantified assault rates – for example, assaults per bed per day – insufficiently reported for meta-analysis. We considered requesting a measured assault rate from study authors for meta-analysis purposes but acknowledge that data was unlikely to be available to them without information on the rostering of each survey respondent. Rather, richness of data lay with the qualitative perceptions and experiences of healthcare professionals. As such, this study focused on a thematic synthesis of the literature.
Conclusion
This systematic review included 18 articles that met eligibility criteria out of a potential 1097 identified from searches. It appears that PFV is commonly encountered by ICU staff particularly nursing staff, but otherwise we know very little about its epidemiology and risk. Although the past decade has seen a shift towards addressing this widespread occupational hazard, it has neither been sufficient nor effective in addressing occupational safety. Given the normalisation by staff that FPV is part of the job, perhaps a starting point from the organisation down is to say it is not part of the job, and to echo a zero-tolerance policy, internationally.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241231707 – Supplemental material for Understanding aggression displayed by patients and families towards intensive care staff: A systematic review
Supplemental material, sj-docx-1-inc-10.1177_17511437241231707 for Understanding aggression displayed by patients and families towards intensive care staff: A systematic review by Varadaraj Sridharan, Kelvin CY Leung and Carmelle Peisah in Journal of the Intensive Care Society
Footnotes
Acknowledgements
Authors would like to acknowledge Ms. Tracy McDonald and Ms. Claire Ambrose, Librarians at Cumberland Hospital, Westmead for their immense help in sourcing the articles, education with use of Endnote, OVID search engine and for being available at short notices to address the most trivial of queries; and James Elhindi – statistician at Research and Education Network, Westmead Hospital for providing input on feasibility of a meta-analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.