
Abstract
Three-dimensional (3D) sonography is a valuable imaging technique to evaluate the uterus and distinguish the different types of congenital uterine abnormalities. The provided case series demonstrates the unique diagnostic patient findings of a bicornuate uterus and an incompetent cervix. The patient presented over a series of multiple pregnancies that used cervical cerclage, to achieve an improved maternal-fetal outcome. In this patient, her uterine anomaly was diagnosed prior to pregnancy. During each gestation, close diagnostic attention was paid to the shape of the uterus, the location of the gestational, and the cervical length, by using transvaginal sonography. This imaging surveillance played an important diagnostic role in providing a better patient outcome for the patient’s multiple pregnancies. Continued research into the use of 3D sonography, for this specific diagnostic application, is needed to accelerate its use in determining the specific location of gestational sac(s).
Müllerian ducts are the structures responsible for the development of the upper two-thirds of the vagina, cervix, uterus, and fallopian tubes. 1 The development of the genital tract begins during the third week of pregnancy and carries into the second trimester. Crosby et al. were the first to propose that the fusion of the two Müllerian ducts, which starts at their caudal ends in the Müllerian tubercle and proceeds cranially up to the fundus. Various types of uterine, cervical, or vaginal anomalies result from failure of the duct to develop appropriately, while absent or incomplete fusion results in uterus didelphys. 2 The congenital uterine abnormalities are classified into six groups based on their prognosis for future fertility and surgical correlations.
Class I. Segmental Müllerian agenesis or incomplete vaginal canalization is suspected when a young girl reaches puberty without menses.
Class II. Unicornuate uterus, which is related to infertility and pregnancy loss, sonography demonstrates a uterus that is long and slender (cigar-shaped) and deviated to one side.
Class III–V are more challenging to diagnose because they all have two uterine cavities, and their correlation classification and treatment depend on the appearance of the external contour of the uterine fundus.
A congenital malformation is often challenging to demonstrate during the nongravid state and may mimic a fibroid. A class III is designated by a uterine didelphys, which is a complete duplication of the uterus, cervix, and vagina. This condition is not usually associated with fertility problems and does not generally require treatment. 3 Sonography can be used to detect two endometrial echo complexes, which are best demonstrated during the secretory phase of the menstrual cycle, when the endometrium is most prominent. A class IV is highlighted in the current case study, as the bicornuate uterus appeared as a duplication of the uterus with a common cervix. The bilobed uterine cavity has wide-spaced cavities and a low incidence of fertility complications and is usually not treated. 3 A class V would involve a septate uterus in which two uterine cavities are closely spaced, with one fundus and sometimes two cervical canals or a vaginal septum. This condition has the highest incidence of rate of infertility, and the septum may be removed by a hysteroscopic approach. 3 A class VI is related to exposure to the drug diethylstilbestrol (DES) in utero. The uterus is normal in size and shape externally; however, the cavity is “T” shaped with an irregular contour. This condition may be challenging to diagnose with sonography. Although congenital uterine abnormalities exist, some Müllerian duct anomalies (MDAs) can have normal reproductive outcomes. 3
The use of transvaginal sonography, in evaluating the cervix, has been addressed in the literature by Anderson. He emphasized that the endovaginal approach gives more detailed imaging of the cervix than the standard abdominal approach. 4 According to a study by Bega et al., information regarding cervical morphology tends to be lost when relying on two-dimensional (2D) imaging, only for cervical length. Three-dimensional (3D) volume imaging has created a plausible methodology to verify and enhance these 2D measurements. 5 Early detection of the short cervix, during sonography, is the primary diagnostic tool used by sonographers and clinicians to provide improved patient outcome. While the patient, in this case study, presented experienced difficulties in receiving prenatal care, a combination of early transabdominal and transvaginal sonograms were used to assess gestational location, and cervical length. These sonographic diagnostic assessments were performed in each of her four pregnancies and resulted in improved outcomes. A combination of 3D sonography and a transvaginal sonogram, during the first trimester, were highly effective for this patient. More evidence is needed to accelerate the adoption of this diagnostic tool for determining which cornua the gestational sac occupied for each successive pregnancy. A summary of each of the patient’s pregnancies is provided in the case report.
Case Report
A 43-year-old female, G4P4, was diagnosed with a bicornuate uterus before her pregnancies and presented to the emergency department (ED) with flank pain and left lower quadrant pain, which started in the morning and worsened throughout the day. The patient reported no nausea, vomiting, or diarrhea, no fever or hematuria. Upon admission to the ED, the physicians requested a transabdominal and transvaginal sonogram, as well as a renal and urinary bladder sonogram. The transabdominal and transvaginal sonograms were performed with a Logiq E9 ultrasound equipment system (GE Medical, Waukesha, WI) and a C1-6 curved-array transducer to assess the uterus, ovaries, kidneys, and urinary bladder. The sonogram revealed normal-appearing bilateral kidneys with no evidence of hydronephrosis or nephrolithiasis. The urinary bladder appeared fully distended with a standard thin bladder wall. The uterus appeared to have two horns previously diagnosed by regular 2D sonogram. The ovaries were normal, the right ovary measured as 2.3 × 1.7 × 2.1 cm3, with an estimated volume of 4.5 ccs. The left ovary was measured as 2.6 × 1.8 × 2.5 cm3, with an estimated 6.0 ccs. The vasculature was normal appearing in both ovaries, with no sonographic features of ovarian torsion. The 3D sonogram was performed to view the uterine cavity and distinguish the type of uterine anomaly. Figures 1 and 2 demonstrate the sonographic view of two endometrium cavities. These sonograms highlight the number of horns, and whether there is a septation.
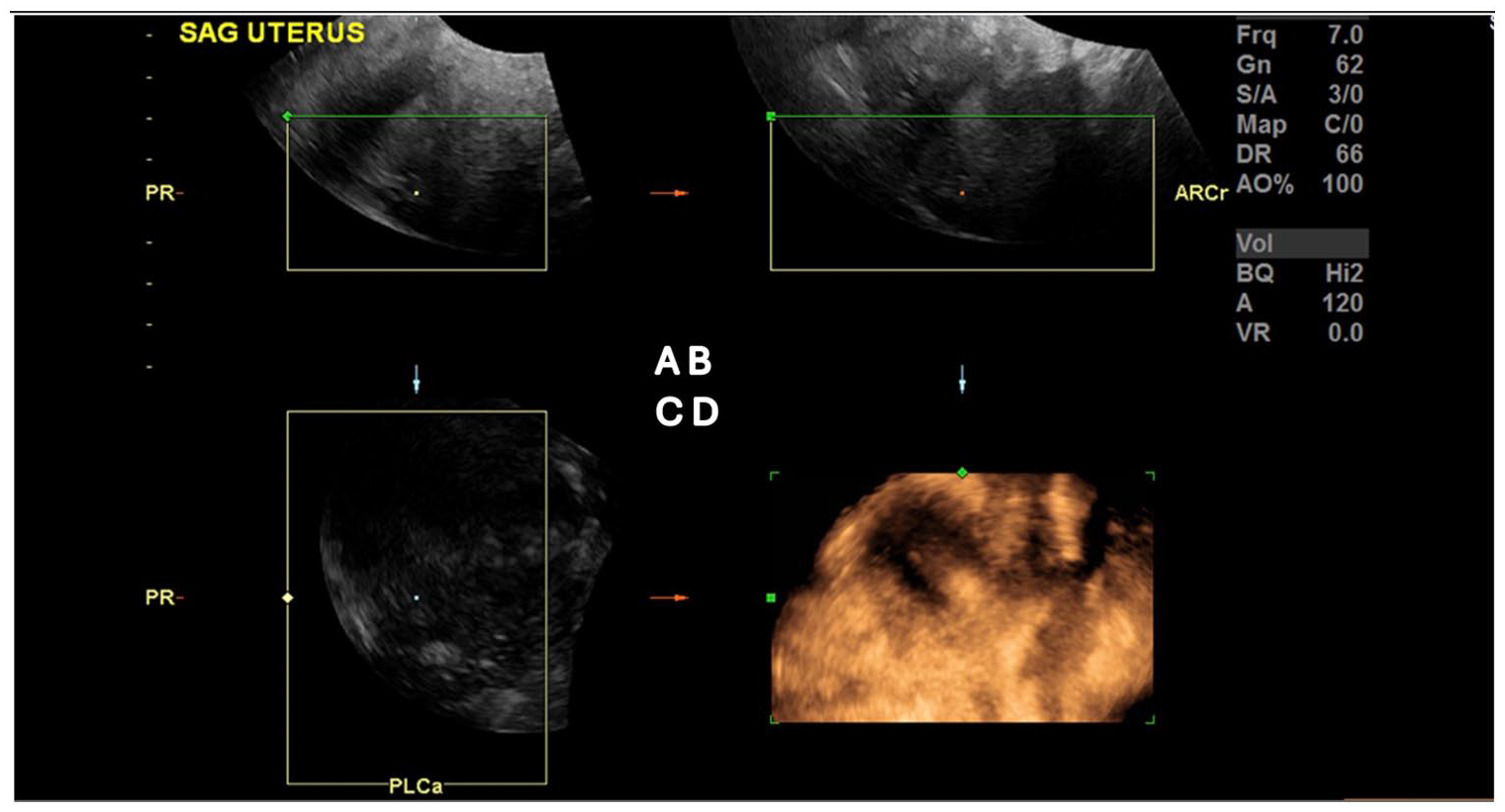
The procedure to obtain a rendered image of a Mullerian anomaly, in this case of a bicornuate uterus. (A) The initial plane for obtaining three-dimensional (3D) volumes was generally mid-sagittal (Window A). Acquisition was carried out with a sweep angle of 90°. The image corresponds to the bisector of the angle made by the volumetric transducer as it is moved from one side of the uterus to the other. Window B is the axial plane and Window C is the coronal plane. (B) The rendering box was then adjusted (Window A) and the green line adapted to the curved plane of the uterine cavity, so it become positioned on the endometrium. The midline was verified (Window B). In the bottom right is the rendered image obtained from an axial plane (Window A) so that both horns would fit in the same field of view, enabling the cavity/fundal relationship to be better established, in the 3D reconstruction (see bottom right).
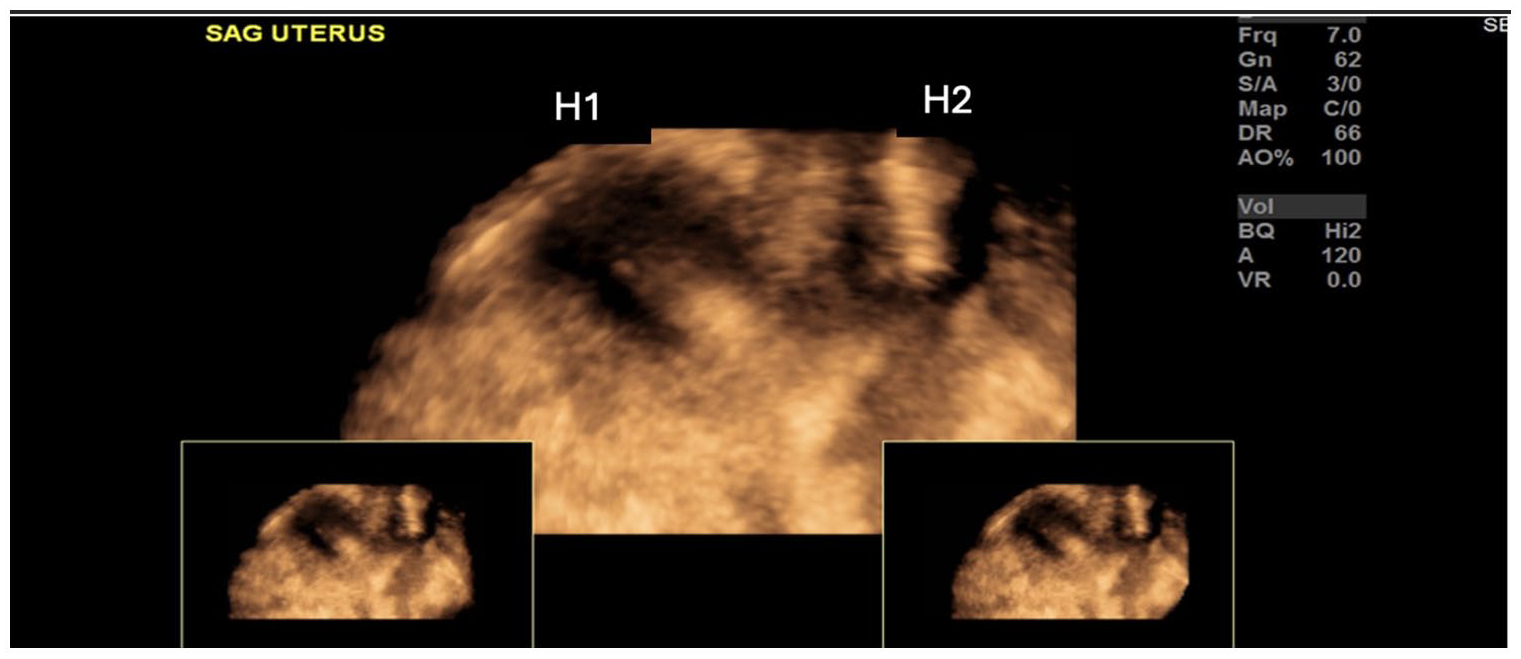
The three-dimensional (3D) sonogram was used to better demonstrate the two horns of a this bicornuate uterus. The horns are indicated on the image by H1 and H2.
Patient’s First Pregnancy
The patient’s first pregnancy was sonographically detected as viable that included a single fetus, located on the right horn (See Table 1). Owing to patient’s circumstances, there was no diagnostic first-trimester sonogram completed (See Table 2). The patient’s sonographic fetal survey examination was limited and completed in the third trimester. The fetal gestational age was measured to be 32 weeks and six days, with an additional diagnostic finding of oligohydramnios. By 13 weeks of gestation, the patient presented to the ED with spotting and was diagnosed as having a short cervix; however, there was no sonographic report available. A cerclage was placed the following week to mitigate the risk of preterm birth, and the patient was given dexamethasone. During the period of 16 to 36 weeks gestation, the patient was taking hydroxyprogesterone caproate (500 mg) weekly, to lower the risk of preterm birth, as well as completing a course of betamethasone, at 28 weeks gestation. Owing to the estimated fetal weight being larger than expected and a reduction in the amniotic fluid index (AFI), based on the initial sonogram, a cesarean delivery (C-section) was planned and performed by 38 weeks gestation (See Table 1). The C-section was performed with spinal anesthesia, upon patient consent and explaining the procedural benefits and risks. The patient understood the risks and agreed to having her first delivery surgically. A healthy living infant was delivered, and both were discharged together, two days after delivery.
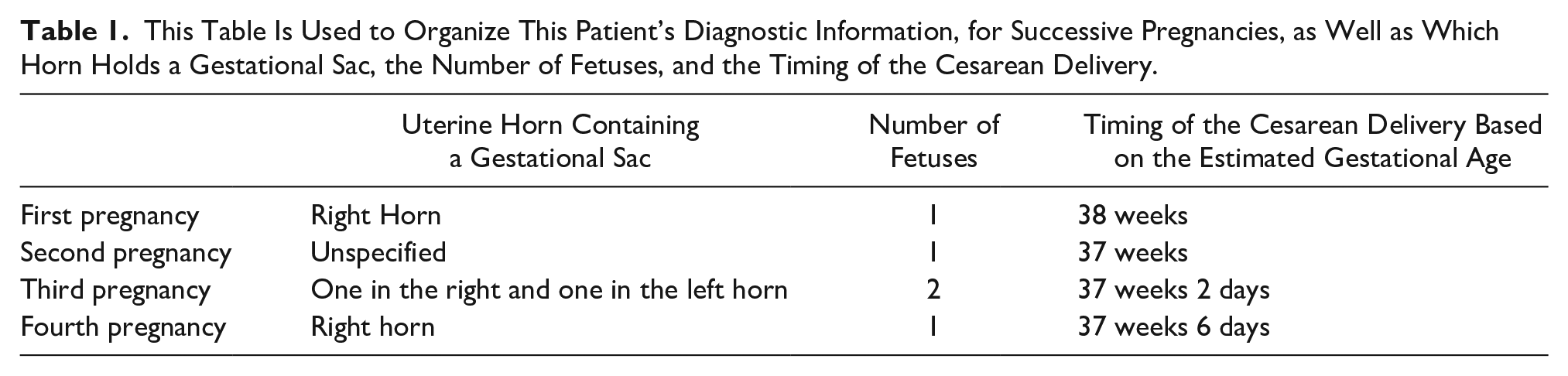
This Table Is Used to Organize This Patient’s Diagnostic Information, for Successive Pregnancies, as Well as Which Horn Holds a Gestational Sac, the Number of Fetuses, and the Timing of the Cesarean Delivery.
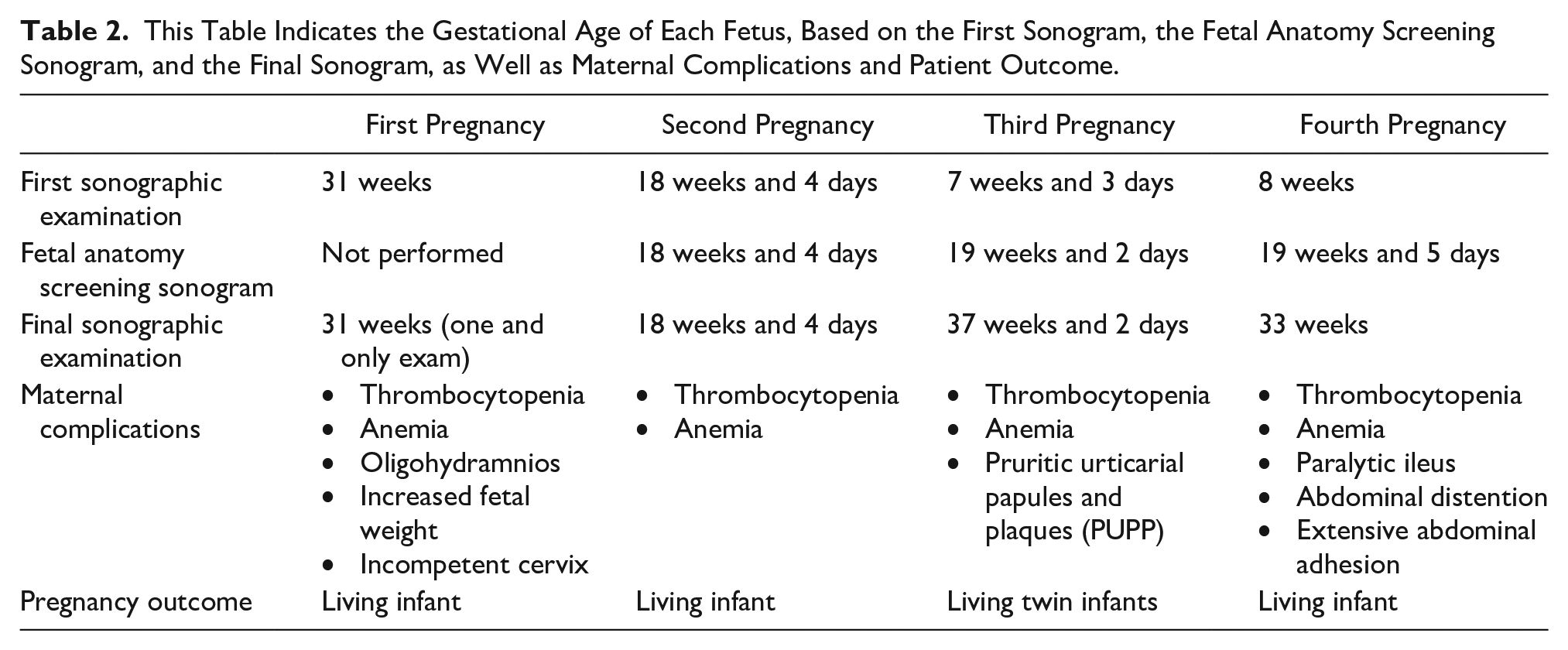
This Table Indicates the Gestational Age of Each Fetus, Based on the First Sonogram, the Fetal Anatomy Screening Sonogram, and the Final Sonogram, as Well as Maternal Complications and Patient Outcome.
Patient’s Second Pregnancy
Two years later, the same patient had a second singleton pregnancy, but in an unspecified uterine horn. She prophylactically had a cervical cerclage placed, after 13 weeks of gestation. The cerclage was placed due to her history of a short cervix and the previous history of a threatened preterm labor. Her initial sonogram at 18 weeks four days gestation was unremarkable. She was considered a high risk for this second pregnancy due to her current history of thrombocytopenia, anemia after C-section, and a bicornuate uterus. During this pregnancy, the patient’s platelet count dropped from 148 000 to 116 000. As noted (See Table 1), her repeat C-section was performed at 37 weeks, with spinal anesthesia. The delivery was completed with a healthy infant being delivered and mother and infant were discharged, on second day of admission.
Patient’s Third Pregnancy
The patient’s third pregnancy was considered a dichorionic diamniotic (Di-Di) set of twins, with one fetus in each uterine horn. The first-trimester sonogram, for this pregnancy, was completed at 7 weeks and 3 days of gestation (See Figure 3). Each gestational sac contained their own yolk sac. The crown-rump length (CRL) and heart rate were measured for each fetus and represented a viable pregnancy (See Figures 4 and 5). A repeat sonogram was performed at 11 weeks and two days of gestation (See Figure 6). At this time, the fetuses were measuring 3.79 cm, and 4.53 cm, which corresponds to 11 weeks and two days of gestation (estimated date of delivery [EDD]: 10/05/2018). The fetal anatomy sonogram was competed at 19 weeks and two days. At that time, the cervical length, by transvaginal sonogram, measured 4.39 cm, which was sufficient to avoid the placement of a cerclage. Instead, routine surveillance sonography was performed to monitor the cervix at 25, 29, 33, 35, and 37 weeks of gestation. As the patient had a history of two prior C-sections, an incompetent cervix, thrombocytopenia, anemia, and pruritic urticarial papules and plaques (PUPP), a repeat cesarean, with spinal anesthesia, was completed at 37 weeks and two days. A positive outcome was noted as the patient and both healthy living twins were discharged on the second day of admission.
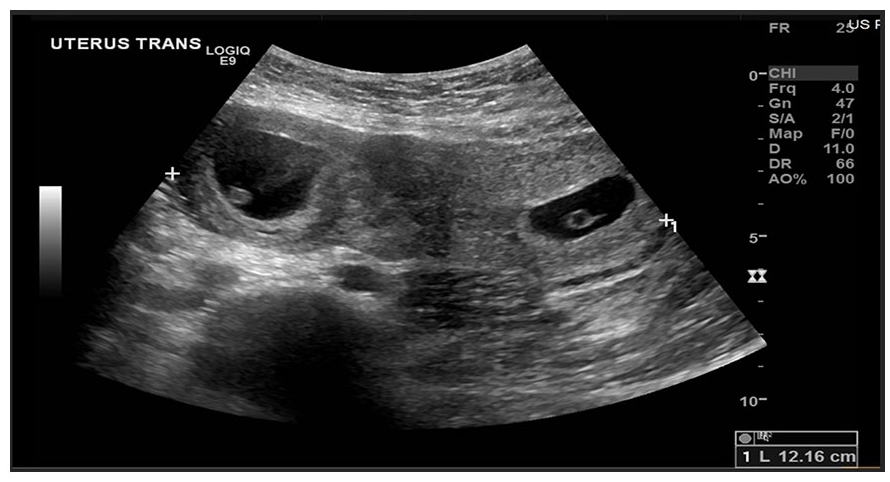
A bicornuate uterus with two gestational sacs and separate yolk sacs were noted on the first-trimester transverse sonogram (7 weeks and 3 days of gestations). Each gestational sac occupies one uterine cornua. The width of the uterus is indicated on this transverse view and corresponds to 12.16 cm.
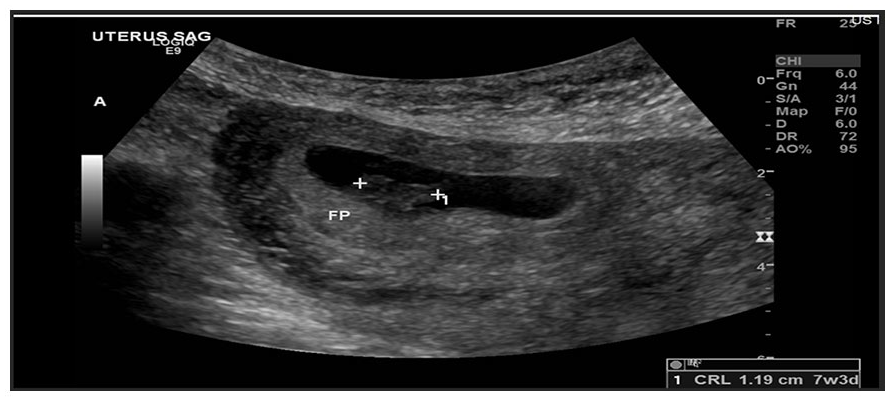
This sagittal sonographic view of the uterus demonstrated a gestational sac and fetal pole. The crown-rump length measurement is indicated based on the electronic calipers. The crown-rump length measurement of 1.19 cm correlated to a gestational age of seven weeks and three days.
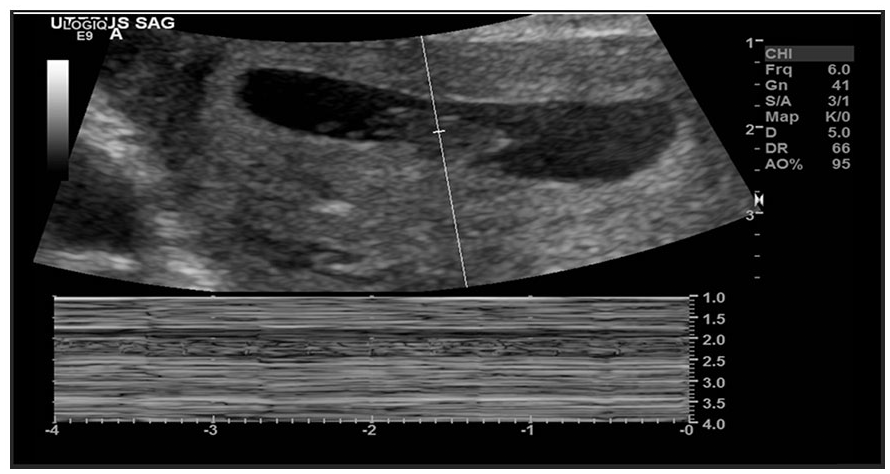
As part of the first-trimester sonogram, an active cardiac tracing was captured via M-mode and was part of the first-trimester sonographic protocol.
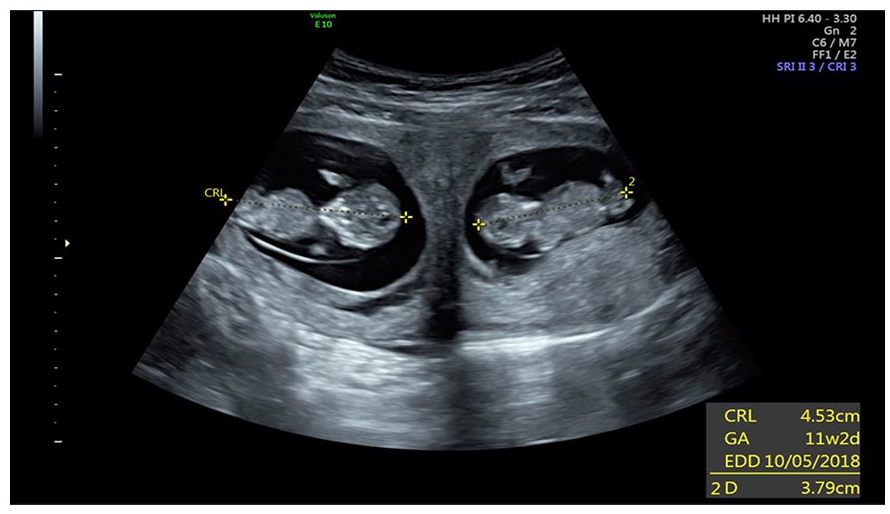
A repeated sonogram completed at 11 weeks of gestation, documented twin living fetuses. This transverse transabdominal sonogram demonstrated a fetus with a crown-rump length (CRL) measurement of 4.5 cm, which corresponded to 11 weeks and two days. The second fetus and gestational sac were located closer to the uterine cervix and the CRL measurement was 3.79 cm.
Patient’s Fourth Pregnancy
The same patient returned with a fourth and final pregnancy that was in the right uterine horn (See Figures 7 and 8). The first sonogram of this pregnancy was performed in the clinic, at eight weeks of gestation. The CRL was measured at 1.65 cm, corresponding to eight weeks and 0 days (EDD: 11/30/2021). Her sonographic fetal survey examination was performed at 18 weeks and six days of gestation and demonstrated a normal appearing fetus, in utero. The patient had a repeat appointment, in the clinic, four days after the sonographic fetal survey. To monitor the viability of the fetus and the cervix length, the patient had regular clinic visits at 24 weeks, 33 weeks and six days, 35 weeks and six days, and 38 weeks and two days, respectively. Her cervical length was maintained and measured 5.14 cm, which negated the need for cerclage. A repeat C-section was recommended due to the patient’s prior history and the fetus being in transverse position (fetal head to the maternal right); therefore, the delivery was performed at 37 weeks and 6 days. The result was the safe birth of a healthy living infant; however, the patient developed abdominal distention, paralytic ileus, and gestational thrombocytopenia, with extensive abdominal adhesions. The patient’s hemoglobin dropped to 7.9 and she was symptomatic. Owing to the abdominal distention, the patient was hospitalized and hydrated with intravenous (IV) saline and potassium chloride (KCL) supplementation, through the same IV line. In addition, the patient was advised and instructed to follow a soft diet plan. As for the anemia, two units of packet red blood cell (PRBC) were given. Platelets stayed within a normal range continuously and the abdominal distention resolved. The patient was discharged with the infant on the third admission day with a good patient outcome.
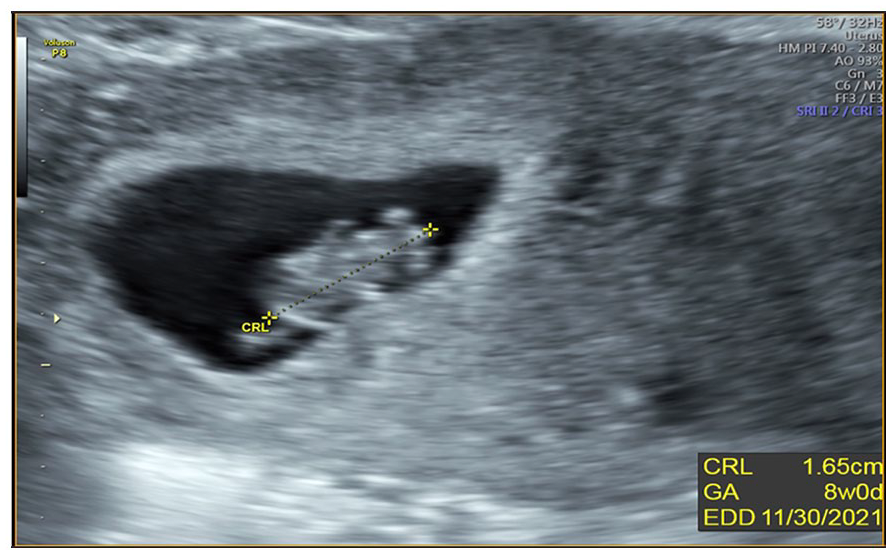
A sonographic demonstration of an intrauterine pregnancy in the right uterine horn. The crown-rump length (CRL) measurement was 1.6 cm, which corresponded to eight weeks gestation, as part of the patient’s fourth pregnancy.
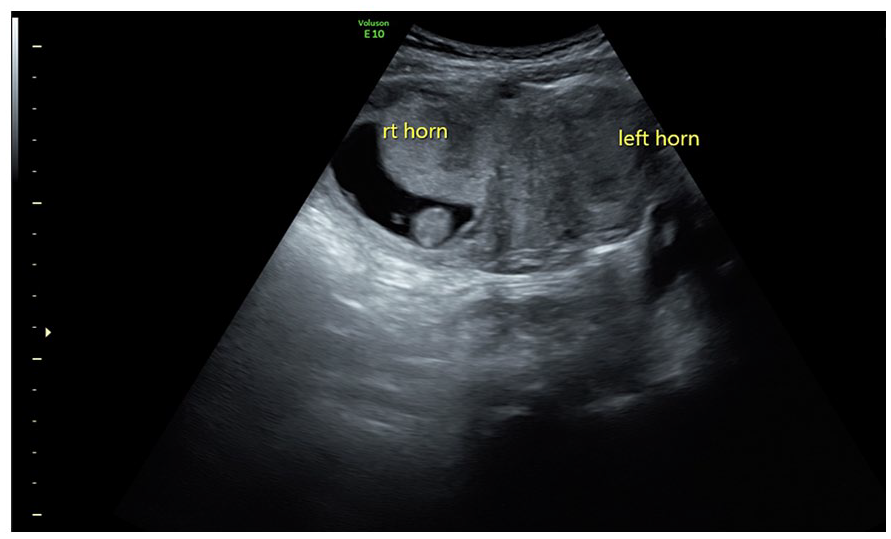
A sonographic demonstration of a bicornuate uterus with viable intrauterine pregnancy, in the right uterine horn. This sonogram was completed at 8 weeks gestation and was part of the assessment of the patient’s fourth pregnancy.
Discussion
Müllerian duct anomalies have been noted to have a higher association with endometriosis and infertility. 6 If not detected early, MDA can cause pregnancy complications. Occurring in 4% of the general population, MDA contributes to 40% of abortions and preterm deliveries. However, the patient, in the current case series, did not have any history of endometriosis, nor issues with infertility. This case series emphasized the use of 3D sonography and helped to recognize the type of MDA, that the patient possessed. In a comparable study done by Grigore et al., 7 the role of hysterosalpingography and 3D sonography was important in the care of 139 patients. In that patient cohort, 3D sonography had a sensitivity of 88%, specificity of 94%, a positive-predictive value of 96%, a negative-predictive value of 84%, likely the ratio of 5.5, and the accuracy of 90% in diagnosing uterine cavity abnormalities. 7 There was also a 100% sensitivity and 99% specificity in diagnosing congenital uterine malformation. 7 Therefore, it may be highly beneficial to use 3D sonography in cases of an uterine abnormality or a diagnosed MDA. In comparison, the current case series patient had no hysterosalpingography performed, only sonography examinations. However, this case series would seem to support the Grigore et al., study that 3D sonography was a diagnostic key to recognizing the morphology of the current patient’s uterus and identifying her bicornuate uterus, early in pregnancy. Therefore, improved patient care and associated treatment plans were available for the current case study patient and her subsequent pregnancies. All these diagnostic decisions were made to protect her four pregnancies and have positive patient and fetal outcomes. Sonography played an important diagnostic role in allowing early recognition of that patient’s shortened cervix, which had a positive effect on the treatment and management plan, as it allowed the placement of the cerclage, prevented complications, and aided in preventing preterm labor.
In addition, serial sonograms, early and throughout gestation, were crucial to ensure the condition of the cerclage, and cervix was closed, without complications or signs of preterm labor. A meta-analysis compared cerclage versus no cerclage in patients with shortened cervical length, during the second trimester. The review concluded that cerclage is associated with a significant decrease in preterm birth and improved neonatal morbidity and mortality. 8 A cohort study by Yassaee and Mostafaee examined 40 pregnant patients, with uterine anomaly, to compare the role of cerclage in the pregnancy outcome, regarding preterm and term deliveries. The participants were divided into two groups: the case group included 26 women with uterine anomalies for whom cervical cerclage was done and the control group was composed of 14 women with uterine abnormalities for whom cervical cerclage was not performed. 9 They found that in patients with bicornuate uterus, and cervical cerclage, term delivery occurred in 76.2% and preterm delivery in 23.8%. In patients with bicornuate uterus and without cervical cerclage, term delivery occurred in 27.3% and preterm delivery in 72.7%. In patients with arcuate uterus and cervical cerclage, term and preterm deliveries were equal (50% vs 50%), still in a patient with an arcuate uterus and without the cerclage, term and preterm deliveries occurred in 66.6% and 33.3% of the participants, respectively. 9 Yassaee and Mostafaee 9 concluded that cervical cerclage is an effective procedure in bicornuate uterus for the prevention of preterm deliveries. Still, it does not affect the pregnancy outcomes in the arcuate uterus. This current case series supports the use of cerclage for the bicornuate uterus, to prevent preterm labor. The statistics of the Yassaee and Mostafaee study supports the hypothesis that using cerclage in a patient with bicornuate uterus, as seen in this case study, may prevent preterm labor. In addition, 3D sonography is very useful, as it can assist in detecting the type of uterine anomaly (See Figures 1 and 2). Since cerclage was deemed helpful for patients with a bicornuate uterus; however, it may not be for those with an arcuate uterus. Given that those with an arcuate uterus have only minor irregularity in urine shape, they should be identified and followed differently. Although cerclage placement was scheduled for the current case series patient’s twin pregnancy, it was avoided and substituted by a routine cervical sonogram, every month, as it measured 5.0 cm and had no clinical features of incompetence.
Li et al. conducted a study on patients with twin pregnancies to estimate whether cerclage could extend the length of a pregnancy, lower the risk of preterm labor, and improve perinatal outcomes. This cohort study compared a cerclage placement to a lack of cerclage and its effectiveness for a twin pregnancy. 10 Their meta-analysis indicated that cerclage placement was beneficial for reducing preterm birth and prolonging a twin pregnancy, with a cervical length of <15 mm, or a dilated cervix of >10 mm. However, the benefit of a patient history which indicated the use of cerclage (singleton or twin) was less certain in twin pregnancies with a normal cervical length, based on their review of the literature. Further high-quality studies were needed to confirm Li et al.’s 10 findings that published cohort result would fit with the current case series, where the cerclage was not placed for the third pregnancy of twins, as the cervix was measuring 4.39 cm. Unfortunately, 3D sonography was only relied on to diagnose the shape of the uterus, where it could add more diagnostic value, if used to measure the cervical length.
Conclusion
This serial case study was presented to highlight the diagnosis of MDA, as well as providing this patient’s high-risk pregnancies with a suitable treatment plan. In this case, 3D sonography was used prior to pregnancy and to diagnose bicornuate uterus. The patient had multiple pregnancies located in different horns, and an incompetent cervix in her first gestation. Placement of cerclage through her first two pregnancies due to the shortened cervix and during her second pregnancies, prophylactically, played a important role in preventing preterm delivery. In addition, having the advantage of an MDA diagnosis, allowed for a closer investigation of pregnancy location, in this patient’s subsequent pregnancies. Renewed research into the use of 3D sonography, to monitor pregnancies complicated by an MDA diagnosis, is needed to measure its clinical impact for improved maternal-fetal outcomes.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because the data were properly anonymized and followed HIPPA guidelines.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.