
Abstract
Uterine didelphys is a rare congenital anomaly of the female reproductive organs, designated by the presence of the uterus as a pair of organs. This occurs as a result of the failure of the embryonic fusion of Müllerian ducts. Women with this abnormality have a paired uterus with two cervices and usually a double vagina. The chance of having a pregnancy in one of the pairs along with prolapse of the other is very low in a didelphic uterus. To the best of the author’s knowledge, only one case of such an event has been reported so far. In this case report, we are reporting on a 28-year-old gravida four para three (all are vaginal deliveries, 2 are alive, healthy, and term deliveries without any compilation; 1 is an early neonatal death delivered at 8 months) woman who presented to our hospital with a complaint of a protruding mass per vagina for 14 days in the presence of pregnancy. After she was evaluated and investigated, she was diagnosed with pelvic organ prolapse and late-preterm pregnancy. The prolapse reduced gradually as the gestational age advanced. Cesarean section was done at the gestational age of 38 weeks plus 2 days for the indication of infected pelvic organ prolapse in labor, with the outcome of a 3000 gram male alive neonate. Intraoperatively, there was uterine didelphys, one uterus holding the pregnancy while the other was prolapsing.
Introduction
Müllerian duct anomalies (MDAs) are a group of congenital defects of the female reproductive tract which occur due to the abnormal formation, fusion, or resorption of Müllerian ducts in utero. It is classified as an abnormality of formation (agenesis), lateral fusion defects (arcuate, bicornuate, didelphys, septate, and unicornuate), and vertical fusion defects (transverse vaginal septum).1,2
The didelphic uterus results from a lateral fusion defect and is one of the rare types of MDAs occurring in 1/3000 of all women and 11% of women with Müllerian anomalies. It arises from incomplete fusion of the upper portion of the Müllerian ducts that results in two entirely separate hemi uteri, two cervices, and usually two vaginas or a longitudinal vaginal septum. The cause of the failure of fusion is not known. But there are several risk factors identified as contributing factors. Patients with a didelphic uterus may have associated defects in the renal system, vagina, and, rarely, the skeleton.3–5
The diagnosis of MDAs, including didelphys, is challenging and usually made during the reproductive period. This is believed to be because they are associated with symptoms like amenorrhea, dysmenorrhea, dyspareunia, pelvic pain, and obstetric complications such as recurrent pregnancy loss, premature delivery, malpresentation, intrauterine growth restriction (IUGR), placental abruption, and cervical insufficiency.5–8
Pelvic organ prolapse (POP) has been reported in women with MDAs. 9 A chance for a didelphic uterus to present as POP in one uterus and pregnancy in the other is a very rare event, with only one case reported to the best of our knowledge. While no guideline has been published for management in this rare scenario, the decision about the treatment modality is made depending on the expert’s opinion.4,10,11
Case
This is a 28-year-old gravida four para three (all are vaginal deliveries, two alive, healthy, and term deliveries without any compilation, one early neonatal death delivered at 8 months) mother whose gestational age from LNMP (Last Normal Menstrual Period) was 36w5d who came to Wolaita Sodo University Comprehensive Specialized Hospital with the chief complaint of protruding mass per vagina of 14-day duration. Associated with the prolapse, she was also complaining of lower abdominal pain and a foul-smelling vaginal discharge of 4-day duration. She had an antenatal care follow-up at a nearby health center twice in the second trimester and it was uneventful, but she was not evaluated in a hospital or by a senior obstetrician. Other than the above complaint, she has no headache, blurring of vision, vaginal bleeding, dysuria, or urgency. She has no history of self- or family-diagnosed chronic surgical or medical illnesses like hypertension, diabetes mellitus, renal, or cardiac illness.
Upon physical examination, her vital signs were blood pressure (BP) of 120/75, pulse rate (PR) of 100, respiratory rate (RR) of 18, and temperature of 37.1°C.
The other systems’ physical examination was unremarkable except for the abdominal and genitourinary systems’ evaluation.
On obstetric abdominal palpations, the fundal height was 36 weeks, longitudinal lie, cephalic, and with a positive FHB (Fetal Heart Beat) (144) without uterine contraction.
Genitourinary examination revealed a protruding mass per vagina of 5 × 7 cm, which is pink-colored, with an ulcer and a whitish foul-smelling discharge on its surface (Figure 1). Upon palpation of the mass, it was tender and irreducible.

(a) A gravid uterus, POP (infected and ulcerated) and (b) focused view of the ulcerated POP.
Blood workup
The White blood cell count was 12,790/mm3, hemoglobin was 10.5 g/dL, hematocrit was 32.3%, and platelet was 306,000 per microliter. Liver enzyme measurement and renal function tests were unremarkable: SGPT (Serum Glutamic Pyruvic Transaminase) = 12 IU/L, SGOT (Serum Glutamic Oxaloacetic Transaminase) = 26 IU/L, and creatinine 0.9 mg/dL.
An ultrasound examination was performed with the findings of singleton intrauterine pregnancy, cephalic, aggregate gestational age of 35 weeks, and an estimated fetal weight of 2500 g.
She was admitted to the obstetric ward with the diagnosis of late-preterm pregnancy and stage 3 POP with an infected decubitus ulcer. After admission, she was given therapeutic antibiotics (ceftriaxone and metronidazole), wound care, and a single course of corticosteroid (dexamethasone for fetal lung maturity).
With the above management, she improved after resting and discontinued stressful activities. The prolapse reduced gradually, and on the 10th day, no mass was visible externally.
After a 12-day stay in the obstetric ward, the patient started to complain of pushing down pain and the passage of liquor of 1-hour duration. Upon physical examination, she was diagnosed with active phase of the first stage of labor at term and POP with an infected ulcer being managed. For this, she underwent an emergency cesarean section (CS), with the outcome of a 3000 gram male alive neonate with an APGAR score of 8 & 9.
Intraoperatively, there were two uteruses (one gravid, the other not) with their single tube and ovary (Figure 2). Both kidneys were palpated and are normal.

(a) Intra-operative picture of the posterior view of the double uterus; (b) an anterior view of the double uterus with their tube and ovary, and the right uterus with a repaired cesarean incision.
She had a smooth postoperative period, and her postoperative hematocrit was 32%. She was discharged on the fifth day after surgery with an appointment at a postpartum clinic. After 4 months of delivery, she was evaluated by speculum examination and screened for cervical cancer by visual inspection with acetic acid (VIA). On the speculum examination, two cervices were seen (Figure 3). Screening for cervical cancer by VIA was negative; an ultrasound was done, and it showed two separate uteruses and cervices (Figure 4).
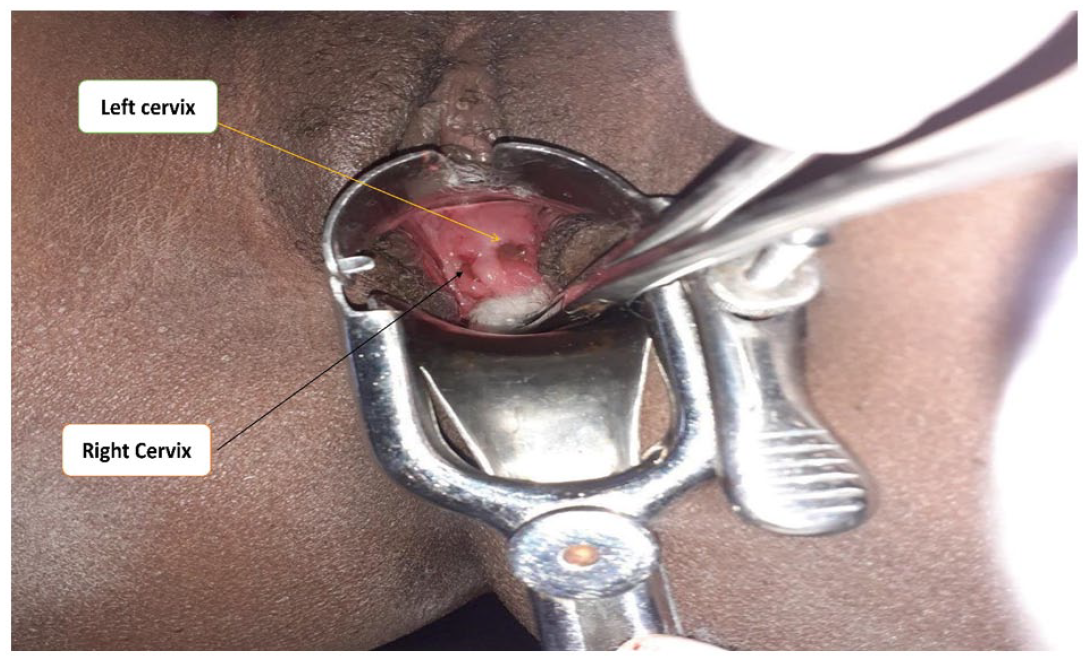
Speculum examination showing two cervices and negative for VIA.

Two-dimensional ultrasound showing two uteruses and cervices.
Discussion
MDAs affect 0.1%–3% of women. Didelphys uterus results from extreme non-fusion, with complete duplication of the uterus, cervix, and vagina. It accounts for 11% of MDAs and is typically asymptomatic.8,12
Two-dimensional (2D) transvaginal sonography and hysterosalpingography are great screening tests for low-risk mothers. Three-dimensional (3D) pelvic ultrasound is recommended to diagnose and classify MDAs accurately for those who have had inconclusive findings during screening tests or who have had a recurrent pregnancy loss. Magnetic resonance imaging and combined laparoscopy and hysteroscopy should be considered for MDAs complex for diagnosis.
Uterus didelphys has also been related to higher rates of infertility, spontaneous miscarriage, IUGR, and postpartum hemorrhage. However most women with MDAs have a good reproductive outcome. Depending on the type and severity, it is important to advise women with MDAs about the high risk of first- and second-trimester miscarriage, preterm delivery, fetal malpresentation, IUGR, and preeclampsia. 1
In another review, uterus didelphys was not linked to decreased natural or assisted fertility or an increase in spontaneous abortions, according to a meta-analysis of 25 studies covering more than 160,000 women, including 3766 with congenital uterine abnormalities. According to the research, there is an increased chance of breech presentation, intrauterine growth retardation in the fetus, low-birth-weight newborns below 2500 g, preterm birth before 37 weeks gestation, and perinatal death. 13
When a uterine didelphys is diagnosed, the kidney should also be investigated for anomalies to rule out Herlyn–Werner–Wunderlich syndrome. In mothers who have a major fusion abnormality, placental implantation is essentially unilateral. This could result in the loss of function of one uterine artery in the uteroplacental circulation. This could be the reason for placental insufficiency, IUGR, and intrauterine fetal death.14–16 In our patient, we evaluated the kidney, and it was normal.
POP has been reported in women with MDAs. All cases reported, however, were when MDAs were diagnosed before or at the same time as the development of POP in premenopausal women. Upon a literature search for case reports of POP with MDAs, only 19 cases were found. Among reported cases of MDAs associated with POP, the majority were women with neovagina. 9 There is one case report of double prolapse of the didelphys uterus. 17
For pregnant patients with MDAs, the mode of delivery must be decided individually. The literature reports are almost equal for those who prefer CS and those who prefer vaginal delivery. It is quite common to get abnormal presentations and positions in patients with uterus didelphys, but there are reports of successful labor in this group of women. 10 CS was the mode of delivery for 82% of patients having MDAs, as reported by Heinonen et al. 18
Because of the inadequate development of the uterus’s muscular part, sometimes it can lead to inert labor, and uterine rupture, though we have not found any case reports of rupture in the literature reviews. Obstructed labor can be caused by a long and firm cervix, which is often attached to the other uterus. Moreover, often the non-gravid uterus rotates posteriorly and becomes confined in the pelvis, which leads to mechanical obstruction. 10
Patients with uterine didelphys and POP frequently have apical prolapse, which may present at younger ages or in nulliparous women. A number of surgical treatments can offer the symptomatic patient significant improvement, but it may require modifications to typical surgical procedures since the ureter is much closer and more likely to become kinked. Before cuff closure, it is good to consider ureterolysis and more extensive bladder dissection, as well as cystourethroscopy to ensure ureteral jets after closure.19,20
Although laparoscopic uterosacral ligament hysteropexy or total vaginal hysterectomy with uterosacral ligament suspension for anterior and apical prolapse can be performed, laparoscopic uterosacral ligament hysteropexy is associated with a better anatomic and symptomatic cure rate and women’s satisfaction. 21 It is crucial to consider how to approach women with special anatomy, like uterine anomalies, who want uterine-sparing surgery. One case report demonstrated that vaginal uterosacral ligament hysteropexy is reasonable in a patient with POP and uterine didelphys. 22
A chance for a didelphic uterus to present as POP in one uterus and pregnancy in the other is a very rare event, with only one case reported to the best of our knowledge. While no guideline has been published for management in this rare scenario, the decision about the treatment modality is made depending on the expert’s opinion.4,10,11
Conclusion
Didelphys uterus is an extremely uncommon MDA. We suggest that the management and outcome of pregnancy with uterine prolapse depend on symptomatology, prolapse severity, the degree of obstruction, and patients’ preferences. Depending on these facts, it requires an individualized approach to management. In pregnant women with MDAs, the mode of delivery must be individualized, taking into account maternal and fetal well-being as well as maternal preference. A didelphic uterus presenting as POP in one uterus and pregnancy in the other is a very rare event, with one case reported so far, so we report this case after managing it in an individualized manner.
Footnotes
Acknowledgements
I would like to thank Ms. Selamawit Getachew and Dr. Bethlehem Admasu for editing and commenting on this case report.
Author contributions
All authors are involved in diagnosing and treatment, including operation, while the corresponding author wrote the case report. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the journal submitted, and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Patient consent
Informed written consent has been obtained from the patient for all case details and images to be reported in the journal.