
Abstract
Pregnancies within rudimentary horns of unicornuate uteri are extremely rare. These pregnancies account for approximately 1 in 76 000 to 1 in 140 000 worldwide, with uterine rupture being the most concerning complication. A case is presented of a 24-year-old female, gravida 2, para 0, who underwent multiple sonograms pertaining to two gestations over a 3-year period. Both pregnancies occurred within the left rudimentary horn of a unicornuate uterus. The left rudimentary horn was confirmed, on magnetic resonance imaging, to have no communication with the right horn or endocervical canal. The first pregnancy resulted in a missed abortion, and the second pregnancy, 3 years later, was a twin gestation, which was carefully monitored. At 20 weeks, the uterus began to rupture, and an emergency C-section was attempted. Neither the fetus nor the rudimentary horn survived, which was excised. This case demonstrates a rare uterine finding, a pregnancy occurred twice within the horn that lacked communication with the cervix.
Keywords
Introduction
Pregnancy within a rudimentary horn is a rare occurrence.1–3 It is about 1 in 76 000 to 1 in 140 000 of all pregnancies worldwide.1–5 Uterine rupture is the most concerning complication associated with these pregnancies.5,6 Early diagnostic sonograms can provide critical information about maternal and fetal health associated with life-threatening pregnancies of this nature. Clinical coordination, careful monitoring of pregnancies, and planned Caesarian sections increase the chance of having a live delivery.
Müllerian duct anomalies (MDAs) are often evaluated sonographically. However, there are some sonographic limitations with regard to imaging depth during pregnancy that make some cases difficult to diagnose with sonography alone. 3 Magnetic resonance imaging (MRI) is noninvasive, does not use ionizing radiation, and is an option to visualize the entire fetus in the enlarged uterus.7–9 In addition, MRI has multiplanar capability, is excellent at demonstrating soft-tissue characterization, and permits greater imaging depth and a greater field of view when compared with sonography. 8
A case is presented of a 21-year-old female who underwent multiple sonograms and MRIs pertaining to two separate gestations over a 3-year period. During the first pregnancy, a unicornuate uterus was suspected with sonography and later confirmed using MRI. In the second pregnancy, which showed twin fetuses, a uterine rupture occurred at 20 weeks in the gestation. Though an exploratory laparotomy was performed in an attempt to save the pregnancy, both fetuses demised. The left rudimentary uterine horn was excised during the procedure. Similar to the first pregnancy, diagnoses in the second pregnancy benefited from both the use of sonography and MRI. A discussion of the events of the two pregnancies is presented.
Case Study
A 21-year-old female, gravida 1, para 0, was seen in a medical center for an initial sonogram to confirm pregnancy. A Siemen’s Sequoia 512 with a 4V1 Vector 4 MHz transducer was utilized for a transabdominal sonogram, and an EV-8C4 8 MHz transducer was used to obtain transvaginal images (Siemens Healthcare, Malvern, PA). The first sonographic images (Figure 1) revealed a uterine anomaly reported to be a possible unicornuate uterus. The left horn of the uterus contained a fetus with no cardiac activity, approximately 8 weeks, 1 day as measured by crown-rump length. The patient was then referred for a multisequence, multiplanar noncontrast MRI of the pelvis (Figure 2) using a General Electric 1.5T Signa Excite (GE Healthcare, Wauwatosa, WI), which documented a unicornuate uterus with a rudimentary left horn. The report stated that a unicornuate uterus with a rudimentary left horn was evident.
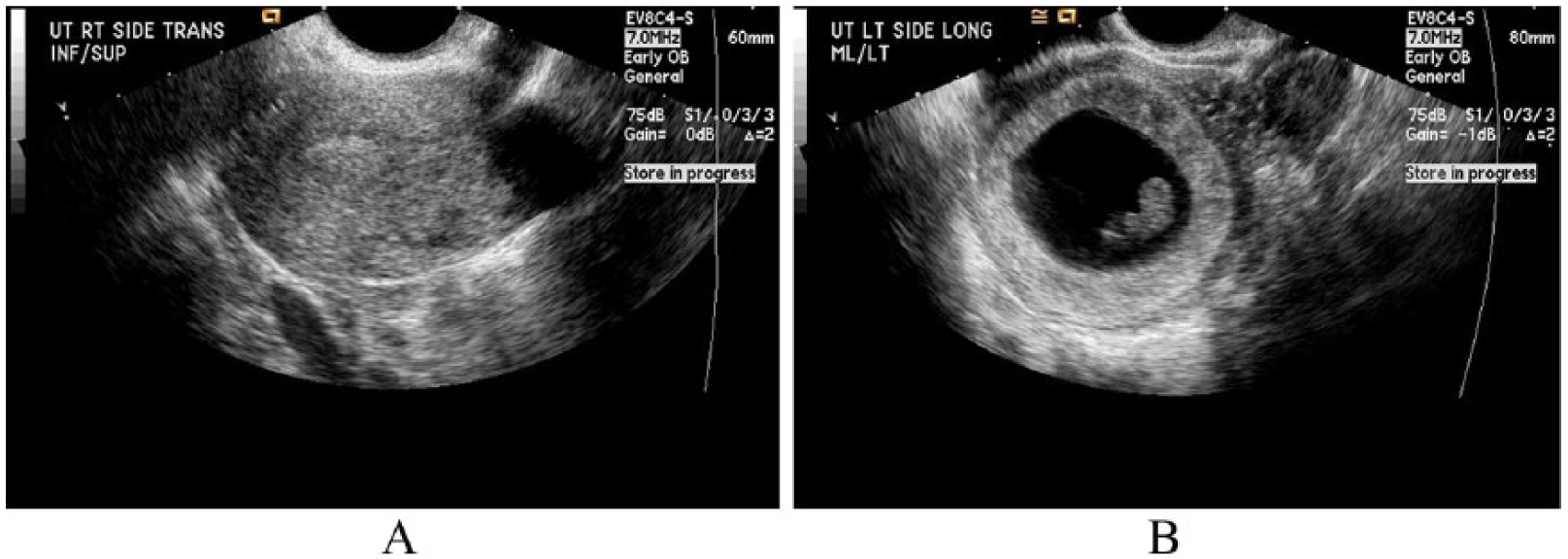
(A) Transvaginal sonogram demonstrating a sagittal image of the right uterine horn with a normal-appearing endometrium. (B) A sagittal image of the left rudimentary horn containing a gestational sac. The gestational sac contained a nonviable embryo approximately 8 weeks gestational age.
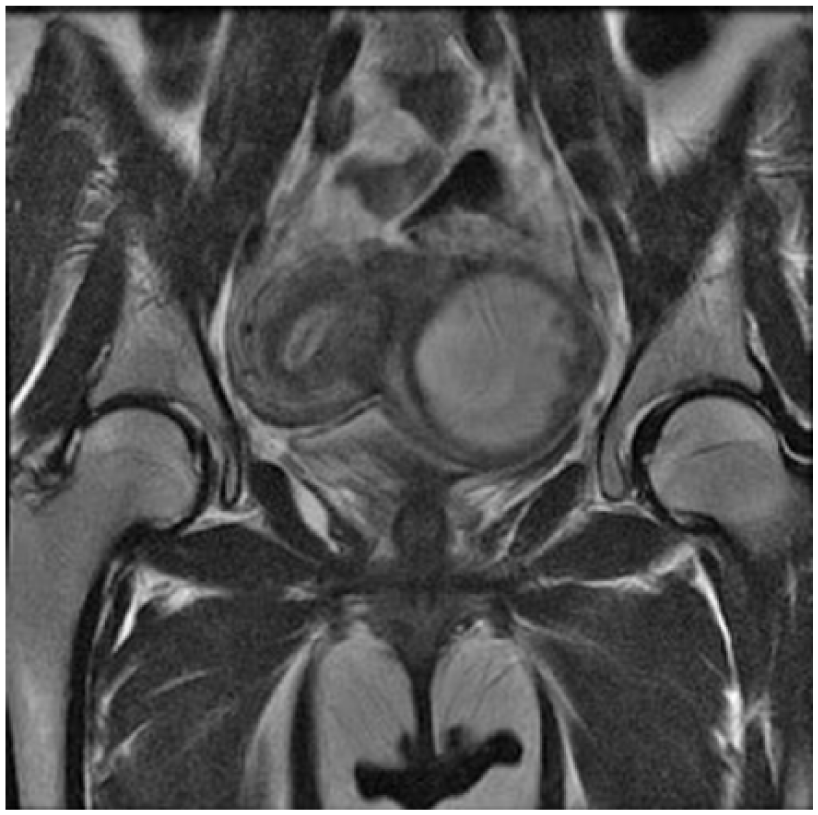
A magnetic resonance image in a coronal plane demonstrating the two uterine horns. An endometrium without a gestational sac can be seen in the right horn. There is a gestational sac seen in the left rudimentary horn related to the 8-week, 1-day singleton pregnancy.
After unsuccessful removal of the missed abortion (MAB) by dilation and curettage procedure, the patient eventually required radiofrequency ablation for removal of the products of conception from the rudimentary left horn (Figure 3). A second noncontrast MRI was performed to evaluate the uterus in a nongravid state (Figure 4). The purpose of this MRI was to determine the specific details of the MDA not fully appreciated during pregnancy. The radiology report stated that there was no communication between the left rudimentary horn and the right horn or cervix. Status post ablation in the left horn, the pregnancy was no longer evident.
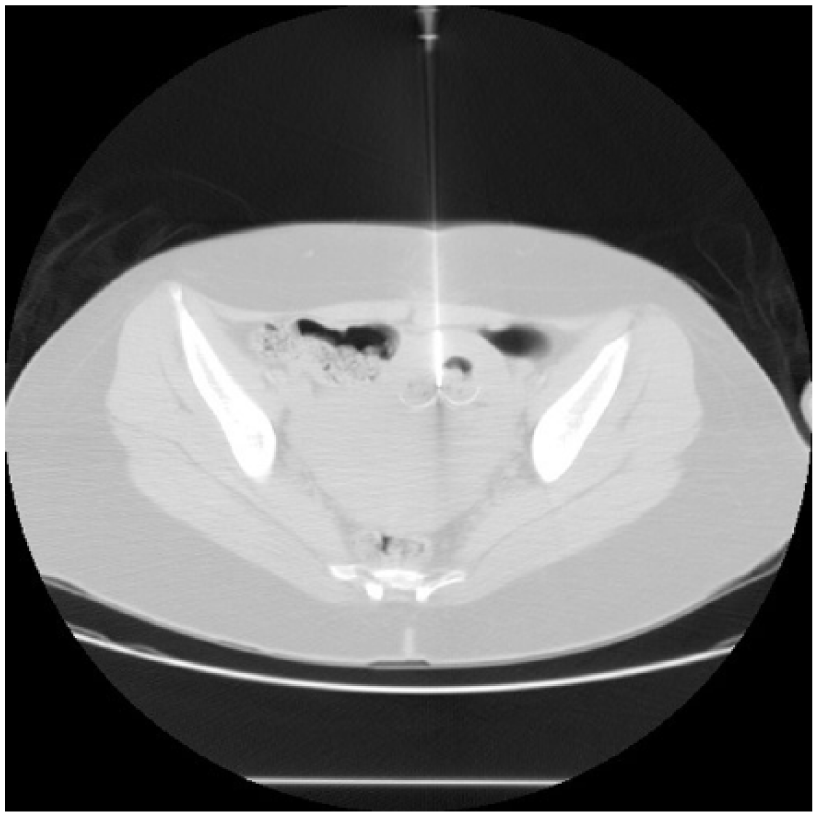
This computerized tomography scan was taken during a radiofrequency ablation to remove the retained products of conception from the left rudimentary horn after the missed abortion.
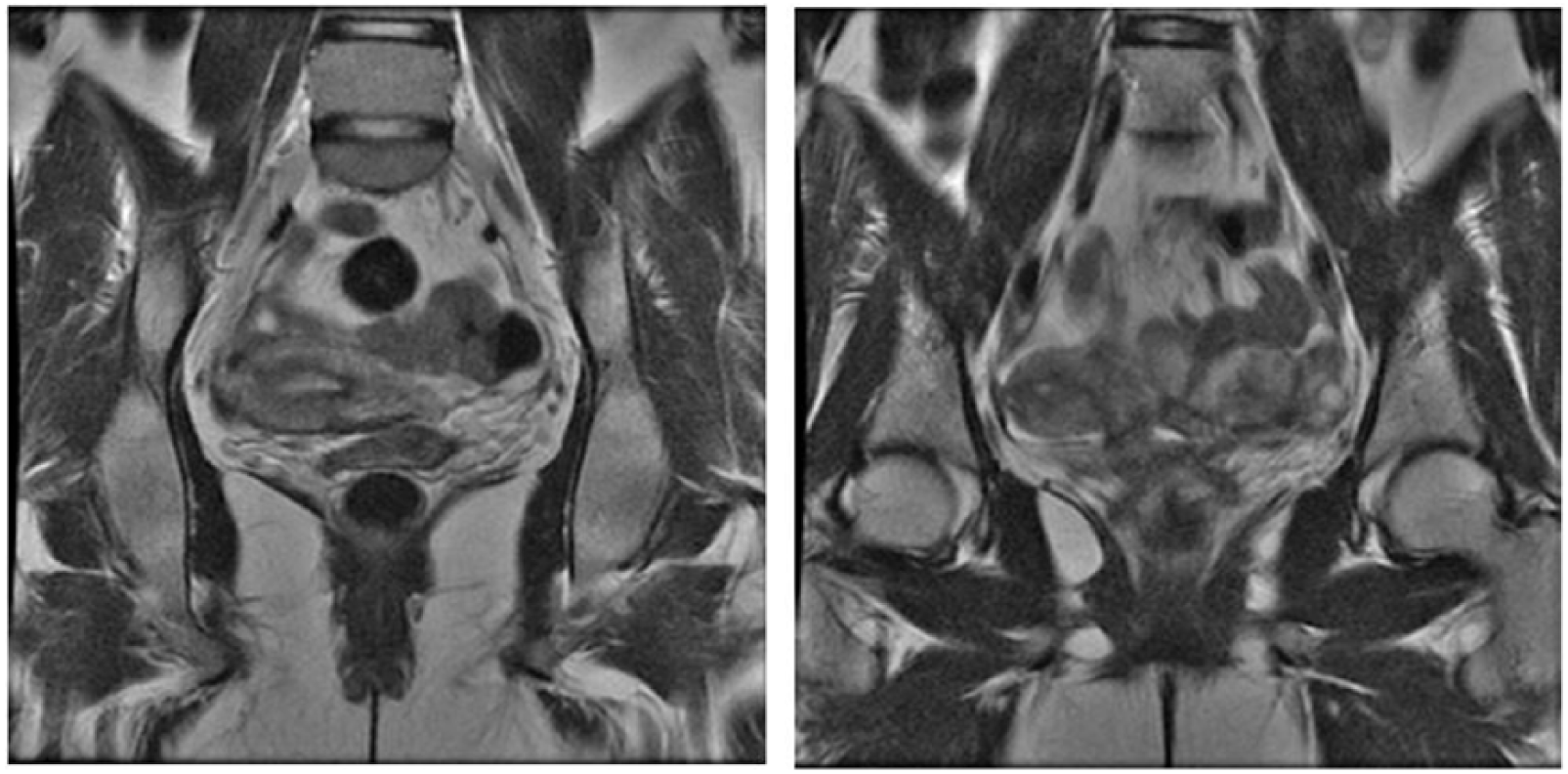
Magnetic resonance images taken in a coronal plane represent this Müllerian duct anomaly in the same patient during a nongravid state. The radiologist confirmed that the left rudimentary horn had no communication with the right uterine horn or the left endocervical canal.
Three year later, the patient, now a 24-year-old female, gravida 2, para 0, was seen in the maternal fetal medical department of the same medical center for a second pregnancy. Her gynecological history included endometriosis, ovarian cysts, multiple sexually transmitted infections (STIs), and an abnormal pap smear. A General Electric Voluson E8 Expert was used. A 4C-RS curvilinear 2.0-5.5 MHz transducer was used to obtain transabdominal images. The sonogram revealed a monochorionic-diamniotic gestation contained within the left rudimentary horn. Fetus A had a crown rump length (CRL) of 6.9, cm corresponding to a 13.1-week gestation in the 38th percentile. Fetus B had a CRL of 7.3, cm corresponding to a 13.4-week gestation in the 51st percentile. Regular cardiac rhythm was observed in both fetuses, and the location of the placenta was posterior. Transabdominal evaluation of the cervical canal indicated no shortening or funneling (Figure 5). There was no evidence of twin-to-twin transfusion syndrome.

Sonogram demonstrating a 13-week, 3-day, viable monochorionic-diamniotic gestation contained in the left rudimentary horn. The sonographer documented the presence of a membrane separating the two fetuses in multiple planes throughout the sac.
Four days later, the patient presented to the emergency department of the same medical center for left-sided lower abdominal pain. The medical staff ordered a transabdominal sonogram with the indication of pelvic pain. The sonographer demonstrated what was thought to be a gestation within a normal uterus (Figure 6) with a fibroid in the lower uterine segment (LUS). There was no specification of a rudimentary horn noted at the time of this exam.
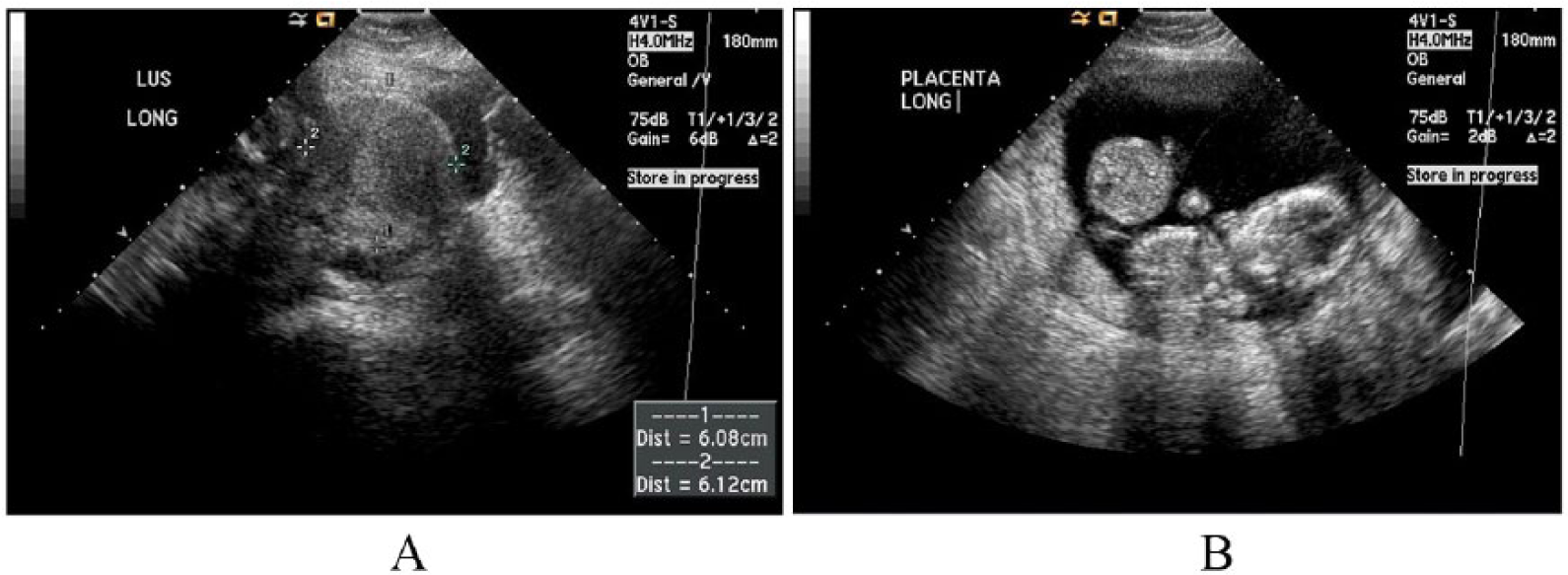
(A) A sagittal image of the LUS showing the right horn, which the sonographer documented as a potential fibroid. (B) Sagittal transabominal sonogram representing the twin gestation. Note that the lower uterine segment (LUS) is not demonstrated.
Nine days after the first emergency department visit, the patient returned with persistent and now more intense left-sided lower abdominal pain. The medical staff ordered a renal sonogram with the indication of kidney stones. Normal sonographically appearing kidneys were noted in this exam. After discussing the medical history with the patient, a follow-up obstetrical sonogram was performed. At this time, there was suspicion of an abdominal ectopic pregnancy (Figure 7). There was also concern that the myometrium appeared unusually thinned, with potential for uterine rupture (Figure 8). The radiology report from this study was equivocal, and due to the patient’s complex history, an MRI of the pelvis was ordered.
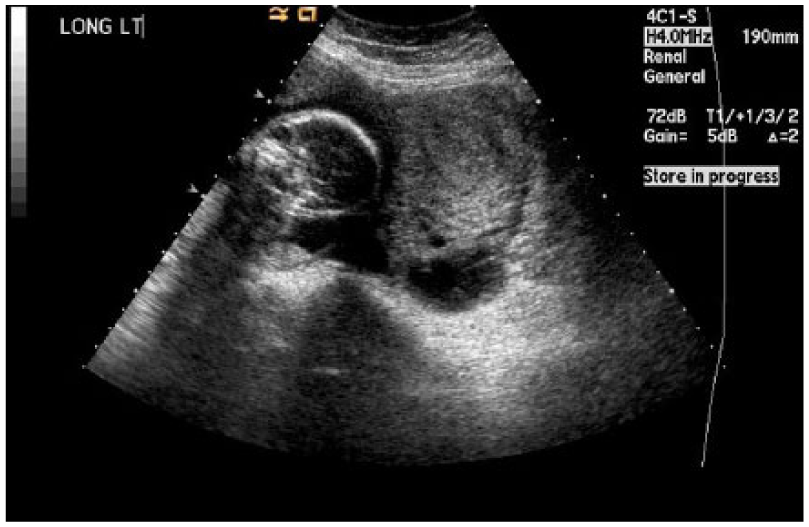
A transabdominal sonogram attempting to demonstrate a gestational sac that was believed to be a potential abdominal ectopic pregnancy.

This transabdominal sonogram represents a lack of connection between the gestational sac and the lower uterine segment. Additionally, a thin layer of myometrium is seen surrounding the sac, which was indicative of potential uterine rupture.
The patient was referred for multisequence, multiplanar MRI with 10 cc Magnevist IV contrast of the abdomen and pelvis using a Siemens 1.5 Magnetom Aera. The uterus was identified extending to the right with the endometrium appearing contiguous and tubular, suggesting a uterine anomaly with an empty right horn. A single cervix was identified. There was questionable parenchyma extending from the lower uterine segment toward the gestational sac. A twin gestation was identified with one fetus in the transverse presentation and the other in cephalic presentation (Figure 9). Using MRI, it was interpreted that this twin gestation was likely contained within the left rudimentary horn. The right uterine horn appeared to lie transverse in the pelvis. Coronal MRI images showed both fetuses within the same gestational sac, surrounded by a very thin layer of myometrium, contained in the left rudimentary horn (Figure 9).
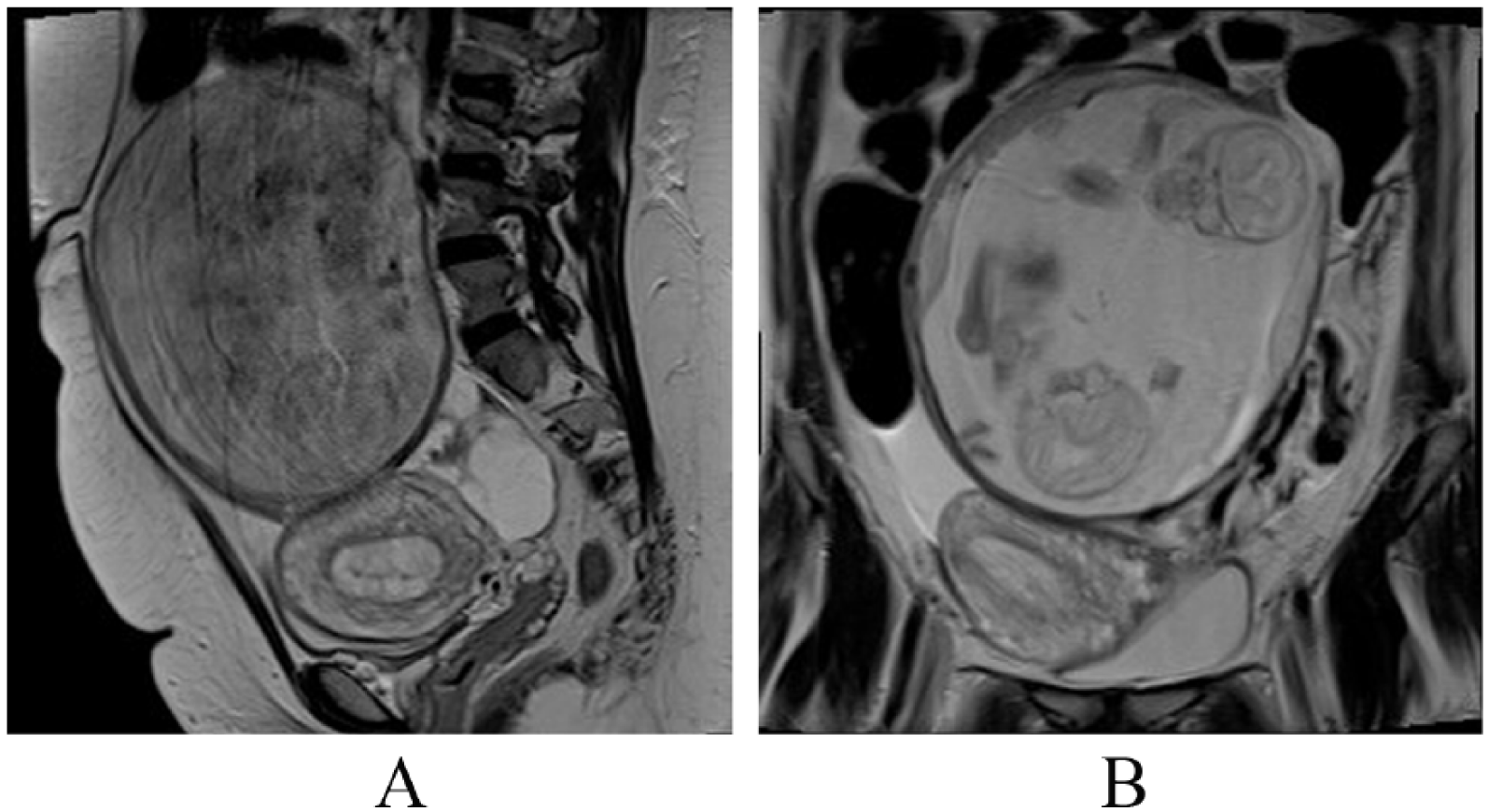
(A) A magnetic resonance image (MRI) in a sagittal plane demonstrating two uterine horns. The left rudimentary horn contains the pregnancy. Note the right horn (without a gestational sac) appears to lie transverse in the pelvis. (B) An MRI in a coronal plane demonstrating both fetal heads within the gestational sac contained in the left horn.
Due to concern of uterine rupture, the patient was referred to maternal fetal medicine for careful monitoring. The OB/GYN physician and surgical team prepared for a Caesarian section at 25 weeks in the gestation to deliver the twins. At 20 weeks, the uterus began to rupture, and an emergency C-section was attempted that resulted in demise of both fetuses. The left rudimentary uterine horn was excised during this procedure.
Discussion
Mauriceau and Vassal first described rudimentary horn pregnancy in the literature in 1669.1–5 In general, unicornuate uteri are rare, only making up about 5% of MDAs.1,10 This uterine anomaly results from unilateral hypoplasia of the uterine ducts during fetal development.
5
The embryonic process, which shapes the uterus during fetal development, begins with the Müllerian ducts.
8
The Müllerian ducts are the structures responsible for the development of the upper two-thirds of the vagina, cervix, uterus, and fallopian tubes.
9
Unicornuate uteri carry increased risks for miscarriage, preterm labor, ectopic pregnancy, and most significantly, uterine rupture.
8
Knowledge of MDAs is often a first step in understanding the possible outcomes of pregnancies associated with these anomalies. Diagnosis of MDAs is important because of the high risk of associated pathology: MDAs have high association with endometriosis and infertility, and 15% of women who have had recurrent miscarriages have a documented MDA. 9 In 2009, Chandler et al. 9 reviewed the seven classifications of MDAs as outlined by the American Fertility Society. Class I, uterine agenesis/hypoplasia, is characterized by lack of identification of a uterus or small amounts of rudimentary tissue. 9 Class II, unicornuate, has four possible subtypes: (1) no rudimentary horn, (2) rudimentary horn with no uterine cavity (nonfunctional rudimentary horn), (3) rudimentary horn with a communicating cavity to the normal side, and (4) rudimentary with a noncommunicating horn.8,9 Renal anomalies (most commonly renal agenesis), ipsilateral to the rudimentary horn, are seen in about 40% of cases. 8 Class III, dydelphys, has fully developed, normally sized, individual horns; a deep fundal cleft; and two cervices. 9 Class IV, bicornuate, has a central myometrium with a fundal cleft greater than 1 cm deep. 9 Bicornuate horns are not as fully developed as compared to those seen in didelphys uteri. 9 Class V, septate, will present as a uterus that is completely or partially divided into two cavities. 9 Class VI, arcuate, is characterized by a mild indentation of the endometrium at the uterine fundus. 9 Finally, Class VII, diethylstilbestrol (DES) related uteri, are characterized as having a “T-shaped” uterus cavity. 9 These have resulted from the use of the drug, DES, which was used in the prevention of miscarriage between 1945 and 1970. 9
Pregnancies within a rudimentary horn are uncommon.1–4 It is estimated that about 600 to 700 pregnancies have been reported within the rudimentary horn at the time of this study. 1 Rupture of the rudimentary horn is considered a surgical emergency. 10 The rate of live births has been reported to be from 10% to 13% of reported cases worldwide since 1946.3,4,11 The endometrium is particularly thin and does not typically have communication with the endocervical canal. 4 This lack of connection between the rudimentary horn and cervix is reported in up to 72% of cases. 10 Given that the corpus luteum is usually found on the same side as the rudimentary horn, it is believed that spermatozoon fertilizes the ovum through retrograde transperitoneal migration.4,6,12 This can occur when a fertilized or nonfertilized ovum wanders through the peritoneum from one side of the pelvis to the other. 6 In transperitoneal migration, the ovum can be transferred to the opposite tube via the peritoneal fluid within the peritoneal cavity. Also, spermatozoa that have acquired access to the peritoneal cavity through a patent oviduct may enter through the opposite fallopian tube. 6
Antenatal diagnosis of a pregnancy within a rudimentary horn can be difficult.1 –3 While many MDAs are first noticed on sonography, secondary imaging is often required with MRI. 11 Sonography is the preferred method in acute cases because it is readily available, can be performed quickly by a skilled sonographer, and is inexpensive. 8 Yet sometimes limitations exist in sonography with regard to its field of view, especially in patients with large body habitus. 8 As pregnancy advances, sonographic imaging of MDAs can be elusive because the enlarging uterine horn with thinning myometrium will often obscure the other anatomic structures.1,3 The use of sonography is best in the first trimester, with a reported 26% sensitivity in detection, which continues to decrease as gestational age progresses.4,5,10 MRI can be a very useful tool for the diagnosis of rudimentary horn pregnancies. 10 Also, MRI is often seen in the literature to confirm equivocal findings seen using diagnostic sonography because of limitations in the field of view of sonography during the advanced pregnancies when the uterus is enlarged.1–5,10 Finally, MRI is a useful tool in the diagnosis of these anomalies because of its ability to produce clear anatomic detail of both the internal uterine cavity and the external contour of the pelvis. 13
Differential diagnoses of rudimentary horn pregnancies include interstitial pregnancies, tubal ectopic pregnancies, cornual pregnancies, and abdominal ectopic pregnancies.3,5 While a rudimentary horn pregnancy may be difficult to distinguish from the aforementioned differentials, there can be grave outcomes if the anomaly is not recognized. Therefore, during a sonogram, it is crucial that sonographers pay particular attention to the thinned myometrium as this is the feature associated with premature rupture.
Conclusion
Rudimentary horn pregnancy is a rare and life-threatening condition. The fetal survival rate is very low with great potential risk to maternal mortality rate. Careful patient monitoring, including review of previous sonograms, MRIs, and other diagnostic studies, and surgical intervention are frequently necessary to achieve live births. Rudimentary horn pregnancies can sometimes present as complex and elusive using sonography alone. Therefore, follow-up with MRI can aid in confirmation of the diagnosis. The present case describes a rare occurrence of a patient with subsequent pregnancies within a rudimentary horn of a unicornuate uterus, the second of which being a twin gestation. This demonstrates the need for sonographers to be fully aware of the multiple types of Müllerian duct anomalies and their presentations to ensure proper management of care for patients with complex obstetrical history.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.