
Abstract
Mosaic trisomy 14 or partial trisomy 14 is a rare genetic abnormality that occurs when only a portion of cells have an additional copy of chromosome 14. It has a female prevalence of 3:1 and is associated with a wide range of related disorders. In this case, severe polyhydramnios because of borderline micrognathia was correlated to the diagnosis of mosaic trisomy 14. Early sonographic detection of associated findings can prompt the genetic testing required for diagnosis. Combining sonography and genetic testing leads to an accurate diagnosis, proper management, and postnatal planning for the patient.
Keywords
Partial trisomy of the 14th chromosome, or mosaic trisomy 14, is a rare genetic disorder in which some cells of the body have an extra 14th chromosome. Mosaic trisomy 14 has an incidence rate of 3:1 in females compared with males. 1 Findings commonly associated with mosaic trisomy 14 include developmental delays, growth restriction, dysmorphism, congenital heart defects, and genitourinary abnormalities. Abnormal craniofacial features such as broad nose, cleft palate, low-set ears, micrognathia, and microcephaly are also associated with mosaic trisomy 14. 2 The phenotypic findings associated with trisomy 14 mosaicism are variable and are typically non-lethal. The severity of these findings is not correlated to the proportion of cells affected by trisomy. 3 Pregnancies with complete trisomy 14 almost always result in first-trimester demise. 1 Mosaic trisomy 14 cannot be differentiated from other congenital anomalies by prenatal sonogram alone. The only way to diagnose mosaic trisomy 14 is via amniocentesis. As of 2013, only nine cases of mosaic trisomy 14 have been diagnosed via amniocentesis. 2 As of 2014, only 40 live births have been reported. 1
Case Report
A 35-year-old woman, gravida 4, para 1112, presented to the maternal fetal medicine clinic for a routine anatomy sonogram at 18 weeks 2 days, by last menstrual period. The patient’s maternal health history was significant for cavernous venous malformation following an intracranial hemorrhage in the first trimester. In addition, she was prescribed Keppra, which is an antiepileptic drug.
A detailed anatomy sonogram was performed with a Voluson E10 (GE Healthcare, Zipf, Austria) ultrasound system using a C1-6 MHz curvilinear transducer. The sonogram demonstrated bilateral choroid plexus cysts (See Figure 1), an intracardiac echogenic focus and fetal growth restriction with an estimated fetal weight of 3%, and an abdominal circumference of 10%. Based on these findings, an amniocentesis was performed. The patient was referred to genetic counseling and scheduled for an echocardiogram, as well as serial growth sonograms.

An axial sonographic view of the fetal head is provided that demonstrated bilateral choroid plexus cysts.
The amniocentesis revealed an abnormal banding pattern on chromosome 14q, on some cells. A diagnosis of partial trisomy 14 was given as some cells were not affected. A follow-up sonogram was performed at 31 weeks 1 day and demonstrated severe growth restriction, with an estimated fetal weight of <1%. In addition, the fetus had an abdominal circumference measuring <1% (See Figure 2), mild ventriculomegaly measuring 10 mm (See Figure 3), and abnormal umbilical artery Doppler waveforms. The subsequent sonogram at 33 weeks was significant for borderline micrognathia and severe polyhydramnios, with an amniotic fluid index (AFI) of 49 cm (See Figure 4). Borderline micrognathia was subjectively detected on the profile image (See Figure 5) and was objectively diagnosed using a jaw index calculation on the sonographic mandibular view (See Figure 6).
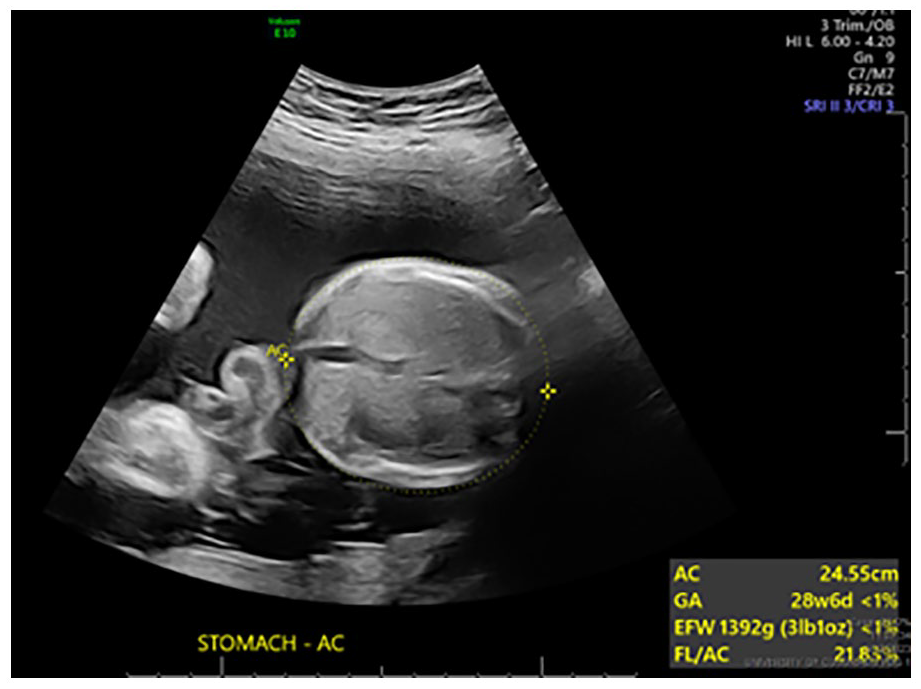
An axial sonographic view is provided that demonstrates the measurement of the fetal abdominal circumference and indicated intrauterine growth restriction.
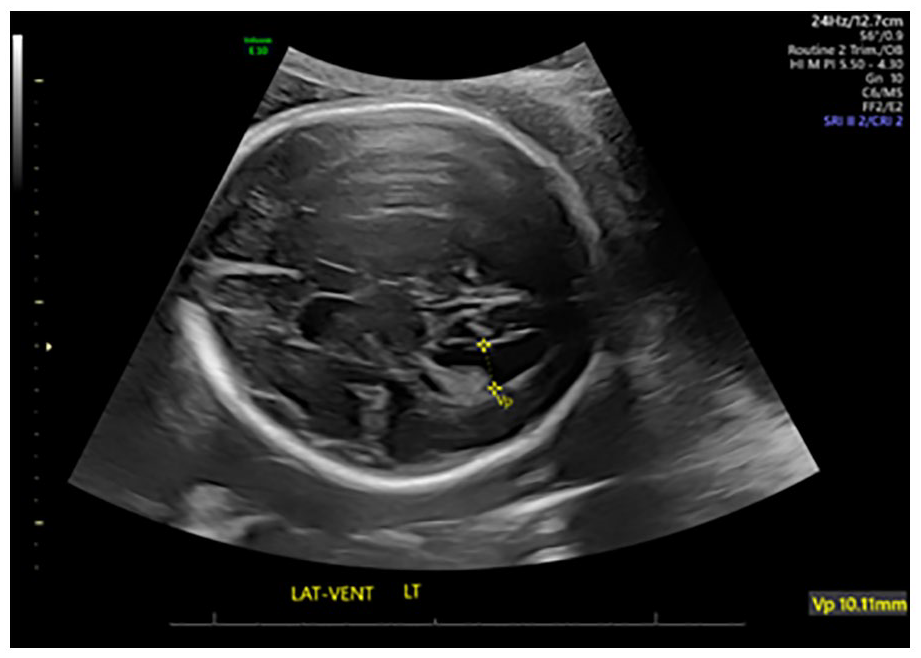
An axial sonographic view of fetal brain that demonstrated a mildly enlarged lateral ventricle.
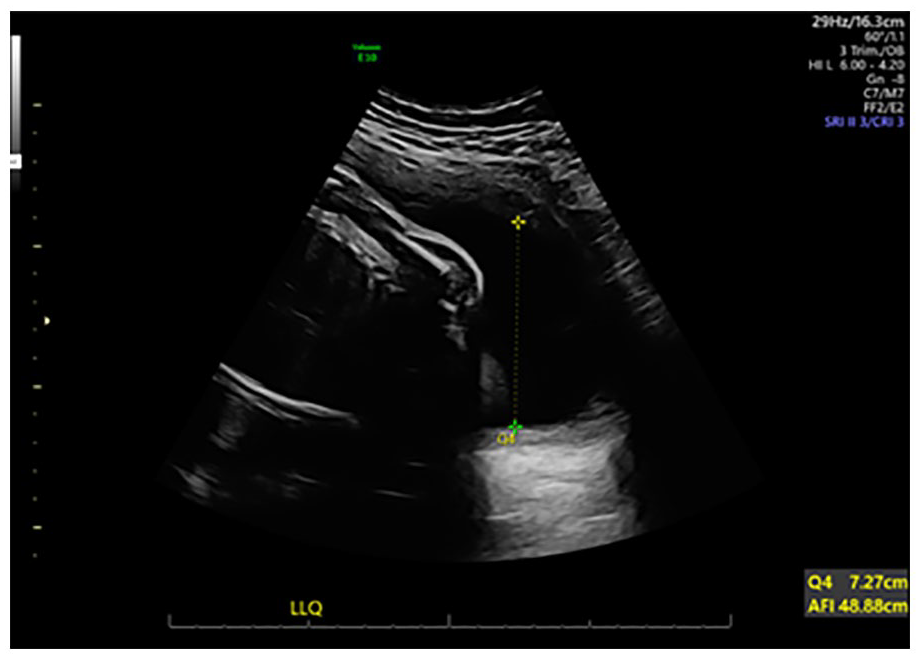
A left lower quadrant of the uterus was the location where this sonographic measurement was taken to obtain the maximum vertical pocket fluid measurement. The calculated amniotic fluid index was 49 cm, which indicated severe polyhydramnios.
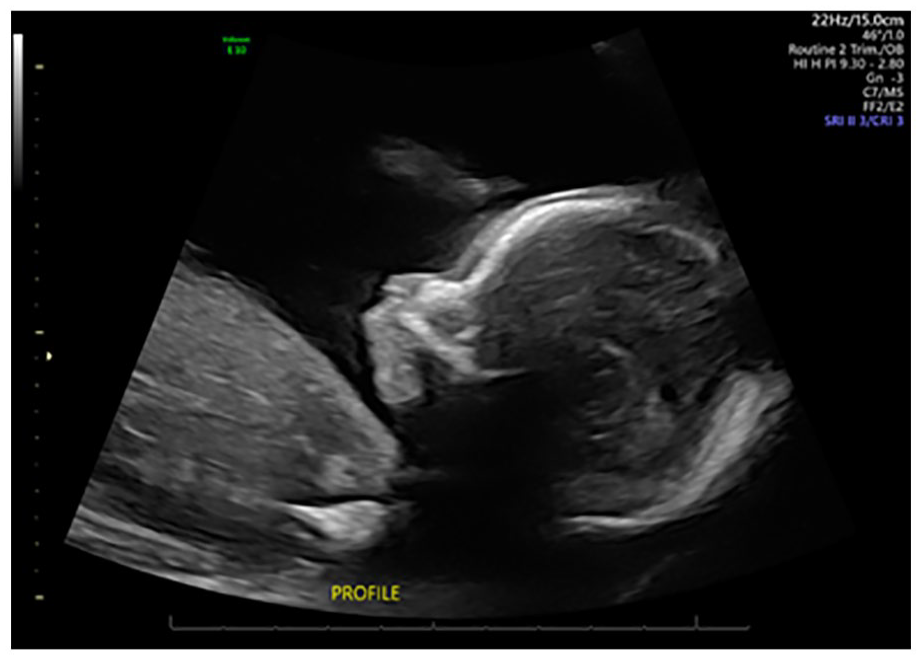
A sagittal sonographic view of the fetus provided the opportunity to make a subjective assessment of possible micrognathia.
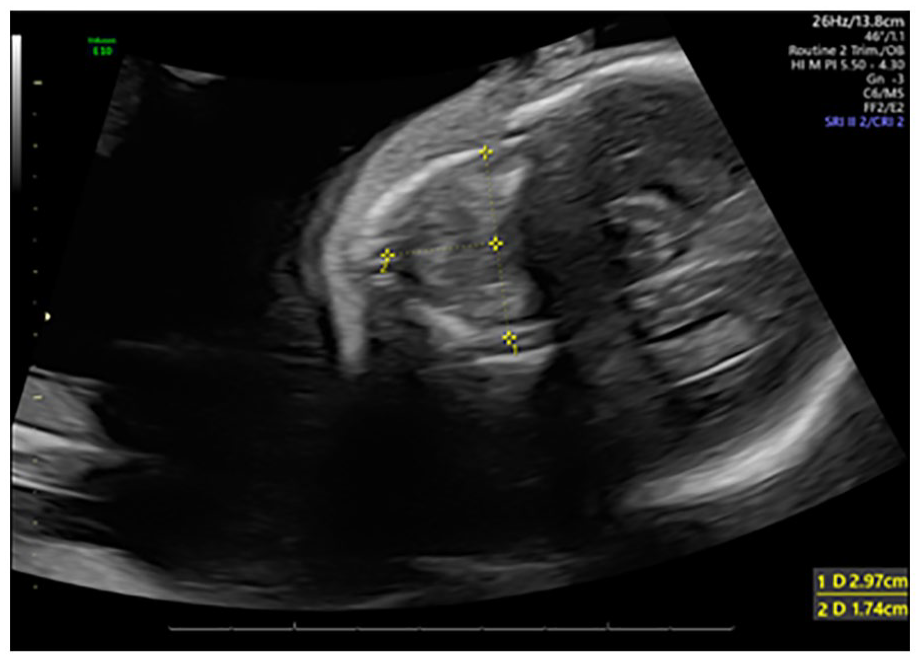
An axial sonographic view is provided of the fetal mandible and was used to measure and report the fetal jaw index.
Delivery occurred at 34 weeks via scheduled cesarean section with a modified ex utero intrapartum treatment (EXIT) procedure. A modified EXIT procedure was necessary in this case because of the compromised airway, due to micrognathia. A bilateral salpingectomy was also performed at the time of delivery. Postnatally, the diagnosis of micrognathia was confirmed. Trachea and enteric tubes were placed in the neonate to maintain the airway and provide nutrition. The neonate did not survive past the 17th day after delivery.
Discussion
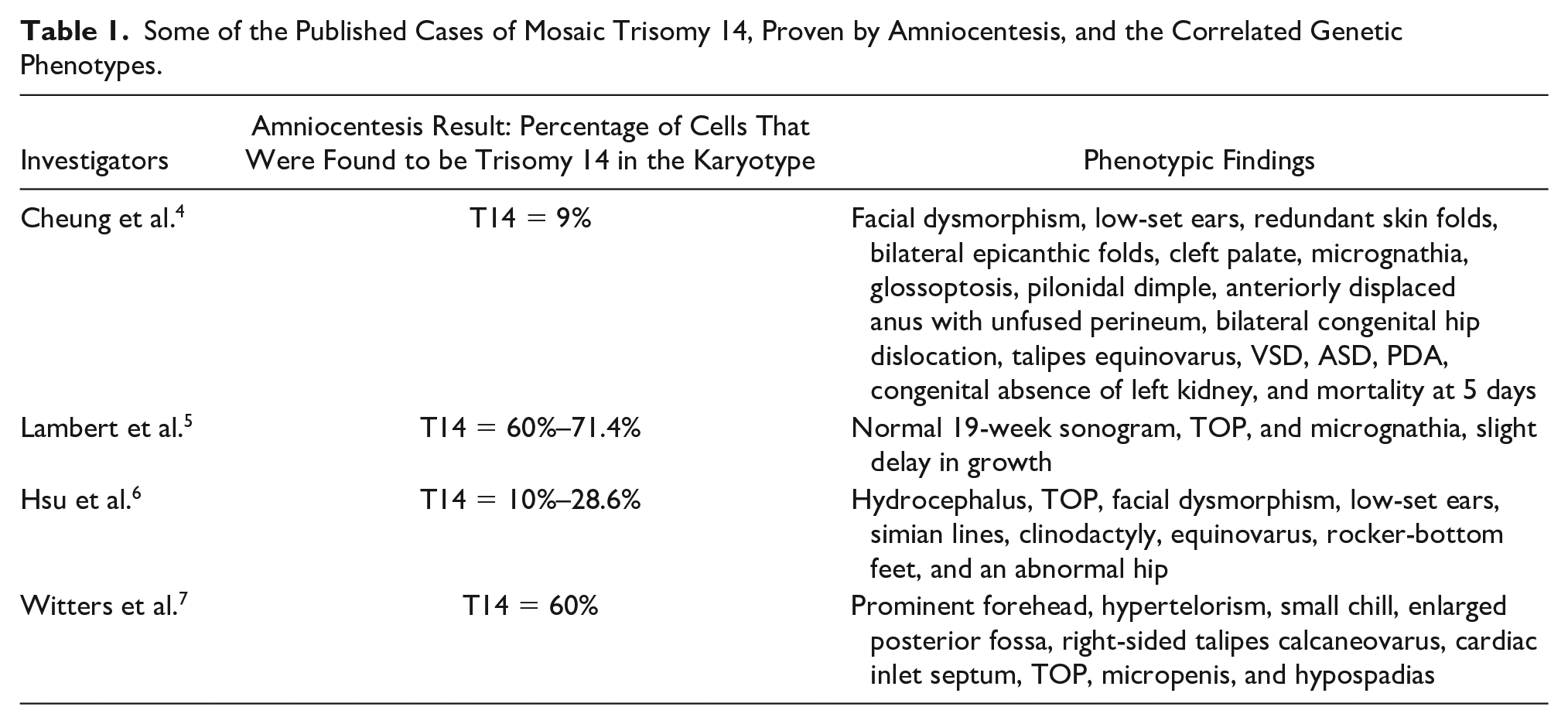
Trisomy is a genetic condition that occurs when one chromosome has three copies instead of the normal two. Errors in chromosome number occur during the nondisjunction phase of cellular division. Mosaicism occurs when only some cells contain an extra copy of the chromosome and other cells contain normal chromosomes. Partial or mosaic trisomy 14 is an extremely rare condition occurring when some cells contain an additional copy on the 14th chromosome. 1 The diagnosis of mosaic trisomy 14 is often made secondary to an abnormal set of sonographic findings, as well as amniocentesis. The phenotype of fetuses with mosaic trisomy 14 can vary greatly. The phenotypic appearance of the fetus is unrelated to the proportion of cells affected by trisomy. A table highlighting various phenotypes of mosaic trisomy 14 is provided based on a 2013 literature review by Cheung et al. (See Table 1). Based on the review by Cheung et al., phenotypes of low-set ears, cleft palate, bilateral hip dislocation, ventricular septal defect, hydrocephalus, rocker-bottom feet, and clinodactyly, among other appearances, can be observed.
Some of the Published Cases of Mosaic Trisomy 14, Proven by Amniocentesis, and the Correlated Genetic Phenotypes.
In the present case, the discovery of choroid plexus cysts, intracardiac echogenic foci, and growth restriction, at 18 weeks, prompted the need for an amniocentesis. Although these sonographic findings at 18 weeks prompted genetic testing, the finding of borderline micrognathia at 33 weeks may be the most significant diagnostic imaging finding in this case, due to the associated complications of trachea and esophageal obstruction. The jaw index is calculated based on the measurements taken (See Figure 7) and using the following equation:

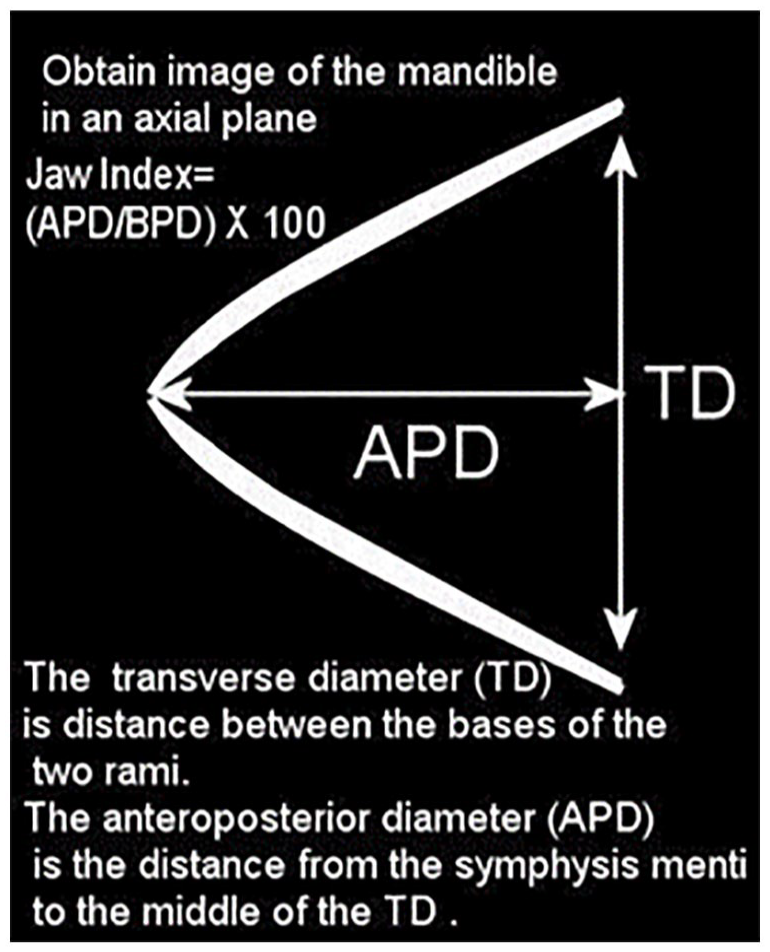
A diagram of the fetal mandible demonstrates how to accurately obtain a fetal jaw image and the measurements needed to calculate the jaw index.
The anteroposterior diameter (APD) can be measured on a cross-sectional view of the fetal mandible. The transverse diameter (TD) measures from the inner base of the two rami. The APD measures from the symphysis to the middle of the TD. Using the above equation, the jaw index in this case measured 25.6. A jaw index of less than 23 has 98.1% specificity in diagnosing micrognathia. 8
Two sonographic views are important in the detection of micrognathia: profile and mandible. The fetal profile provides a subjective view of the chin in relation to the rest of the face. A recessed or small chin should raise suspicion for micrognathia. A cross-sectional mandibular view allows for jaw index calculations which can provide an objective diagnosis of micrognathia.
The effects of micrognathia are variable depending on the severity of the associated fetal complications. Micrognathia can lead to polyhydramnios in utero due to glossoptosis. Glossoptosis describes a normal tongue obstructing a small mouth opening. This can lead to an obstruction of the trachea and esophagus, 9 resulting in an imbalance of amniotic fluid. Polyhydramnios is detected by an AFI greater than 25 cm. 10 Complications associated with severe polyhydramnios include fetal growth restriction, premature rupture of membranes, preterm labor, postpartum hemorrhage, abnormal fetal presentation, and prolapsed umbilical cord. 10
The prognosis for prenatal micrognathia is poor. A mortality rate of >80% has been reported due to associated chromosomal anomalies. Micrognathia is found in up to one third of triploidies. 9 Neonates born with micrognathia often have feeding and airway complications. Detection of micrognathia in utero is important so proper neonatal care can be prepared prior to delivery. An isolated finding of micrognathia can be surgically treated postnatally. A tongue-lip adhesion procedure can be performed in which the tongue is tied to the lower jaw to prevent glossoptosis. Mandibular distraction osteogenesis (MDO) may also be performed. An MDO procedure slowly lengthens the lower portion of the mandible, to relieve airway obstruction. 9
Polyhydramnios and growth restriction should always prompt prenatal suspicion of underlying trisomy. Early findings such as echogenic intracardiac foci and choroid plexus cysts in conjunction with growth restriction should elicit a recommendation of amniocentesis. Routine and frequent surveillance should be scheduled, which include the use of umbilical artery Doppler, throughout the remainder of pregnancy. Fetal echocardiograms are often recommended for fetuses with trisomy, due to their high risk of congenital heart defects, such as ventricular septum defect.⁷ Ex utero intrapartum treatment procedures are often recommended during delivery with known micrognathia in order to ensure a functioning airway is established before the umbilical cord is severed.
Conclusion
Mosaic trisomy 14 is a rare genetic condition with a wide range of associated anomalies and phenotypic appearances. Routine prenatal sonography is the most reliable way to characterize associated abnormalities and prompt further genetic testing. Micrognathia, severe polyhydramnios, and fetal growth restriction were all important prenatal sonographic findings that supported the diagnosis of mosaic trisomy 14 in this case. Early sonographic detection of mosaic trisomy 14, along with any corresponding anomalies, is vital for effective prenatal and postnatal management.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because all case data was de-identified.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified.