
Abstract
Placental chorangioma is a rare, benign tumor of the placenta. Chorangiomas are typically small, are asymptomatic, and pose no threat to pregnancy. However, in extreme cases, large placental chorangiomas can cause maternal and fetal complications associated with poor outcomes and fetal demise. Prenatal sonography is an accurate method for diagnosing these benign tumors based on grayscale imaging and color Doppler assessment of intratumoral vascularity. Early diagnosis is critical in predicting the potential for subsequent maternal and fetal complications, planning sonographic surveillance, treating maternal symptoms, and delivery planning. This case study discusses the diagnosis and management of a large placental chorangioma in an otherwise uncomplicated pregnancy.
Introduction
Placental chorangioma, also referred to in the literature as chorioangioma, is a benign, nontrophoblastic tumor of the placenta, occurring in approximately 1% of pregnancies.1-3 This tumor is thought to be associated with capillary and villous stroma hyperplasia and has been compared to a hamartoma, rather than a true neoplasm. 1 Documentation of sonographic diagnosis is limited because most chorangiomas are small and asymptomatic. However, large placental chorangiomas (greater than 4-5 cm in diameter) often result in fetal and maternal complications and account for the small number of case studies available. Since the first known sonographic diagnosis of a placental chorangioma in 1978 by Asokan et al, advances in resolution and color Doppler have considerably enhanced evaluation of placental lesions. 4 In 1994, Bromley and Benacerraf prospectively identified 10 cases of solid placental masses in gray scale ranging in size from 4 to 10 cm. 5 Results of this study revealed that the grayscale sonographic appearance of chorangioma was indistinguishable from that of placental hemorrhage and other lesions. It was speculated that color Doppler interrogation could have been valuable in differentiating these lesions. 4 Chorangiomas are definitively diagnosed with pathologic assessment but can be identified prenatally with routine sonographic examination of the placenta and presence of feeder vessels. Early diagnosis can greatly influence consequent fetal and maternal surveillance. Advanced maternal age, maternal hypertension and diabetes, female sex of the fetus, primipara pregnancies, and multiple gestation pregnancies are all associated with increased incidences of placental chorangioma. 6
Case Study
A 32-year-old pregnant woman, gravida 7, para 2 0 4 2, presented for a second trimester sonographic fetal anatomy evaluation. The patient’s history was significant for hypertension. The sonogram was performed using a Philips iU-22 ultrasound system (Philips Medical, Bothell, WA) with a C5-1 MHz transducer. Dating was consistent with the gestational age of 19 weeks 2 days and fetal weight measured in the 57th percentile. Fetal anatomy and growth appeared within normal limits. A hypoechoic lesion was visualized in the superior, fundal margin of the placenta measuring 1.9 × 2 × 1.7 cm with minimal vascularity (Figure 1 and Figure 2). Based on the patient’s history of low risk pregnancies and normal sequential screening values, the lesion was thought to be consistent with a venous lake. Placental venous lakes are avillous spaces that appear as hypoechoic, or anechoic, irregular shaped lesions in the placenta and are associated with favorable outcomes.7,8

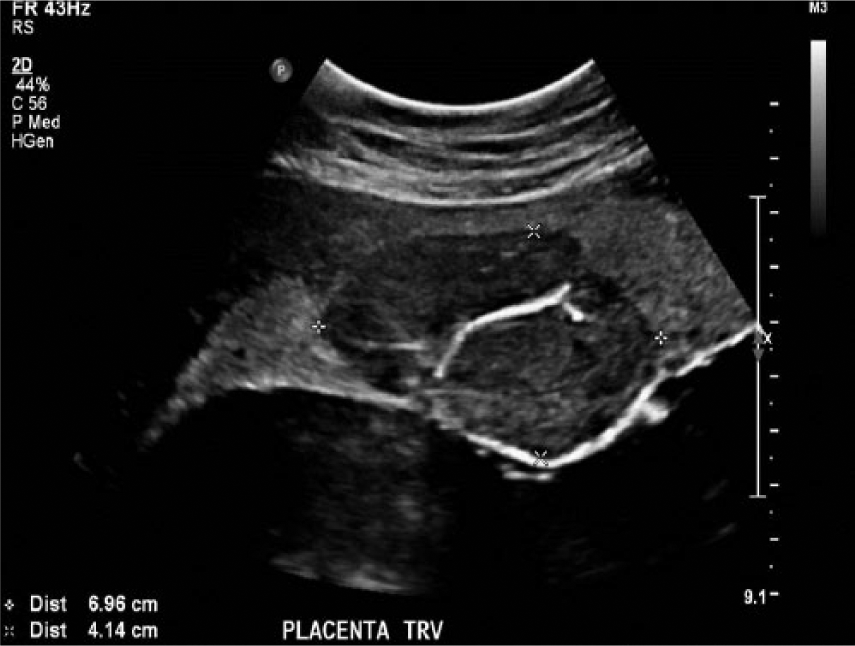
Transverse grayscale image of the hypoechoic lesion in the superior margin of the placenta at 19 weeks and 2 days (white arrow).
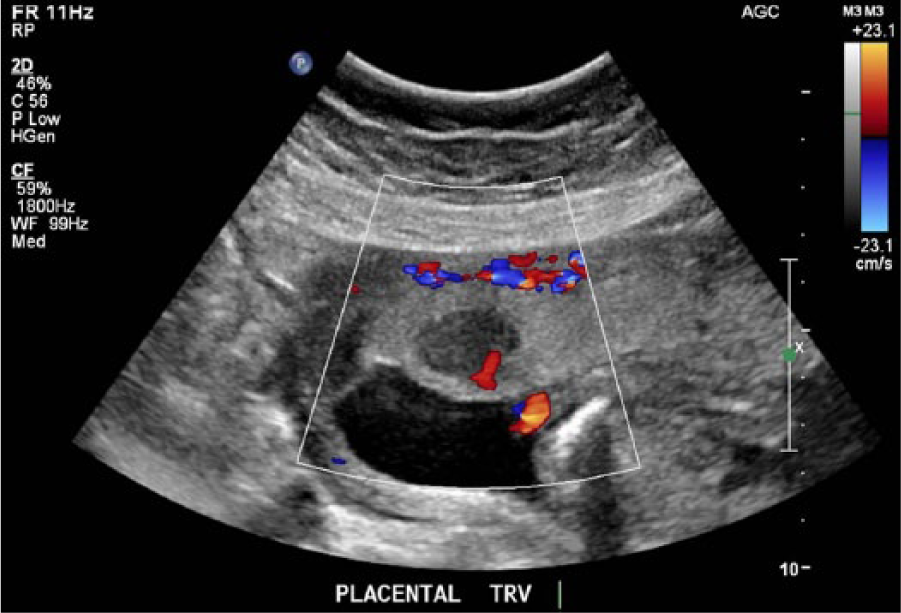
Transverse color Doppler image of the hypoechoic placental lesion showing minimal vascularity at 19 weeks and 2 days.
A follow-up sonogram was scheduled four weeks later for reevaluation of suboptimal fetal anatomy and surveillance of the lesion. This examination showed that the placental lesion had increased in size to 4.4 × 4.4 × 3.1 cm, but was still thought to be most consistent with a venous lake due to limited vascularity. Fetal weight measured in the 66th percentile and the amniotic fluid index (AFI) measured 22.5 cm, indicating borderline polyhydramnios. The patient was scheduled to return for a second follow-up sonogram in four more weeks.
At that time the size of the fetus was consistent with a gestational age of 27 weeks 2 days. Fetal anatomy was visualized and considered unremarkable. However, the patient presented with mild contractions and an AFI of 42 cm, indicating severe polyhydramnios. The placental lesion had increased significantly in size and vascularity, with the appearance of fibrous septa and a large feeding vessel (Figure 3 and Figure 4). These findings were more consistent with the diagnosis of a placental chorangioma. The new diagnosis put the fetus at risk for anemia and congestive heart failure. Therefore the patient was scheduled for a fetal echocardiogram. Weekly middle cerebral artery (MCA) and umbilical artery Doppler assessment and fetal Non-Stress Test (NST) surveillance were ordered. Preterm labor precautions were reviewed with the patient. The patient was counseled regarding amnioreduction procedures and she elected to undergo a therapeutic reduction which resulted in the removal of 900 milliliters of amniotic fluid.
Transverse grayscale image of the large placental lesion exhibiting a substantial increase in size at 27 weeks and 2 days weeks. The tumor is hypoechoic to the surrounding placental tissue and exhibits echogenic fibrous septa.
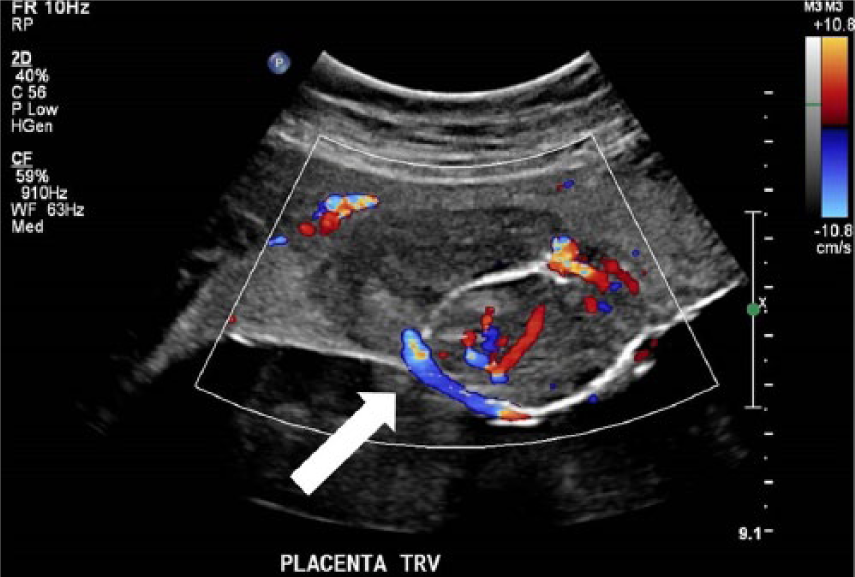
Transverse color Doppler image of the large placental lesion with a visualized feeder vessel at 27 weeks and 2 days (white arrow).
Four days later, the patient returned to clinic with complaints of increasing discomfort associated with recurrent polyhydramnios. A bedside sonogram revealed an AFI of 48 cm.
Again, the patient underwent an amnioreduction of three liters of amniotic fluid at 27 weeks 6 days. An additional four liters of fluid were withdrawn at 29 weeks 5 days. Fetal Dopplers were performed weekly and remained within normal limits through the remainder of the pregnancy. At 32 weeks 6 days the fetus was macrosomic, there was severe polyhydramnios, and the chorangioma now measured 6.5 × 7 × 4.1 cm. Over the course of pregnancy, the patient underwent four amnioreduction procedures with a total reduction of nearly 12 liters of amniotic fluid.
Following the final procedure, the patient was treated with betamethasone, in anticipation of preterm delivery. Before receiving her second dose of betamethasone, the patient did in fact go into preterm labor and delivered a viable female infant by a normal, spontaneous, uncomplicated vaginal delivery at 33 weeks gestation. The pathology report of the placenta confirmed the presence of a large, 6.7 cm chorangioma. There were increased levels of nucleated fetal red blood cells in the placenta and evidence of intravillous hemorrhage. Nucleated fetal red blood cells are rare in placental circulation after 28 weeks gestation, which suggested fetal stress associated with vascular perfusion to the large chorangioma. Abrupt changes in pressure across fetal vessels often results in intravillous hemorrhage, most likely a consequence of the patient’s substantial amnioreduction.
Discussion
Most chorangiomas are small and pose no risks to pregnancy. However, large placental chorangiomas are associated with maternal and fetal complications. Fetal complications include intrauterine growth restriction (IUGR), fetal anemia, nonimmune fetal hydrops, and congestive heart failure, secondary to the shunting of blood to a highly vascular chorangioma.2,3 Sonographic interrogation of the placenta is routinely obtained in any fetal sonogram regardless of gestational age. However, a small chorangioma could easily be overlooked or misdiagnosed as a venous lake. As in this case study, it is not uncommon for chorangiomas to appear unremarkable and asymptomatic early in pregnancy. However, large placental chorangiomas can grow exponentially with the placenta, resulting in late-onset symptoms such as polyhydramnios. It is important to be aware of placental masses upon sonographic examination due to their potential sequelae.
Sonographically, chorangiomas appear as well-circumscribed solid masses with fibrous septa and variable echogenicity compared to the placenta. They may exhibit increased blood flow and feeder vessels.1,6,9 The presence of significant blood flow rules out avascular differentials such as placental lake, hemorrhage, and hematoma, as well as other placental masses like myomas or teratomas. 1 Less perfused chorangiomas are associated with better outcomes and a decrease in blood flow over time can indicate an improved prognosis. 10 Hyperechoic echotexture of a tumor compared to the placenta typically indicates fibrous degeneration and is also associated with a more favorable outcomes as well. 11 Chorangiomas are most frequently located near the fetal surface of the placenta and less perfused areas of the placenta such as the chorionic plate and placental margins. 1 Several authors have correlated an increased incidence of chorangiomas with pregnancies at higher altitudes in association with decreased oxygen levels. 12 The majority of these diagnostic findings were consistent with the characteristics of the large chorangioma discussed in this case study. The lesion exhibited fibrous septa as well as a feeder vessel and its location was near the fundal margin of the fetal surface of the placenta. The patient’s residence throughout pregnancy was at an altitude of over 5000 feet above sea level.
Placental chorangioma is considered a nontrophoblastic tumor, but in the case of any placental mass, neoplastic proliferation cannot be excluded as a differential. Gestational trophoblastic disease (GTD) encompasses several perinatal placental and uterine tumors that vary in sequelae and are often associated with significant morbidity and mortality. This spectrum includes trophoblastic tumors, as well as partial and complete hydatidiform molar pregnancies. Trophoblastic tumors such as placental site trophoblastic tumor (PSTT) and choriocarcinoma may present with grayscale and color Doppler sonographic findings similar to placental chorangioma. These invasive neoplasms arise from placental trophoblast cells and can metastasize to other maternal organ systems. Clinically, PSTT and choriocarcinoma are associated with elevated human chorionic gonadotropin (hCG) and symptoms secondary to metastasis.13,14
If a large placental chorangioma is suspected, systematic surveillance protocols and treatment plans should be in place in the case of maternal and fetal complications. Highly vascular placental masses raise concern for fetal congestive heart failure secondary to the shunting of blood to the mass. Therefore, in the presence of a large, vascular chorangioma, a fetal echocardiogram should be performed and fetal Doppler assessment should be utilized to interrogate the umbilical arteries and vein and the middle cerebral artery. Absent or reversed end diastolic flow within the umbilical arteries is considered abnormal and typically indicative of poor perfusion to both the fetus and the placenta which is associated with IUGR. Normal umbilical artery flow can be seen in Figure 5. The middle cerebral artery is responsible for 80% of fetal brain circulation and normally exhibits high resistant, continuous forward flow (Figure 6). 15 In the presence of fetal hypoxia and stress from blood shunting, redistribution of blood flow, known as the brain-sparing reflex, increases flow to the brain, heart, and adrenals. Although subtle, this can be reflected in the middle cerebral artery with an increased peak systolic velocity or decreased resistive index.
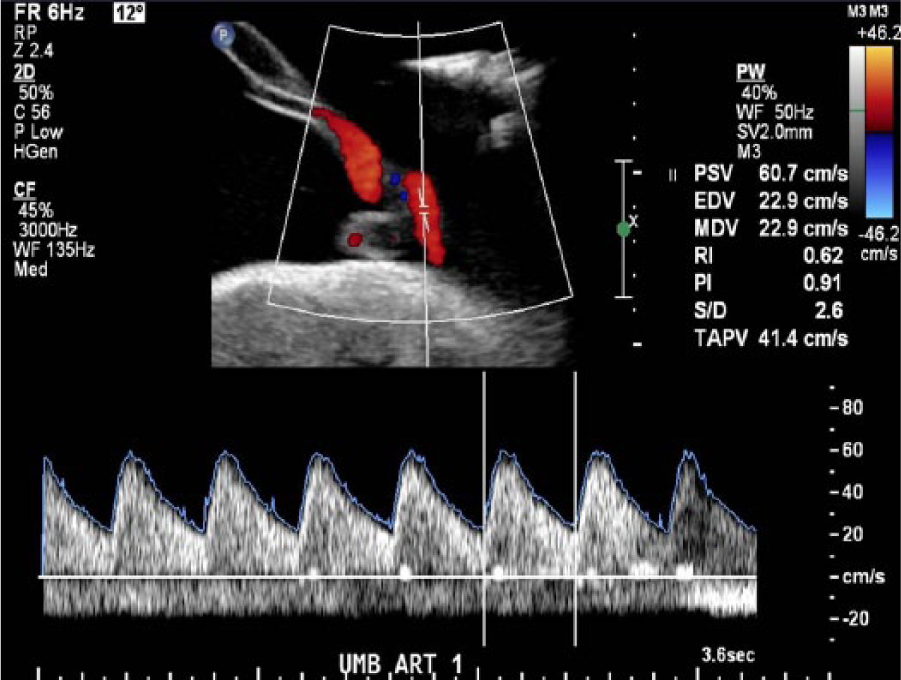
Normal, continuous forward flow in the umbilical artery.
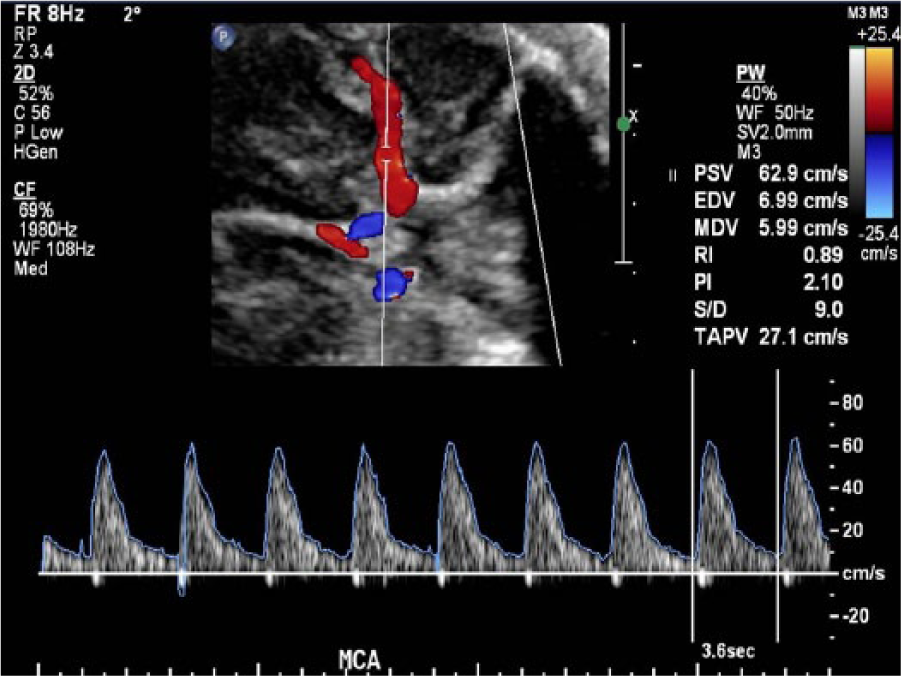
Normal, high-resistant, continuous forward flow in the MCA.
Unfortunately, the retrospective review of this case study was limited due to the lack of systematic evaluation of the chorangioma and its feeder vessel with spectral Doppler. There was not documentation of prenatal spectral Doppler interrogation despite the patient’s serial sonograms. Literature regarding this technique in the evaluation of placental lesions appears to be absent and its value in the diagnosis of these lesions is not definitively known. It is speculated that the presence of arterial and/or high-grade venous flow supports the diagnosis of a chorioangioma.4,5
As noted previously, large chorangiomas can also cause maternal stress, most commonly polyhydramnios. Polyhydramnios puts the mother at a higher risk for early uterine contractions, cervical insufficiency, placental abruption, cesarean section, and postpartum hemorrhage. 2 Appropriate interventions should be utilized as necessary to treat symptoms of polyhydramnionios and prevent preterm labor. Amnioreduction is a common practice for managing polyhydramnios associated with chorangiomas. There are reports that significant drops in intrauterine pressure from amnioreduction can result in increased tumor perfusion, known as the “steal” phenomenon, which can subject the fetus to hypoxia.16,17 If the vascularity of the chorangioma is causing significant fetal stress, intratumoral alcohol ablation and laser surgery have been successful in thrombosing blood flow to a large placental chorangioma. 18 Any invasive procedure poses some degree of risk to both the mother and the fetus, specifically the risk of infection and the transfer of toxic, ablative material into fetal circulation during an alcohol ablation treatment. 18 Procedural success can be evaluated with cordocentesis to assess a fetal blood sample for the presence of alcohol.1,18 The fetus should be monitored closely following any invasive procedure. 18
Conclusion
In conclusion, this case study emphasizes the importance of comprehensive sonographic evaluation in pregnancy, especially in the presence of a suspected placental lesion. Great care should be taken in evaluating the entirety of the placenta. Early in pregnancy, placental chorangiomas may appear as asymptomatic, unremarkable findings. However, there is potential for significant progression in size and vascularity which can result in late-onset fetal and maternal complications. Early identification of a large chorangioma aids in consequent fetal surveillance, management of maternal symptoms, and delivery planning discussions.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.