
Abstract
A sacrococcygeal teratoma (SCT) is one of the most common fetal extragonadal germ cell neoplasms and carries high risk of maternal and perinatal complications. An example of a fetal SCT, associated with polyhydramnios, is presented in this case report. An antenatal surveillance sonogram revealed an increase in the size of the teratoma size and the amniotic fluid index. The patient underwent Cesarean delivery and postnatally, the infant’s teratoma was surgically excised. The pathologic examination of the specimen revealed a benign mature teratoma. This case demonstrated the important role that serial sonography had in monitoring this fetal pathology. Prenatal fetal sonographic assessment can play an important role for patients who need counseling and surgical planning.
Keywords
A sacrococcygeal teratoma (SCT) is a rare fetal neoplasm, with an incidence of 1 in 20 000–1 in 40 000 live births and is derived from embryonic pluripotent stem cells, in the Henson node, at the front of the coccyx.1,2 It is the most common congenital tumor affecting a fetus and carries a high risk of perinatal complications. 3 Perinatal mortality may result from tumor rupture, hemorrhage, labor dystocia and preterm labor, which can cause associated polyhydramnios or uterine distension, from the tumor. 3 Generally, SCT is more prevalent in a female fetus with a female to male ratio of 3:1.4,5 However, a male infant diagnosed with SCT is more commonly affected by a malignant degeneration.6,7
Sacrococcygeal teratoma is of unknown etiology and can be detected prenatally with sonography, as early as 13-week gestation. 1 When the teratoma is detected, it is described as cystic, solid, or having mixed components, and most of these are identified with cystic components.1,8 Commonly, a teratoma with cystic components are benign and have an excellent prognosis.1,8 In contrast, a smaller percentage of cases (1%–2%) have a malignant potential with a poor prognosis.2,3 Malignant tumors, such as a yolk sac tumor, choriocarcinoma, and an embryonal carcinoma have been reported. 9 Histologically, SCT can be classified into three categories: mature teratomas, immature teratomas, and malignant teratomas.6,7 SCT can result in several complications, such as hydrops fetalis, high output cardiac failure, placentomegaly, and fetal demise. 3 A lack of early detection is associated with increased risk of fetal morbidity and mortality highlighting the importance of initial screening and diagnosis, to determine prognosis and clinical outcomes. 1
According to the Altman Classification of the American Academy of Pediatrics Surgical Section, SCTs are classified into four types based on location:2,10
Type I. The mass predominantly external with a small presacral component. Type I being the most common type reported (46%).
Type II. The mass predominantly external with significant intrapelvic component. Type II being the next likely type reported (35%).
Type III. The mass partially exterior but predominantly intrapelvic with abdominal extension. Type III being the least likely form reported (9%)
Type IV. The mass being entirely within the pelvis and abdomen with no external components. This type also being a more uncommon form reported (10%).
Sacrococcygeal teratoma is rarely associated with chromosomal abnormalities among the few cases that have been reported. 11 One case study documented an incidence of SCT that was associated with Trisomy 13 and was confirmed with cell-free fetal DNA and amniocentesis. 11 In addition, two case reports that documented, in Turkey and Central Africa, newborns with clinical features of Trisomy 13 were postnatally found to have SCT, likely due to a lack of resources. 11 Moreover, SCT has been reported to be associated with other congenital anomalies, such as myelomeningocele and vertebral malformations. 9
An obstetric sonogram is an essential diagnostic tool in tumor assessment and monitoring during pregnancy, as well as detecting those at increased risk for complications that may require a multidisciplinary intervention. 6 If a teratoma is suspected, a multidisciplinary team, including obstetricians, neonatologists, pediatric neurosurgeons, pediatric surgeons, radiologists, and oncologists, must establish a combined diagnostic and treatment plan. 12
Case Report
A 35-year-old female, G3 P2 A0 L2, was referred to a Kuwait maternity hospital, at 29 weeks and 4 days of gestation, for evaluation of a large cystic lesion, in the fetal sacral region. The patient’s medical history was significant for long-term hypertension and adult polycystic kidney disease. Detailed sonographic evaluation in the maternal fetal medicine unit revealed a mass, extending from the fetal spine, which was contained within the pelvis. The mass measured (8.26 × 7.0 × 6.37 cm). with multiple cystic compartments and lacked internal vascular flow or solid components (see Figure 1). The fetal bladder appeared small and compressed, both kidneys were normal, and no intra-abdominal component of the mass was noted (see Figures 2 and 3). The amniotic fluid index (AFI) was 37.1 cm, which indicated polyhydramnios (see Figure 4). Fetal biometry revealed a single living fetus matching the expected gestational age and had an estimated fetal weight of 1.278 kg (14%). There were no diagnostic signs of hydrops or placentomegaly noted, as part of the assessment. The sonographic findings were highly suggestive of an SCT.
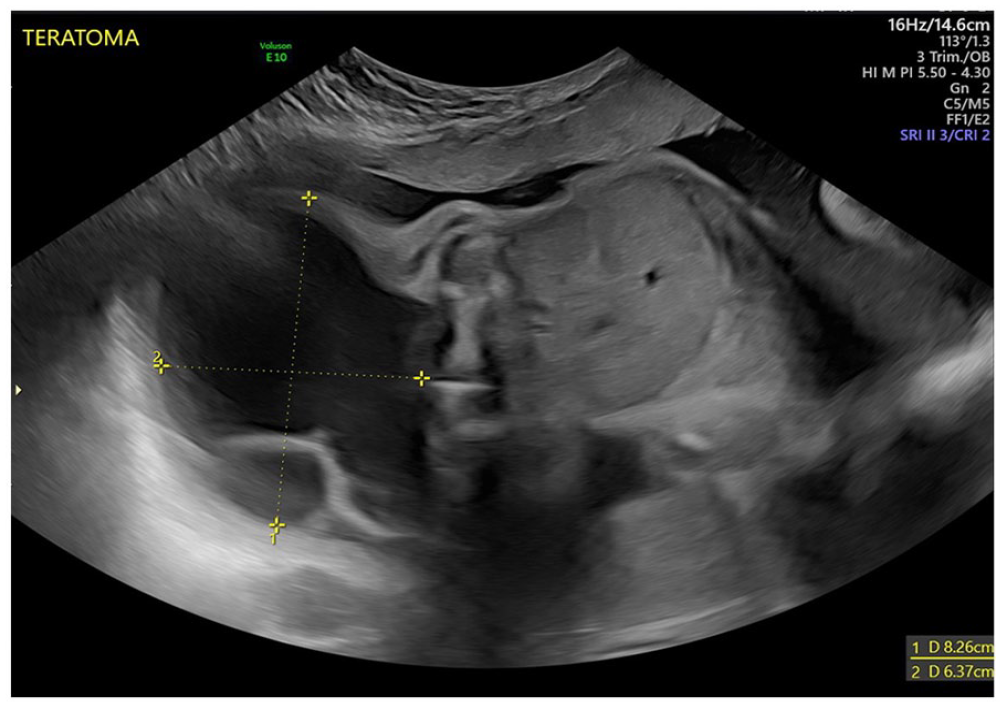
A sonogram taken at 29 weeks and 4 days of gestation, and demonstrates a fetal sacral mass measuring 8.26 × 7.0 × 6.37 cm.
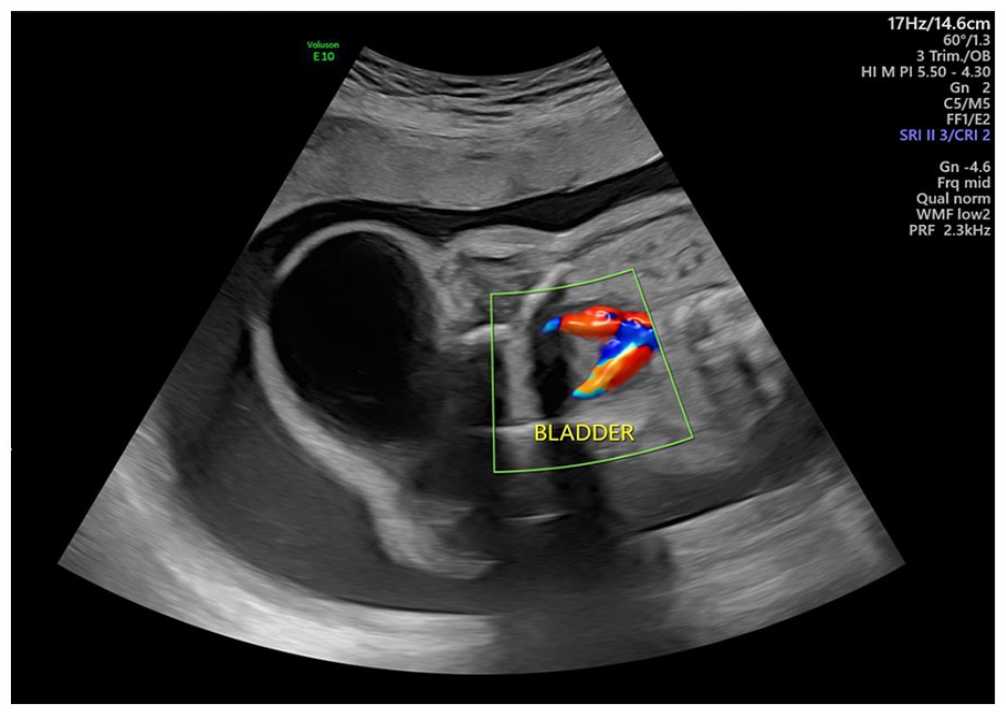
A sonogram shows the compressed and small urinary bladder of the fetus.
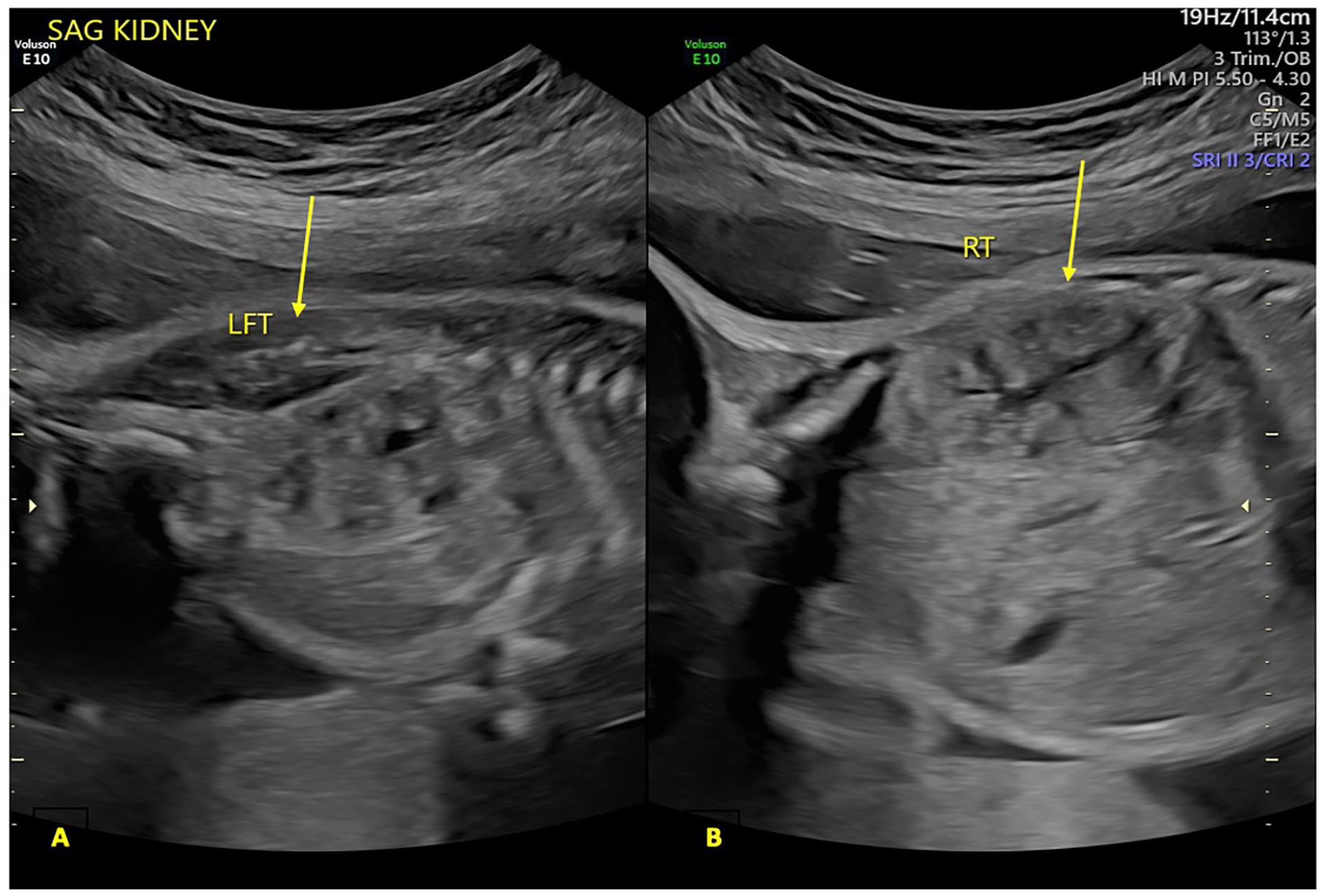
A sagittal sonographic view documents normal fetal kidneys bilaterally. The arrows are used to indicate the left (A) and right (B) kidneys.
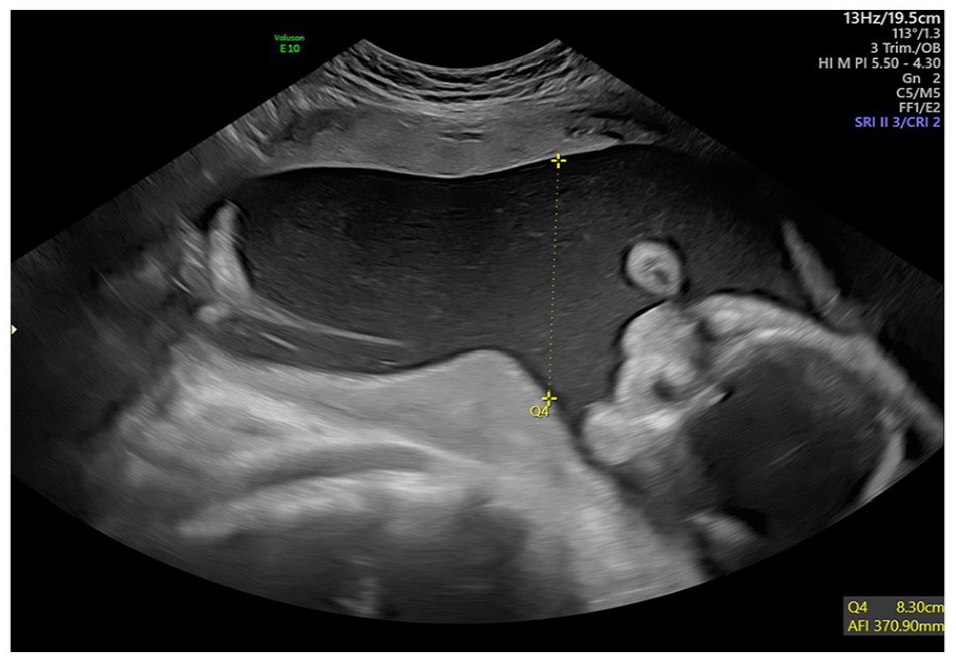
A sonogram taken at 29 weeks and 4 days of gestation, which shows evidence of polyhydramnios with an amniotic fluid index measuring 37.1 cm.
A subsequent sonogram was conducted at 36 weeks and 4 days of gestation, and demonstrated an increase in the size of the teratoma, increased to 12.19 × 11.17 × 12.53 cm and AFI elevated to 46.6 cm (above 97.5th percentile) (see Figure 5). At 37 weeks of gestation, after establishing fetal lung maturity and following proper counseling, an elective Cesarean delivery was performed. A live female infant, in breech position was delivered and had a birth weight of 3530 kg. The infant’s Apgar score was 7 at 1 minute and 9 at 5 minutes, however, a huge sacral mass was noted. The neonate was reviewed by the pediatrician and admitted to the neonatal intensive care unit. In addition, a postnatal review was completed by the pediatric surgeon and fetal magnetic resonance imaging (MRI) was ordered, which confirmed the diagnosis of SCT type I, based on the Altman classification system (see Figure 6A). Surgical resection of the teratoma was performed on day 14, postnatally. The postoperative pathology report, on the specimen, described a mature cystic teratoma. A subsequent fetal MRI was done postoperatively conducted and revealed a complete teratoma excision, with no residual disease (see Figure 6B).
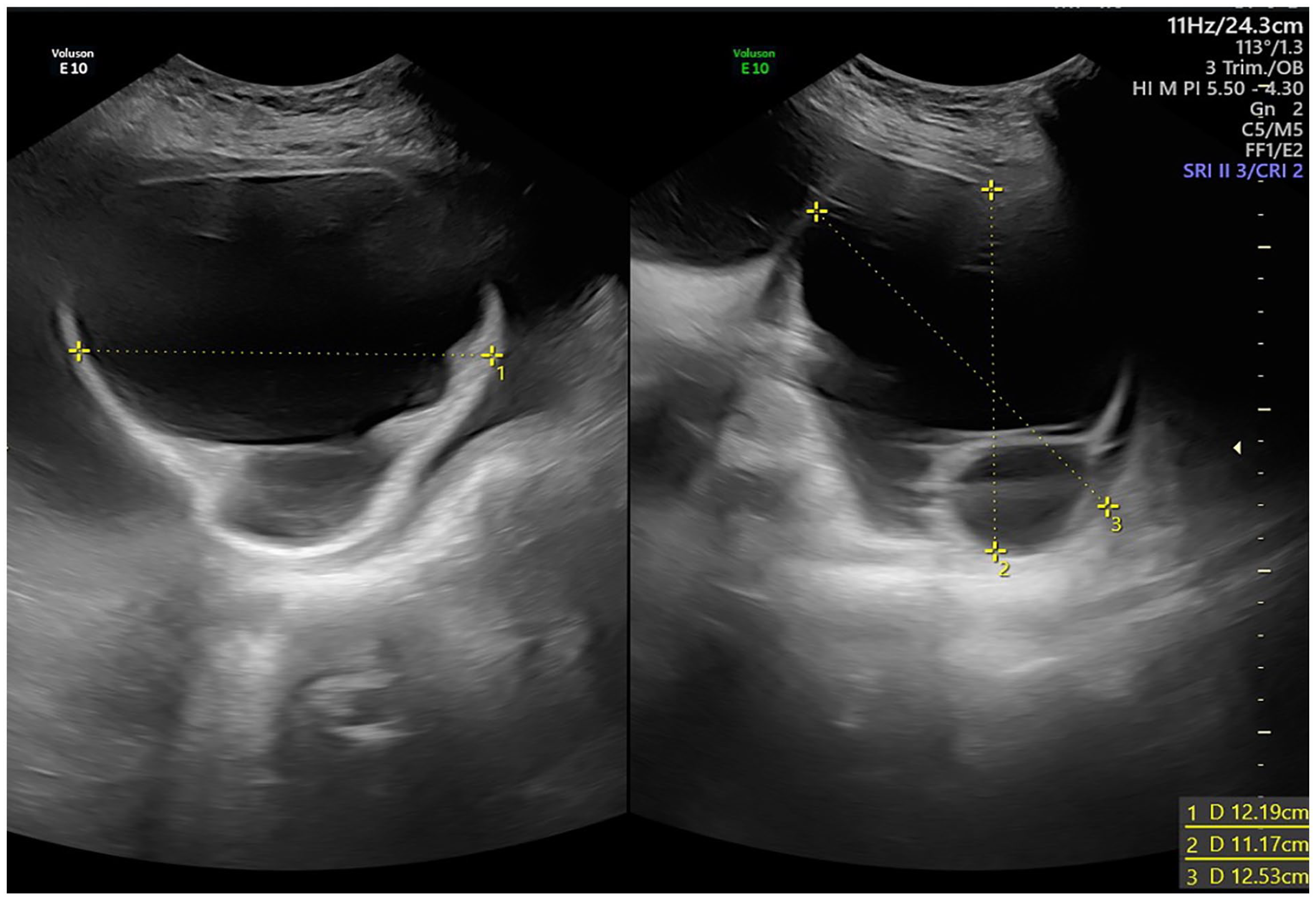
A subsequent sonogram taken at 36 weeks and 4 days of gestation that demonstrates the teratoma increasing in size and measuring 12.19 × 11.17 × 12.53 cm.
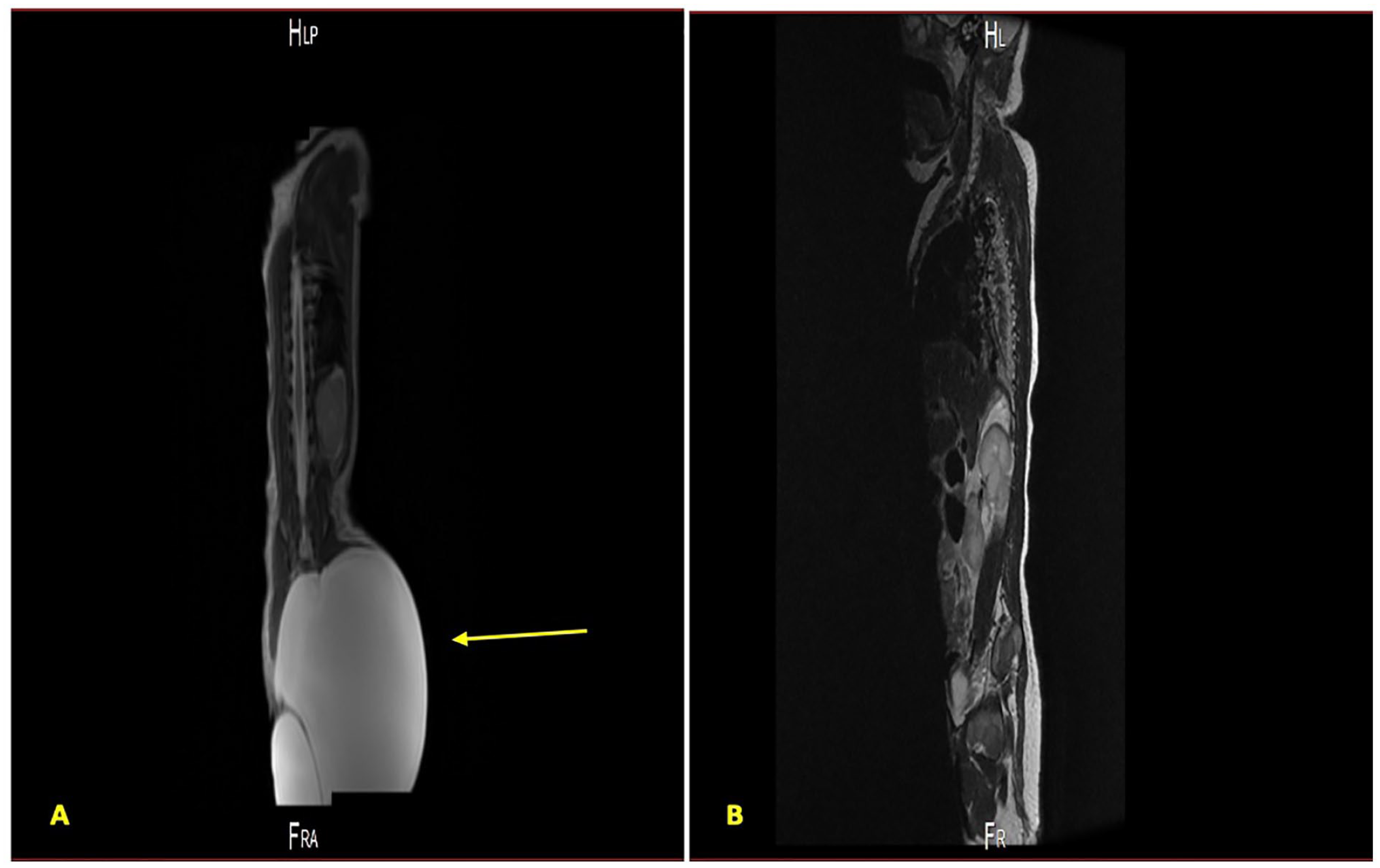
Magnetic resonance imaging of the sacrococcygeal teratoma conducted preoperatively (A) and postsurgical resection (B). The arrow is used to indicate the area of the sacrococcygeal tumor on the preoperative image.
Discussion
A case of SCT was provided that was correctly diagnosed, based on the third-trimester sonogram, monitored with subsequent sonograms, and resulted in a full-term Caesarean section (CS) delivery. The treatment of this infant’s SCT was marked by a successful multidisciplinary approach, which contributed to a good maternal fetal outcome.
Fetal SCT is the most common congenital tumor in a fetus. 13 Sonography is the diagnostic gold standard for detection and surveillance of SCT and to determine fetal prognosis. 13 With the recent advances in ultrasound equipment systems and specialized maternal fetal medicine physicians, those patients who can access these medical resources are unlikely to experience maternal fetal complications. 14
It has been reported that 50% to 80% of patient cases are diagnosed prenatally, usually after 22-week gestation, however, this fetus was diagnosed at 29+4 weeks.8,15 Most teratomas are about 7 to 8 cm in size at initial diagnosis, which is consistent with this report of an SCT that was 8.26 × 6.37 cm., when first detected. 8 A prospective study was done by Yadav et al., 5 which showed that almost two thirds of SCT were either Altman type I or II. This compares with the present case that was also a type I. Yadev et al. 5 also documented that most teratomas are mature, confirmed by histopathology and this is also consistent with the present case. Clinical manifestation of the teratoma in the present case included a sacrococcygeal mass, which matches most of the teratoma cases. 9 Teratomas can be asymptomatic or may cause rectal or bladder obstruction, related to tumor growth. 7 Rapid growth of the mass may cause pressure on adjacent organs, such as rectum or bladder resulting in organ dysfunction (e.g., fecal or urine incontinence). 12
Several parameters can be used to predict the prognosis of SCT. Gestational age at diagnosis is one parameter indicating the earlier the gestational age at diagnosis, the worse the prognosis. Other factors include sonographic findings of hydrops fetalis, placentomegaly, cardiomegaly, low birth weight, and polyhydramnios.8,15,16 In addition, increased rate of tumor growth, solid components, highly vascularized tumors, and high tumor volume index (TVI) > 60 cm3/cm (TVI = largest tumor diameter/head circumference) are considered as predictors of poor prognosis. 15 It has been suggested that polyhydramnios associated with SCT can result from direct transudation into the amniotic fluid and fetal polyuria, secondary to hyperdynamic circulation. 17
A Cesarean birth is the preferred mode of delivery for a tumor diameter greater than 5 cm, as it can avoid labor dystocia, tumor rupture and postpartum hemorrhage.1,16 A vertical uterine incision is the optimal Cesarean approach to reduce fetal injury and tumor rupture risk. 8 Malignant transformation occurs in 20% to 40% of patients within 2 to 4 months, respectively. 1 As a result, postnatal surgical intervention should be done as soon as possible to improve the survival rate from 92% to 95%. 1 Three surgical approaches based on tumor size, site, and relation to vital structures suggested: posterior-sagittal, posterior sacral (Chevron or inverted V-shaped incision), and combined abdominal sacral. 5 A posterior sacral approach provides an excellent surgical exposure for local resection. Whereas, combined abdominal sacral approach is suitable for tumors extending beyond the sacral promontory. 5
A benign lesion can be managed with coccygectomy for simple mass excision, while a malignant lesion should be managed with surgery and cisplatin-based chemotherapy. 5 Consideration of tumor recurrence is essential, so that, complete surgical resection is important. 1 In cases of tumor recurrence, surgery combined with chemotherapy is recommended. 1 Recurrence rate following teratoma resection has been reported as 7% to 10% of cases.5,16 Recurrence can be suspected based on palpation of abnormal mass, per rectal examination, and confirmed by computed tomography, as well as a rapid increase in serum alpha fetoprotein (AFP).5,16 Half of the malignant recurrences have high long-term survival rates due to these tumors being chemotherapy sensitive. 16 The most common risk factors for recurrence includes residual coccyx and tumor rupture during surgery. 6
A 3-year postoperative surveillance should include serum AFP, beta-human chorionic gonadotropin, and physical examination, every 3 to 6 months, as well as assessing the risk for surgical complications, recurrence, residual tumor, and malignancy.7,9,12 Long-term surgical complications have been reported, including urologic and anorectal dysfunction with an incidence of 33% and 29%, respectively. 5 This case report discussion has the limitation that sources published in English were used for references, which may have resulted in missing information and or knowledge gaps.
Conclusion
Teratomas are the most common germ cell tumors of the sacrococcygeal region. Serial sonograms conducted by qualified personnel, using modern ultrasound equipment systems, is critical in the diagnosis and management of any type of fetal congenital abnormality, including SCT. To avoid possibly serious maternal fetal complications, attention should be paid to the patient’s conditions with close obstetrical monitoring. Planning an appropriate procedure and timing postnatally would be suggested. As demonstrated in the current patient case, obstetric sonography provided a prenatal diagnosis and was an important diagnostic tool in the evaluation and surveillance of the tumor, throughout the pregnancy. Sonography can be critical in identifying a fetus at increased risk for complications and in planning a multidisciplinary clinical team approach, as appropriate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the present study because it is a case report, and the Ministry of Health Research Department allows either verbal or written consent to be obtained prior to chart review and writing the paper.
Informed Consent
Verbal informed consent was obtained from all subjects before the study.