
Abstract
Objective:
Published research exists that investigates placental location, as well as maternal and fetal outcomes. It is posited that placental location could be an indicator of subsequent maternal and or infant outcomes that could be identified and proactively treated. The aim of this study was to determine whether indeed there is an association between placental location and specific maternal or fetal outcomes.
Materials and Methods:
A retrospective chart review was conducted on 361 women, who delivered and had obstetric sonograms in a New York academic hospital, between June 2019 and December 2020. The study variables compared to placental location were maternal demographics, substance use during pregnancy, body mass index, blood type, parity, prenatal care, rupture of membranes, mode of delivery, postpartum hemorrhage, systolic/diastolic (S/D) ratio of the umbilical artery, placental location, gestational age at delivery, birth weight, Apgar scores (1 and 5 minutes), and fetal gender.
Results:
Statistical significance was appreciated in the 5-minute Apgar score category between anterior and posterior placentas (P = .03).
Conclusion:
Further prospective research is needed to determine whether different placental locations indeed has an effect on maternal or neonatal outcomes, in which case women may benefit from more intensive pregnancy monitoring.
During the second and third trimester of pregnancy, screening sonograms have become the standard for obstetric management. Sonography is a diagnostic medical imaging technique that uses safe, high frequency, non-ionizing radiation to produce diagnostic images of internal structures, within the human body. These screening sonograms are crucial in obstetric management as they include an evaluation of fetal growth, estimated fetal weight, amniotic fluid volume assessment, cervical length measurement, gestational dating, placental location, and overall anatomic assessment of the maturing fetus.
Published literature has shown that the determination of placental location is of great importance,1,2 as implantation sites may predict adverse pregnancy outcomes.3,4 Examples of negative outcomes are fetal distress, infection, intrauterine growth restriction (IUGR), and fetal demise.5 –9 In addition, fetal complications have been reported to be associated with specific placental implantation sites.3,4
The placenta plays a pivotal role during gestation as the major determinant of pregnancy maintenance, fetal growth, and labor onset.1,2 The site of implantation and resultant location of the placenta, within the uterus, are likely important determinants of placental blood flow and pregnancy success. 3 The primary vascular supply of the uterus is received through the uterine arteries bilaterally. The blood flow is unevenly distributed in the uterus, leading to varying levels of vascular supply to the placenta, as dictated by the implantation site. For example, when the placenta implants on the lateral uterine wall, it will be supplied by only one of the uterine arteries. This can lead to elevated resistance in the placental vascular bed.
Although a substantial body of research exists regarding placental location and pregnancy outcomes, most of these studies focus on concerning placental conditions, such as low-lying placentas or placenta previa, vasa previa, and abnormally invasive placentas (i.e. accreta, increta, percreta), and their associations with the increased risk of maternal and fetal morbidity and mortality.4,8 –12 However, limited research has been conducted to explore the impact of normal placental locations on pregnancy and neonatal outcomes, particularly within the United States.
The human blastocyst normally implants in the upper portion of the uterus, establishing the future site of the placenta for that pregnancy. 13 Placental development can occur in various normal locations: anterior (See Figure 1), posterior (See Figure 2), fundal, and right and left lateral walls of the uterus. 14 According to the literature, fundal implantation seems to increase the incidence of premature rupture of amniotic membrane and shorter duration of the third stage of delivery (delivery of the placenta). 15 Lateral placental implantations have been associated with an increased incidence of preeclampsia, fetal distress in labor, caesarian section, fetuses measuring small for gestational age, low Apgar scores, IUGR,4,6,7,16 and gestational diabetes. 17 Anterior placentas tended to be linked with a higher frequency of postpartum hemorrhage (PPH), shorter gestational age, lower birth weight, lower Apgar score, higher prenatal bleeding rate, longer duration of hospitalization, and higher blood transfusion and hysterectomy rates, pregnancy-induced hypertension, gestational diabetes, placental abruption, IUGR, increased uterine resistance, and fetal demise.3,18 –20 Eccentric, or cornual-fundal, implantations have shown an association with an increased risk of breech presentation. 21 Fetuses presenting in the persistent occiput posterior position were more frequently associated with an anterior placenta.18,19 Women with posterior placentas seemed to have fewer reportable associations in the literature. Posterior placentation has been linked to an increased risk of premature delivery 3 and increased uterine resistance.3,20

A sonographic example of an anterior placenta.

A sonographic example of a posterior placenta.
The overarching aim of this study was to determine the association between normal placental locations and maternal and fetal outcomes.
Materials and Methods
Researchers from a diagnostic medical imaging program collaborated with the obstetrics and gynecology (OB/GYN) department (including the OB/ GYN sonography lab and the Labor and Delivery Unit) to conduct this study. A retrospective cohort study design was employed, involving the review of electronic health records for patients who delivered at a New York university hospital between June 2019 and December 2020.
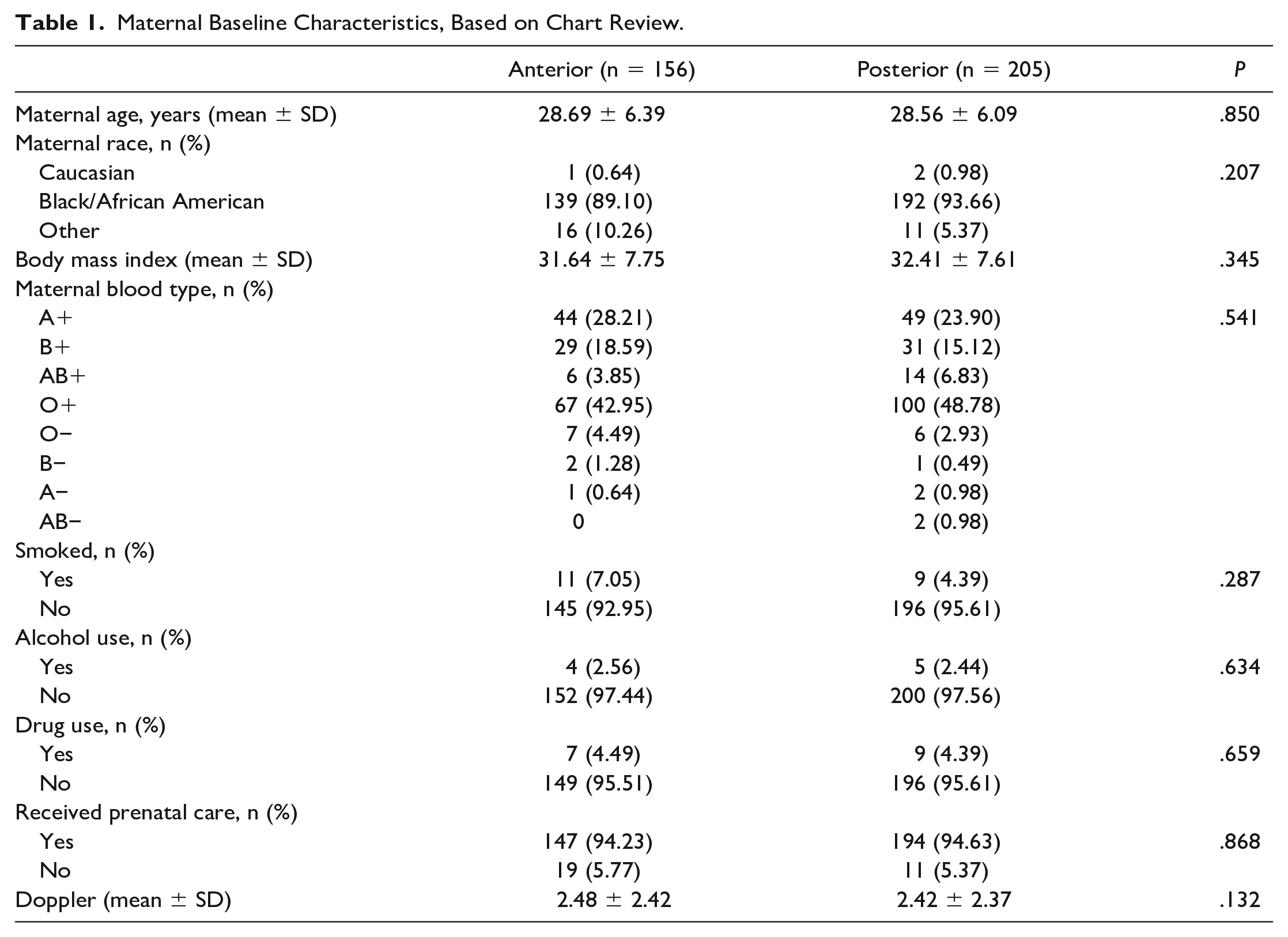
This study included files of patients who had a second or third trimester sonogram (18 weeks gestational age or later), delivered at the hospital, and had data on outcomes of interest. Data collected included maternal characteristics such as demographics, substance use during pregnancy, body mass index (BMI), blood type, parity, and whether or not they received prenatal care during this pregnancy (See Table 1). The type of maternal outcomes collected included the type of rupture of membranes, mode of delivery (vaginal, cesarean section, etc.), the volume of postpartum blood loss, systolic/diastolic (S/D) ratio of the umbilical artery, and placental location, as determined by second or third trimester ultrasound (See Table 2). The placental location was retrieved from the sonographic report, as reviewed by the department’s maternal-fetal medicine physician. The S/D ratio was obtained by the researchers through review of sonographic images of the included participants. Fetal outcomes collected included gestational age at delivery, birth weight, Apgar scores at 1 and 5 minutes, and gender (See Table 3). Pregnancies presenting with preeclampsia/eclampsia, hypertension, diabetes, fibroids, fetuses with congenital or chromosomal anomalies, multiple gestation, fetal demise, placenta or vasa previa, abnormally invasive placentation (placenta accreta, increta, percreta), hemolysis, elevated liver enzymes, low platelets syndrome (HELLP), and uterine anomalies were excluded from this study. The hospital’s Institutional Review Board approved the study (IRB).
Maternal Baseline Characteristics, Based on Chart Review.
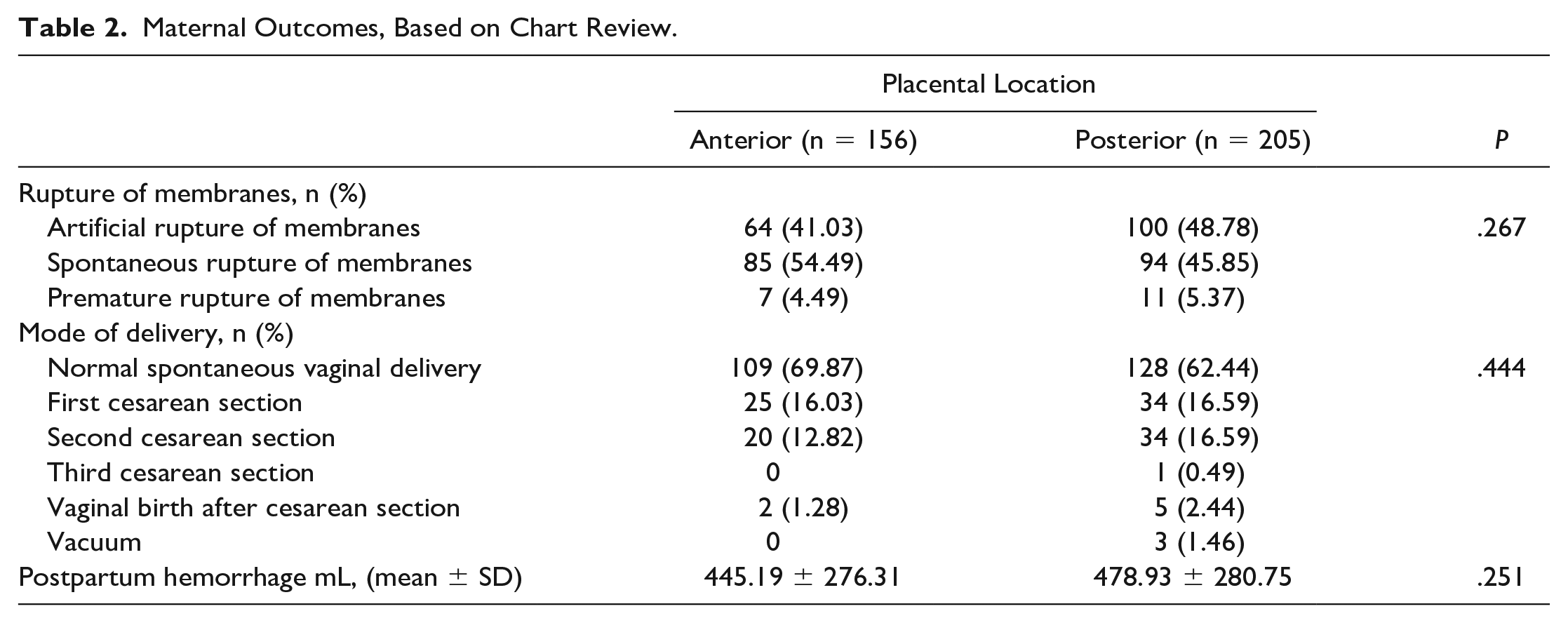
Maternal Outcomes, Based on Chart Review.
Newborn/Fetal Outcomes, Based on Chart Review.
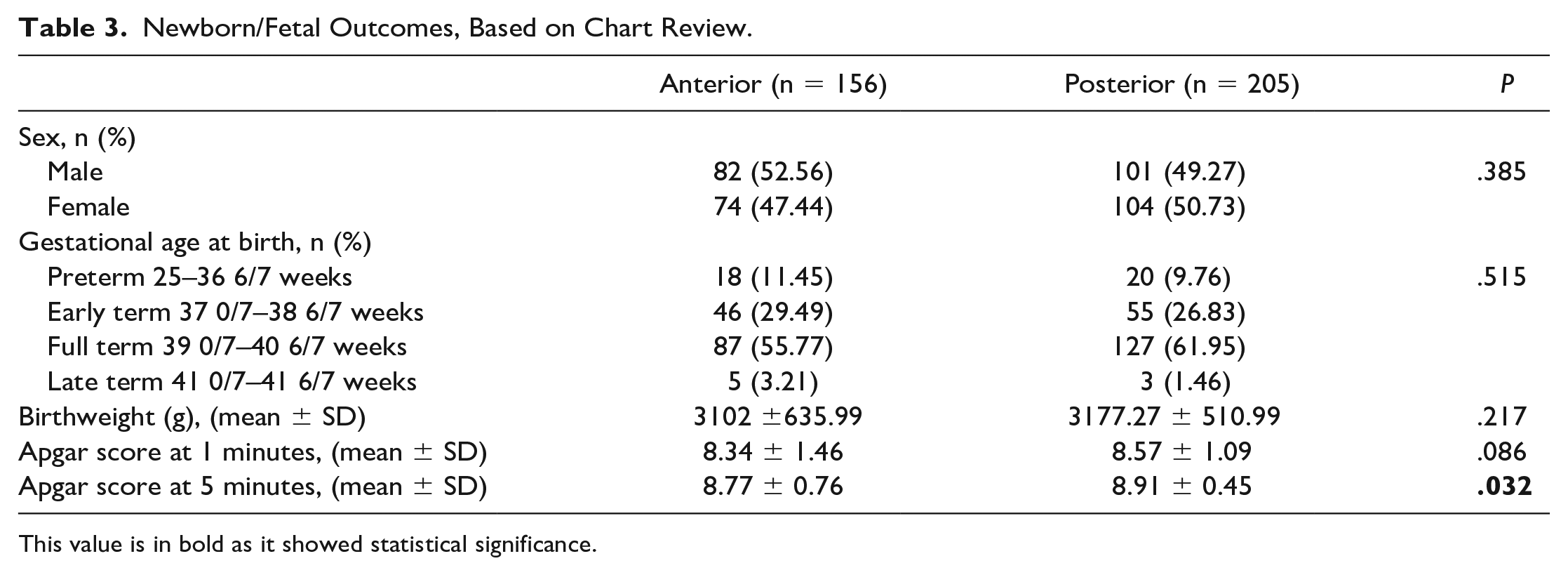
This value is in bold as it showed statistical significance.
Statistical Analysis
Data analysis was conducted using STATA 18 statistical software. Descriptive statistics included mean, median, standard deviation, frequency, and percentages. Proportions were compared using the chi-square test, and means were compared using a t-test.
Researchers analyzed individual variables with descriptive statistics to assess the effect of placental position on both maternal and fetal outcomes, examining the distribution of each variable. Statistical significance was assessed in bivariate analyses using the chi-square or Fisher’s exact test, as appropriate. A P value of .05 was considered statistically significant.
Results
A total of 438 patient charts were reviewed for women who had delivered between June 2019 and December 2020. Due to the absence of essential data within the medical records, the analysis was based on 361 complete patient charts. Of the 361 patient cases analyzed, 156 (43.21%) were identified with an anterior placental location and 205 (56.79%) with a posterior placental location. The results of this study did not yield any patients with a lateral, fundal, or eccentric placental location. Table 1 provides the baseline maternal characteristics. The maternal mean age was 28.62 (median of 28) years, and 91.69% of the participants were African American/Caribbean American. Overall, maternal mean weight was 189.55 pounds (median of 182 lbs.). In the sample analyzed, 261 participants (72.30%) had at least one prior term pregnancy, 29 (8.03%) had at least one prior preterm pregnancy, 165 (45.71%) had at least one prior abortion, and 228 (64.16%) had at least one prior live birth. The majority of participants attested to abstaining from drug consumption during pregnancy (N = 345; 95.56%), while an even greater proportion (N = 352; 97.51%) reported refraining from alcoholic beverages. Furthermore, a substantial majority of participants (94.46%) reported not having smoked during their pregnancy. The same number of participants (94.46%) reported having received prenatal care. The overall mean S/D ratio of the umbilical artery was 2.44 (with a median value of 2.4). None of the baseline maternal characteristics statistically significantly differed based on placental location.
As delineated in Table 2, researchers found that a majority of participants with a posterior placental location had an artificial rupture of membranes (48.78%). Those patients with an anterior placental location tended to have a spontaneous rupture of membranes (54.49%). Irrespective of placental location, the majority of patients had a normal spontaneous vaginal delivery (anterior 69.87%, posterior 62.44%). Neither mode of delivery nor whether the membrane rupture was artificial, spontaneous, or premature showed statistical significance when compared against placental location (P = .27 and .444, respectively). The calculated mean blood loss based on placental location for women with an anterior placenta was 445.19 mL and for women with a posterior placenta, the mean blood loss was 478.93 mL (P = .25).
In terms of gestational duration, the majority of births were full term (anterior 55.78% and posterior 61.95%) and further analysis to detect an association with placental location yielded no statistically significant relationships. Statistical significance was determined regarding the 5-minute Apgar scores, which showed a mean of 8.77 in the anterior placenta group compared to a mean of 8.91 for the posterior placenta group, with a P value of .03.
Discussion
A significant body of research exists concerning associations between placental location and maternal, as well as neonatal outcomes. However, most of the prior studies included a predominantly Caucasian population. This study was unique due to its predominantly African American/Caribbean American population. 22
According to the US Department of Health & Human Services, African American women tend to have higher obesity or be considered overweight compared to other groups in the United States. 23 Based on the results of this study, the mean BMI was 31.64 for women with anterior placentas, and 32.41 for those with posterior placentas. No association was observed between BMI and placental location (P = .28).
In a prior study by Zia, a significant association was found between posterior placental location and preterm labor. 3 This was not consistent with the current research findings, as no association was demonstrated between preterm labor and placental location. This discrepancy may be attributed to the fact that only 10.5% of this study population delivered preterm. Regarding placental location and birthweight, this study’s results demonstrated a lack of statistical significance, which was consistent with the Zia study.
Previous research reported that anterior placentas showed a strong association with O+ blood type, while posterior placentas were linked to blood type A+. 3 Contrary to these previous research findings, this study did not find any association between placental location and maternal blood type. Very few, if any, additional studies have been conducted comparing these variables. Larger scale studies are needed to confirm the correlation between these two variables.
In a study conducted by Torricelli et al., 2 which evaluated 2354 women’s outcomes, those with an anterior placenta had a statistically significantly higher rate of PPH during vaginal deliveries. In contrast, Belachew et al. 19 studied 400 women with previous cesarean sections and found no statistical significance between PPH and placental location. Similarly, researchers discovered no difference between the mean blood loss of women with an anterior versus posterior placental location. This study’s findings are consistent with Belachew’s results and did not show a significant association between PPH and placental location. One explanation of the differences in these findings could be the sample size discrepancies between these studies.
Limitations
This research study had several limitations including its retrospective cohort study design, which has threats to internal and external validity. There also may be inherent variability based on the reporting styles of different sonographers when locating the placental position, the experience of the sonographers, and convenient sampling. In addition, this study was limited to one health care facility. A larger prospective study, where the placental positions are determined by only one experienced sonographer, would be useful to confirm the findings of this study. Additionally, a larger sample size and/or including data from more than one health care facility may yield stronger and more significant results.
Conclusion
In summary, this study endeavored to analyze associations, if any, between normal placental locations and its effects on maternal and neonatal outcomes. No statistical significance was observed between the placental location and the majority of variables analyzed, in this particular cohort. Statistical significance was appreciated in the 5-minute Apgar score category between anterior and posterior placentas (P = .032), showing that posterior placental locations yielded a higher score in this group.
Research including more than one health care facility with a larger sample size is recommended to further investigate the association between placental locations and maternal/fetal outcomes. These types of studies have the potential to inform more effective pregnancy monitoring and outcomes for women and their infants.
Footnotes
Acknowledgements
The authors acknowledge Drs David Sherer, Mudar Dalloul, Ehab Abdelmalek and Sarin Soyemi and their respective departments for their invaluable contributions to this study.
Ethics Approval
The hospital’s Institutional Review Board approved the study (IRB # 1468616).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research won a $5000 grant from the SDMS Foundation’s Research Grant Program.