
Abstract
Placenta previa is one of the most common complications in pregnancy. A partial or complete obstruction of the internal cervical os prevents a normal vaginal delivery. It can be further complicated by placenta accreta. Accreta, increta, and percreta are the three types of placental accreta identified and involve different layers of uterine myometrium. Of these types, percreta is the most invasive, invading through the myometrium to the uterine serosa and potentially affecting surrounding organs or tissues. The prevalence of accreta is increased with those who have a history of cesarean sections. This case study demonstrates how color and gray-scale sonography are a reliable imaging method for identifying placenta previa and accreta.
This case study presents a patient diagnosed with both placenta previa and placenta accreta using both sonography and magnetic resonance imaging. Recent studies have shown a correlation with the development of placenta accreta in patients with a previous cesarean section. 1 As the consequences of an undiagnosed previa or accreta may increase both maternal and fetal mortality, it is important that this is recognized and diagnosed early in the pregnancy. Sonography plays an essential role in diagnosing placenta previa and accreta.
Case Report
A 36-year-old pregnant woman, G4 P2012, presented with heavy vaginal bleeding at 18 weeks 5 days’ gestation. She was referred to a maternal fetal medicine clinic for a history of two prior cesarean sections. In addition, there was a suspicion for placenta increta and placenta previa based on an outside sonographic examination. An anterior previa was visualized on the sonogram with placental lakes and blurred borders as well as a distorted and questionably invaded cervix.
The initial sonogram performed at this facility was done using a Philips iU22 ultrasound system (Philips Medical, Bothell, WA) with a 5-MHz curved linear transducer. The anterior location of the placenta extended inferiorly, completely covering the internal cervical os. A loss of the myometrial/placental interface at the level of the bladder could be seen (Figure 1). Hypervascularity was also seen at the uterine-bladder interface with possible interruption of the bladder wall (Figure 2). Venous lakes were visualized throughout the placenta at the level of the lower uterine segment (Figure 3). These findings were consistent with placenta previa and concern for a possible percreta into the bladder at the level of the cesarean scar. Fetal measurements were appropriate for the gestational age, and all visualized fetal anatomy appeared normal.

Sagittal sonographic image of the cervix showing complete placenta previa. Loss of the clear zone is also seen (open arrow).
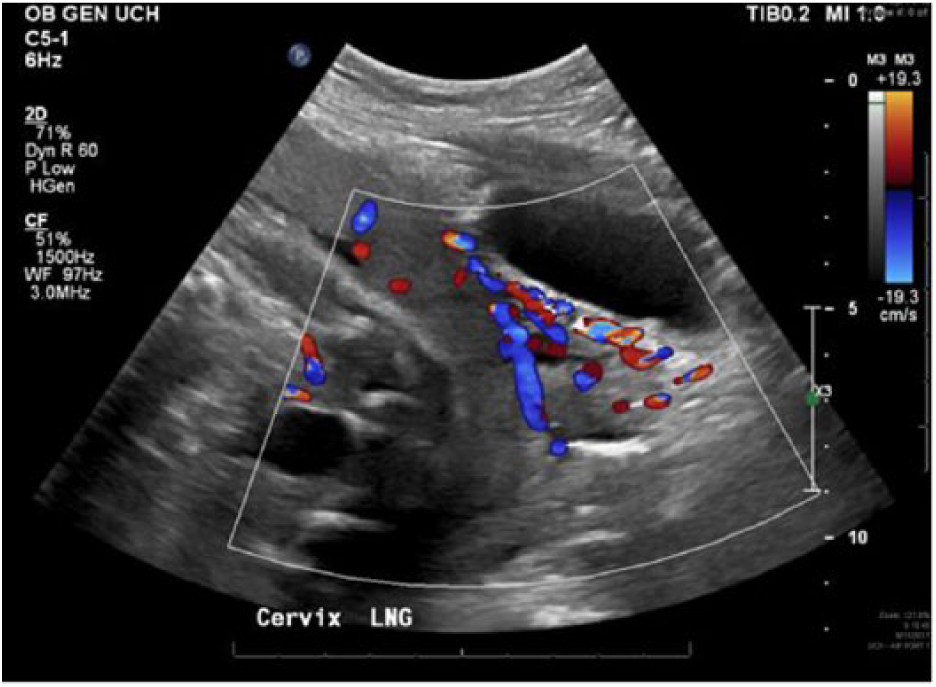
Sagittal color Doppler sonographic image of the cervix showing hypervascularity between the posterior bladder wall and the myometrium of the uterus.

Venous lakes are visualized throughout the placenta at the level of the lower uterine segment.
The patient was made aware of the risk for preterm delivery, the need for a hysterectomy, and possible bladder and bowel resection if maternal hemorrhage occurred.
The patient had a subsequent pelvic magnetic resonance imaging (MRI) examination performed without contrast at 18 weeks 6 days’ gestation. This showed a low-lying anterior placenta completely covering the internal cervical os, consistent with complete previa. Mild tenting of the superior bladder wall with disruption of adjacent fat planes suggested a possible bladder wall invasion consistent with placental percreta (Figure 4). A focal area of the lower uterine segment scarring was also visualized (Figure 5).
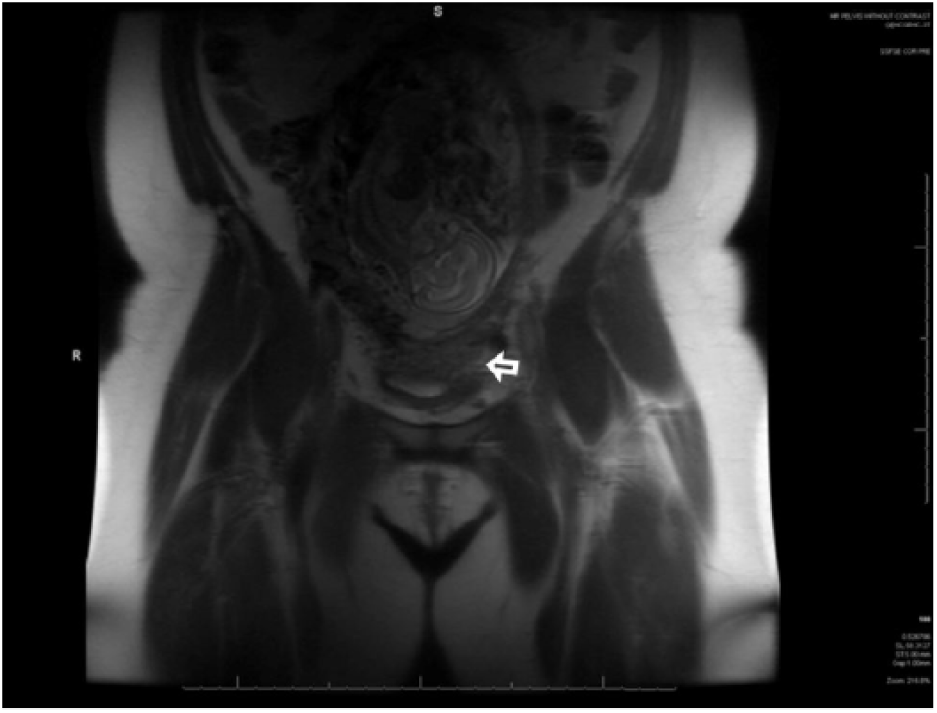
Coronal magnetic resonance image of the pelvis showing placental invasion into the bladder (open arrow).

Area of the lower anterior uterine segment with wall thickening/scarring.
At 24 weeks’ gestation, the patient was admitted to the antepartum department to be consistently monitored until delivery. She experienced frequent small-volume bleeding, which increased to 200 cc before delivery. Due to the increased bleeding, a cesarean section was performed at 31 weeks 6 days. A transabdominal vertical surgical incision, a hysterotomy, was performed at the fundus of the uterus with sonographic guidance to avoid hemorrhage complications of the placental percreta location where a normal cesarean section would occur. Once the baby was delivered, the hysterotomy was closed with the placenta left in the uterus, and the gynecologic oncology team assumed care for the remainder of the surgery. A type II radical hysterectomy was performed, which included a bilateral ureterolysis, or a dissection of the ureters up to the bladder. 2 This procedure also included ligation of the uterine arteries and resection of the uterosacral ligament. 2 The cardinal ligaments were excised, and 1 to 2 cm of the upper vagina were removed. 2 A radical placenta/tumor resection was also performed. A cystoscopy procedure was also necessary to view the integrity of the lining of the bladder wall using a cystoscope. The placental villi reached through the uterine serosa into the bladder peritoneum, although no bladder wall invasion was visualized.
Pathology confirmed placenta percreta involving the anterior aspect of the uterus. The placenta was otherwise histologically appropriate for gestational age. Fibrovascular tissue in the peritoneum and pelvic excision region included rare attached chorionic villi. The cervix also expressed reactive changes within the squamous epithelium.
Discussion
Placenta previa, a diagnosis of a partial or complete covering of the internal cervical os, affects 0.5% of live births and can lead to maternal hemorrhage and morbidity. 3 Previa is typically diagnosed during the second trimester as low-lying or incomplete, and it is more likely resolved by the third trimester. 3 A low-lying placenta is described when the leading placental edge is between 0 and 20 mm from the internal cervical os. 3 If the leading placental edge completely covers the internal cervical os, it is considered a complete previa. 3 A study performed found that 95% of diagnosed placenta previa resolved by 36 weeks’ gestation. 3 According to a previous study, the highest risk group for a cesarean delivery included women with a thick-edge low-lying placenta due to lack of placental migration. 4 An additional study found that previa was diagnosed in 10% of pregnancies in the second trimester with most resolving by 36 weeks’ gestation. 3 Most women diagnosed with low-lying placenta or complete previa will resolve prior to delivery with a median resolution time of 10 weeks from mid-trimester diagnosis during an anatomy survey. 3
Placenta accreta is most often an iatrogenic, abnormal invasion of placental tissue into the uterine musculature. 1 Placenta accreta was first acknowledged in 1937 as the failure of the placenta to separate from the uterus postdelivery followed by severe postpartum hemorrhage. 1 Depending on the depth of villous invasiveness, they are graded into placenta creta or vera, increta, and percreta. 1 The villi adhere to the myometrium of the uterus in cases of placenta creta or vera. 1 Placenta increta is described by villi penetrating deeply into the myometrium. 1 Placenta percreta is the most invasive, with the villi reaching or penetrating through the uterine serosa reaching the surrounding pelvic tissues and organs. 1 It is thought to occur due to a defect of the endometrial-myometrial interface in the area of a uterine scar, which allows trophoblastic infiltration beyond the superficial myometrium as well as villous development inside the myometrium. 1 Placenta accreta has been associated with uterine anomalies such as bicornuate uterus, adenomyosis, submucousal fibroids, and myotonic dystrophy. 1 However, it is more common to find intramyometrial implantation of villous tissue secondary to uterine surgery such as cesarean section. 1
It has been shown that there is an increased likelihood of placenta previa with an increased number of previous cesarean section deliveries. 5 In addition, the risk for placenta previa increased with a greater parity independent of the number of cesarean section deliveries. 5 The risks of having both placenta previa and accreta also increased with the number of cesarean section deliveries, but each can occur independently from one another. 5 In one study, around 75% of women diagnosed with placenta accreta planned for a peripartum hysterectomy. 1 However, hysterectomy is not always required if management for bleeding is controlled. 1
An evaluation to determine the depth of placental accreta invasion is crucial for delivery and postpartum care of the patient. 1 Using gray-scale sonography imaging, signs of placenta accreta include a loss of the clear zone.1,6 The clear zone is a normal, retroplacental, sonolucent zone associated with dilated vessels of the decidua basalis. 7 Loss of the clear zone indicates loss of the decidua. 7 Myometrial thinning to <1 mm or undetectable can also be seen. 1 A “moth-eaten” appearance of the placenta represents intraplacental lacunae or lakes, often large and irregular, and can be associated with accreta.1,6 If the accreta has progressed into percreta, the bladder wall may be interrupted or not visualized. 1,6 This should normally appear as a hyperechoic line between the uterine serosa and bladder lumen.1,6 Sometimes a placental bulge may be seen distorting the extrauterine organs. A focal exophytic mass of placental tissue, extending beyond the serosa, may also be seen. 1
Color Doppler has been suggested to aid in the diagnosis of placenta previa and accreta because of its sensitivity in detecting hypervascularity and can be made with a high level of confidence. 6 Sonographic signs of increta or percreta include uterovesical hypervascularity linking the myometrium and the posterior wall of the bladder, as well as a hypervascular dilated peripheral subplacental or placental bed.1,6 With percreta, color Doppler may show bridging vessels across the myometrium and beyond the serosa. 1 Diffuse lacunae feeder vessels with high-velocity or turbulent flow from the arterial vasculature of the myometrium can also be seen.1,6
The most common sonographic signs of accreta include a loss of the clear zone and placental lacunae present in gray-scale imaging and subplacental hypervascularity and bridging vessels on color Doppler imaging. 1 However, none of these signs, or a combination of these signs, is specific for determining the depth of invasiveness, making it difficult to categorize the level of accreta by sonography. 1
In a study done to evaluate the efficacy of color Doppler used as a means to accurately diagnose placenta previa and/or accreta, all of the abnormally adherent placentas were correctly identified for previa, but two with accreta were misdiagnosed. 6 One was a posterior accreta and the other was a lateral accreta. 6 The patients with proven placenta increta exhibited diffuse hypervascular placental lacunar flow as well as the surrounding myometrial tissues or vascularity within the serosa-bladder junction. 6
There is, however, the possibility of false-positive results using sonography as a tool for diagnosing placenta previa or placenta accreta. With color Doppler, bladder varices could be mistaken for an interphase hypervascularity. 6 A previous study performed found the sensitivity of transabdominal color Doppler for true positives was 82.4%, and the specificity for true negatives was 96.8%. 5 Other studies have shown higher sensitivities, as much as 100%. 6
Due to the adherence of the placenta into the uterine myometrium in the case of placenta increta or percreta, an increased risk for hemorrhage is likely, and a blood transfusion may be necessary during delivery. 7 Interventions such as hysterectomy, ureteric stenting, and cystotomy are likely surgical possibilities, or a conservative approach, such as leaving the placenta in situ, use of cell salvage, and interventional radiology, is another possible intervention. 7 These options should all be discussed with the patient prior to delivery.
Conclusion
Many advances have been made to help identify and diagnose placenta previa and/or accreta. Several sonographic signs have been identified to help aid in the treatment of a patient with these findings during pregnancy. Gray-scale sonography and color Doppler currently continue to be safe and effective imaging modalities for monitoring the progression of accreta as well as changes with placenta previa throughout pregnancy.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.