
Abstract
Placenta percreta is the most complicated degree of the placenta accreta spectrum (PAS). It involves placental invasion through the uterine myometrium and into, or beyond, the uterine serosa, which can ultimately lead to severe maternal hemorrhage. Placenta previa is often associated with PAS and can be a significant indicator, along with other clinical factors. Sonography has historically been a highly accurate and safe imaging modality to assess the PAS. This specific case examines a patient with a pathologically proven percreta with an associated previa and succenturiate placental lobe.
Placenta percreta is the most severe form of placenta accreta spectrum (PAS). It involves trophoblastic placental tissue invading through the uterine serosa and possibly to other pelvic organs. 1 The incidence of PAS has risen from 1 in 2500 pregnancies to 1 in 500 pregnancies, primarily due to the increase of cesarean section rates. 1 It is critical to identify PAS prior to delivery due to an increased risk of maternal hemorrhage and mortality at delivery. 1 Sonography in conjunction with magnetic resonance imaging (MRI) can be highly accurate in evaluating for PAS, prior to delivery. 2 The following case presents a patient with both a complete placenta previa, a pathologically proven placenta percreta, and an associated succenturiate placental lobe. This case discusses the use of a high-frequency linear transducer which was used to aid in the sonographic diagnosis.
Case Report
A 40-year-old G4P3003 pregnant female was referred to a medical center, to further assess and plan for delivery for a suspected placenta previa and accreta, both of which had been seen on a prior sonogram from an outside imaging center. This patient was of advanced maternal age (AMA) with a history of three prior cesarean section deliveries.
Due to the outside imaging findings and patient history, an MRI examination was performed at the medical center, during the 30 weeks and 1-day gestation. This imaging study demonstrated a bulging of placental tissue noted midline over the posterior aspect of the bladder roof. This placental tissue was also noted at the right lower quadrant (7 and 8 o’clock positions) with notable thinning and possible disruption of the uterine serosa (see Figure 1). The MRI findings were consistent with a complete placenta previa as well as concern for PAS, and more specifically, a placenta percreta.
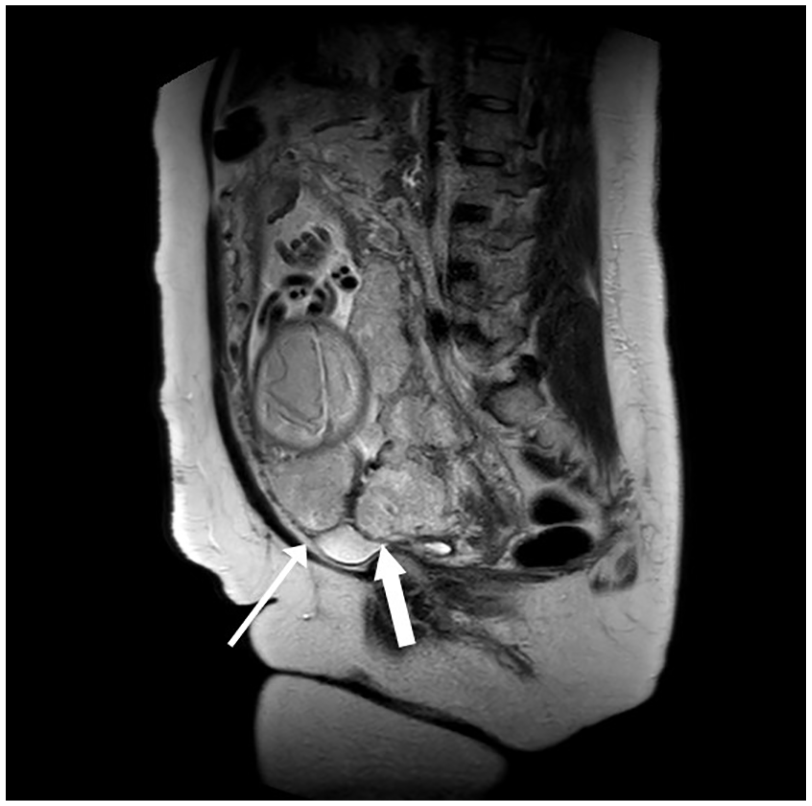
Sagittal MRI image exhibiting bulging of placental tissue midline over the posterior aspect of the bladder roof (thick white arrow) as well as at the right lower quadrant (thin white arrow). MRI, magnetic resonance imaging.
The patient was admitted at 33 weeks and 6 days of gestation to the labor and delivery unit at the medical center, for monitoring due to vaginal bleeding. A sonographic examination was performed transabdominally using a Philips Epic Logic 7 ultrasound system (Philips Medical, Bothell, WA) with both a C 5-1 MHz curved array transducer and an L 12-3 MHz linear-array transducer. Utilizing the C 5-1 MHz transducer, the placenta was visualized completely covering the internal os of the cervix and extending anteriorly to the midpoint of the maternal bladder (see Figure 2A). At this level, a significant amount of vascularity was visualized between the placenta and the maternal bladder in addition to numerous placental lakes with turbulent flow (see Figure 2B). A notable succenturiate placental lobe was also visualized anterior and to the right of the primary placenta where there was loss of the uteroplacental border (see Figure 2C). These areas were further assessed utilizing a linear-array transducer (L12-3 MHz transducer) to obtain better resolution of the uteroplacental border. At the level between the midline placenta and the maternal bladder, a distinct disruption of the uterine serosa by the placenta was visualized. This was also noted in gray-scale sonographic imaging as well as increased vascularity with color Doppler (see Figures 3A and 3B). At the level of the succenturiate lobe, a loss of the uteroplacental border was seen again with gray-scale imaging as well as the increased vascularity with color Doppler (see Figure 3C). These diagnostic findings were indicative of a complete placenta previa. These results also raised the suspicion for placenta percreta by both the primary and succenturiate placental lobes, at the level of previously incised cesarean section scars.
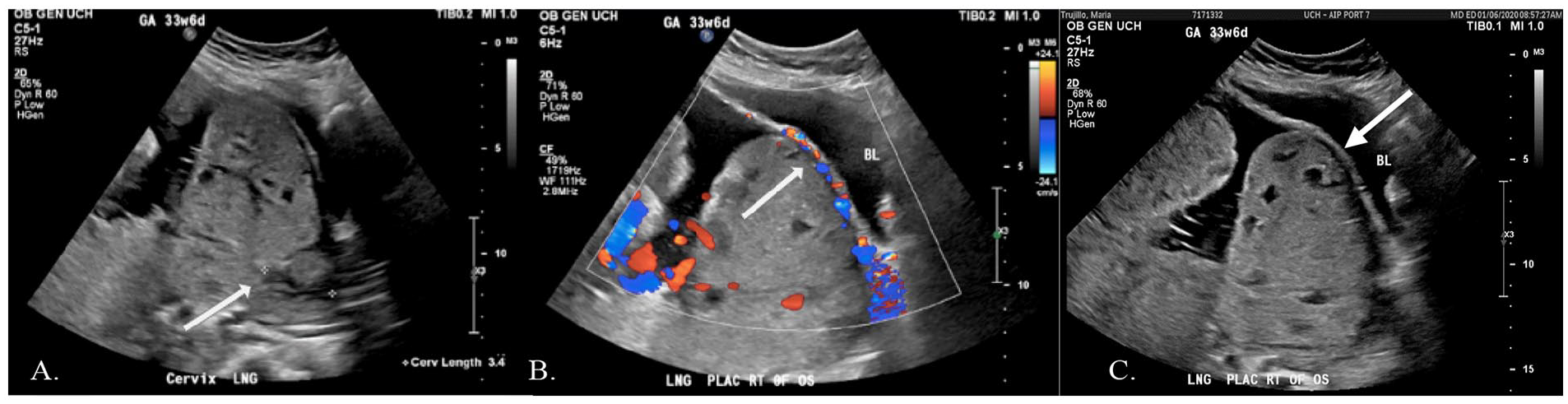
(A) Longitudinal sonographic image of the cervix (using C 5-1 MHz transducer) depicting a complete placenta previa over the level of the internal os (white arrow), in addition to numerous placental lakes with turbulent flow and (B) Longitudinal sonographic image of the placenta (using C 5-1 MHz transducer) exhibiting hypervascularity between the anterior aspect of the placenta and bladder wall (white arrow). (C) Longitudinal sonographic image of the succenturiate lobe (using C 5-1 MHz transducer) showing loss of the uteroplacental border on gray scale (white arrow).
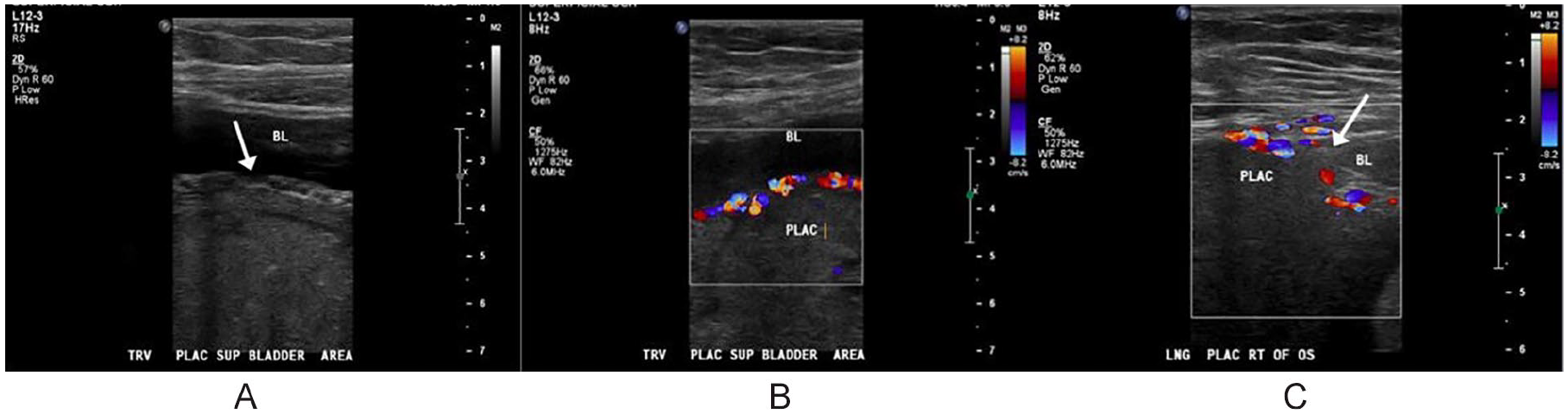
(A) Transverse sonographic image of the placenta at the level of the maternal bladder (using L 12-3 MHz transducer) indicating disruption of the uterine serosa (white arrow), (B) Transverse sonographic image of the placenta at the level of the maternal bladder (using L 12-3 MHz transducer) portraying hypervascularity within the bladder wall, and (C) Longitudinal sonographic image of the succenturiate placental lobe at the level of the maternal bladder (using L 12-3 MHz transducer) showing loss of the uteroplacental border on gray-scale (white arrow) and hypervascularity on color Doppler.
After meeting with both the maternal fetal medicine (MFM) and gynecology oncology teams, the patient consented to a planned preterm cesarean hysterectomy at 34 weeks gestation. This decision was made due to her excessive vaginal bleeding and the extensive degree of percreta. The patient was taken to surgery by the MFM team where intraoperative ultrasound was utilized to map the placenta, in the lower uterine. To not disrupt the placental invasion at the lower uterine segment, a traditional cesarean section could not be performed. Instead, a classical incision at the level of the fundus was created and the live born male fetus was delivered breech, regardless of his cephalic presentation. Areas concerning for placenta percreta were noted in the right lower uterine segment between the uterus and the maternal bladder (see Figure 4). The MFM team then closed the hysterotomy with the placenta still intact for the gynecology oncology team to assume care, for the hysterectomy. Attention was first given to the anterior vesicouterine peritoneum where the team spent approximately 2 hours dissecting this from the lower uterine segment. It was noted that there was clear placenta invading into the dome of the bladder. A significant amount of bleeding (3000 milliliters) was encountered during this and control of intraoperative hemorrhage ensued. The team then continued with a type 2 radical hysterectomy, which included bilateral ureterolysis (intentional freeing of the ureters to prevent them from injury during surgery). It also necessitated the repair of intentional cystotomy (a cystotomy was performed to monitor the integrity of the bladder during surgery and to prevent future complications) and a bilateral salpingectomy. Operative findings were consistent with placenta percreta invading into the posterior wall of the bladder, at the level of the dome. The patient tolerated the surgery well and was sent to recovery with a foley catheter in place and minimal damage to the bladder and ureters.
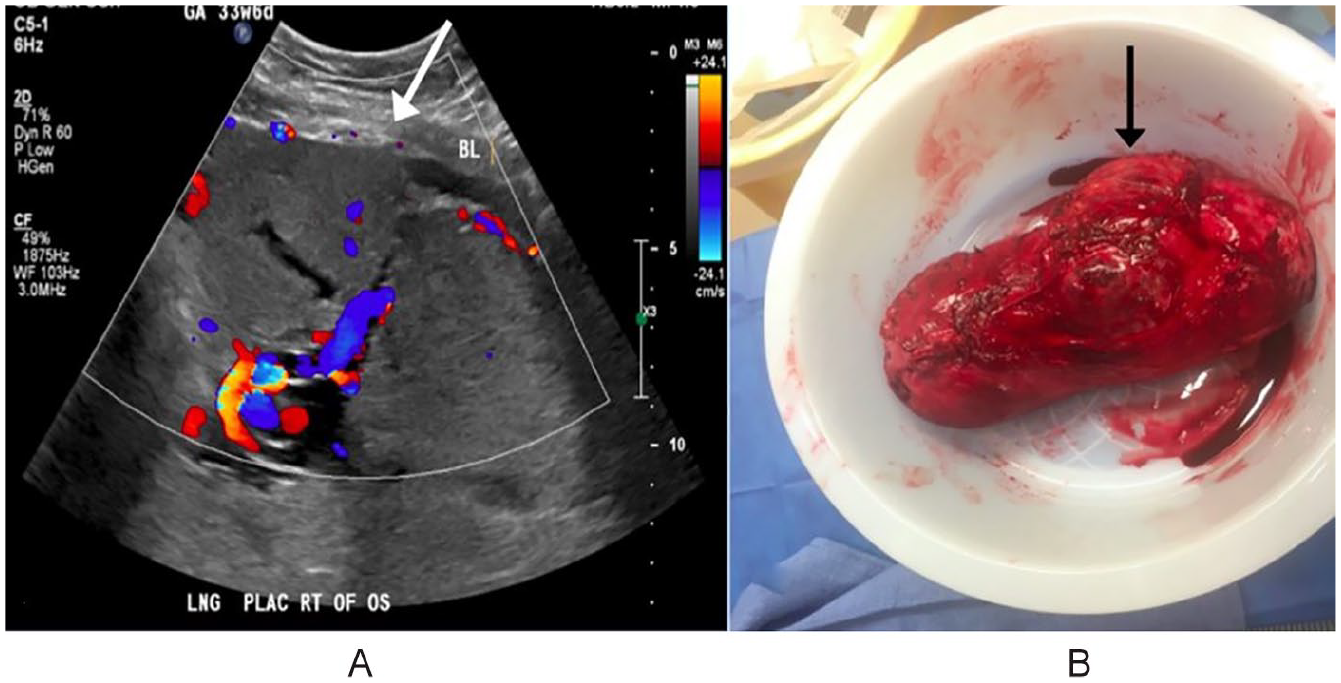
(A) Longitudinal sonographic image of the succenturiate placental lobe (using C 5-1 MHz transducer) portraying loss of the uteroplacental border at the lower uterine segment (white arrow). This area corresponds to the gross specimen in Figure 4B and (B) Post-operative specimen of the uterus with a notable bulging of placental tissue, through the lower uterine segment of the uterus (black arrow).
Both uterus and placenta were sent to pathology following hysterectomy with pathologic findings of placenta percreta et previa with implantation site trophoblasts extending into adherent adipose tissue. A high-grade chorionic villitis was also pathologically reported.
Discussion
PAS as a broad term is the abnormal invasion of trophoblastic placental tissue beyond the endometrium. 1 There are varying degrees of PAS including accreta, increta, and percreta depending on how far the placenta extends beyond the endometrium.1,3 The least severe of the three is accreta, in which the placenta extends into less than 50% of the uterine myometrium. 1 The second type is increta, which occurs when the placenta extends into greater than 50% of the uterine myometrium. 1 The third and most severe type is percreta and is characterized by placental tissue that extends completely through the uterine myometrium and into the uterine serosa. It has the potential of invading surrounding structures and organs such as the maternal bladder. 1 The incidence of PAS has risen from 1 in 2500 pregnancies to 1 in 500 pregnancies which is thought to primarily be due to the increase of cesarean section rates. 1 The pathophysiology of PAS is not known with 100% confidence; however, there are several theories as to why PAS occurs. 1 The primary theory being that prior uterine scarring from surgeries such as cesarean section, myomectomy, uterine curettage, and ablation allows for abnormal invasion of placental tissue through a uterine defect.1,4 Another theory is thought to be a result of the existing hypoxic environment post uterine surgery/procedure that could potentially act as a catalyst for trophoblastic invasion through the endometrial defect. 1 Other risk factors of PAS include AMA, smoking, placenta previa, multiparity, advanced reproductive techniques (ART), submucosal fibroids, and infectious processes such as endometritis. 1
The clinical significance of PAS is the high risk of both maternal and fetal morbidity and mortality. 5 The risk of fetal morbidity and mortality can be attributed to the iatrogenic preterm delivery of the fetus. 3 Maternal morbidity and mortality is predominantly related to the increased risk of postpartum hemorrhage.5,6 Ninety percent of mothers affected by PAS require a blood transfusion during surgery to recover the average of 3000 to 5000 milliliters 3 of blood loss.1,6 Other common surgical complications may include radical hysterectomy, and/or damage to surrounding organs such as the maternal bladder, ureters, bowel, and rectum. 1 These complications could prolong hospitalization, increase medical bills, and has been shown to increase the incidence of maternal psychological distress such as post-traumatic stress disorder. 1 The treatment for PAS, similar to that for placenta previa, includes the patient to be counseled for a planned cesarean section since PAS also puts the patient at an increased risk of hemorrhage. 1 PAS also typically requires both a delivery team and surgical gynecologic team to be present at delivery in anticipation of postpartum hemorrhage. 1 Once the baby has been delivered, the gynecologic surgical team will perform the hysterectomy if necessary and/or spend time resolving the placental invasion depending on its severity. 1 Official diagnosis of PAS is then made histopathologically. 1
Placenta previa is abnormally located placenta at the level of, or near, the internal cervical os due to lack of placental migration. 7 The most common location of a placenta in a pregnancy, not complicated by previa, is anterior. 8 Other normal locations of the placenta include posterior, lateral, or fundal. There are varying degrees of placenta previa including “total,” “partial,” and “marginal.” 7 A total previa describes the placenta completely covering the internal cervical os whereas partial and marginal previas describe the placenta either partially covering or lying just next to the internal cervical os, respectively. 7 The placenta can also be considered “low-lying’’ meaning that the placental edge is within 2 centimeters of the internal cervical os. 7 However, it is not likely that early visualization of a low-lying placenta or what appears to be a previa will actually result in a previa past 36 weeks. 7 The majority (91.9%) of women diagnosed with a low-lying placenta or placenta previa at their mid-trimester anatomy scan had resolution by their next follow-up scan. 7 Most resolved in 10 weeks after initial diagnosis, and those with a distance of 10 mm or greater from the internal cervical os had an almost 100% success rate of resolution at follow-up. 7 Complete placenta previa is highly associated with both AMA and prior history of cesarean section(s).3,6 Complete placenta previa increases the risk of maternal hemorrhage by fourfold, which is why vaginal birth is not recommended and patients diagnosed with placenta previa are typically counseled to have a cesarean section so that the team can prepare for potential hemorrhage to improve both fetal and maternal outcomes. 1
Placenta previa has a high association with PAS (80%) and is the strongest risk factor for PAS especially in combination with a history of cesarean section.6,9 With a history of multiple cesarean sections and the presence of a previa, the risk of an accreta increases by roughly 8% from the first to the second cesarean section and by roughly 36.7% from the first to the third cesarean section. 6 With a history of five cesarean sections and the presence of a previa, the risk of an accreta increases to an overall incidence of 67% and remains about the same after this point independent of a history of greater than five cesarean sections. 6
A succenturiate placental lobe is not necessarily associated with PAS or placenta previa, but there have been studies reporting the association between succenturiate placental lobes and AMA. 10 A succenturiate lobe is a secondary placental lobe that is connected to the primary placental lobe by blood vessels and not by continuation of placental tissue. 10 The primary placental lobe will typically give rise to the umbilical cord rather than the succenturiate lobe; however, it is possible for the placental cord insertion to be located at the succenturiate lobe. 10 If the cord insertion is derived from the succenturiate lobe, there could be risk of intrauterine growth restriction (IUGR) for the fetus because the succenturiate placental lobe is typically smaller in size than the primary placental lobe. 10 It is also important to note that a uterine contraction can mimic a succenturiate lobe. Careful interrogation should be given to a suspected uterine contraction at both the start and end of a sonographic examination to ensure that it resolves and is not in fact a succenturaite lobe, especially if the cord is inserting into or near this area.
There are several sonographic findings that could indicate the presence of PAS. This may include loss of the retro-placental space, which refers to the myometrium that is normally seen between the placenta and serosa of the uterus.11,12 Other sonographic findings may include thinning of the myometrium, placental lakes (lacunae), increased peripheral vascularity with color Doppler, placenta previa, and an irregular bladder wall (if suspecting percreta).11,12 The presence of these sonographic findings, any or all, is not always indicative of PAS and is not 100% accurate for diagnosing the level of accreta, if any. 5
While sonography and MRI are typically used in conjunction with one another to aid in the diagnosis of PAS, neither one of these modalities can definitively diagnose PAS until it has been pathologically proven at delivery.2,12 In most cases, the clinical suspicion of PAS would have to be high to visualize PAS findings on either modality; especially since MRIs are not routinely ordered on most pregnant patients.2,11 Due to these limitations, sonography has often been the preferred modality when initially evaluating for PAS. 11 Sonography in comparison with MRI is more readily available, more efficient, and less expensive.2,11 In a recent study, the isolated use of sonography was found to be more accurate in the diagnosis of PAS with a higher sensitivity (95.65%), specificity (91.78%), and positive predictive value (88%) than that of an isolated MRI. 11 However, MRI is still frequently used as an adjunct to sonographic findings of possible PAS, to further characterize the degree of pathology. 11 While sonography is often the preferred single imaging modality for evaluating for PAS, the accuracy for diagnosing it remains higher when both sonography and MRI are conducted together (97.5%).2,13
It is important to note that sonography has technical limitations and user dependency leading to inaccuracies of diagnosing PAS. 2 It has been shown that second trimester sonographic findings associated with the misdiagnosis of PAS included abdominal fat, bladder fullness, and placental location. 2 Third trimester sonographic findings that were highly associated with the misdiagnoses of PAS included dense placental blood vessels that were mistaken for hypervascularity. 2
Generally, lower frequency transducers (such as the C 5-1 MHz curvilinear transducer) are traditionally used for the sonographic imaging of deep structures, given this promotes deeper penetration but decreased resolution. 13 Linear transducers, however, are best used for imaging superficial structures given that resolution will be enhanced but that depth will be compromised. 13 Obstetric sonography typically utilizes lower frequency transducers due to the deep location of the fetus. 14 However, higher frequency transducers can be utilized in obstetric sonography for imaging superficial structures, like an anteriorly positioned placenta. Increased resolution allows for a more detailed evaluation of the surface of the placenta, cesarean scar site, and the maternal bladder; all important structures to identify when evaluating for percreta. 14 Endovaginal transducers also utilize higher frequencies and have been proven to aid in the diagnosis of PAS. 15 According to a prior study, 5 out of 21 patients with persistent previas demonstrated early sonographic signs of PAS. 15 Of these five suspected PAS patients, all five were pathologically proven to have some form of PAS at delivery. 15 An additional study showed both low- and high-frequency transducers were effective to examine the degree of suspected PAS in multiple patients. 14 It was found that higher frequency imaging allowed for better resolution of the uterine defect both on gray-scale imaging and color Doppler. 14 The high-frequency transducer was able to add information to the examination that the low-frequency transducer could not. 14 The higher frequency transducer revealed additional vascularity on color Doppler within the bladder wall compared with the lower frequency transducer, which is suggestive of placental bladder invasion. The lower frequency transducer revealed only vague peripheral vascularity between the placenta and maternal bladder. 14
Conclusion
Placenta percreta can be a serious complication of pregnancy due to maternal hemorrhage, which is why it is essential to evaluate for PAS when there is a high clinical indication. The presence of placenta previa in conjunction with a history of cesarean section(s) is the strongest risk factor for PAS and should warrant careful sonographic examination. Although there is no direct association between a succenturiate placental lobe and PAS or previa, it is important to note the presence of a succenturiate lobe. This case study demonstrated that this portion of the placenta had invaded the uterus. Sonography is a highly accurate and safe imaging modality for detecting PAS prior to delivery. This case also highlighted how additional diagnostic information can be added, with the use of high-frequency linear transducers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.