
Abstract
Objective:
This study aimed to explore the effects of age, sex, body mass index (BMI), and smoking on the diameter of the portal vein (PV).
Materials and Methods:
This quantitative descriptive study included 113 participants (61.9% males and 38.1% females) who underwent sonography. The participants were selected via convenience sampling. Patients with known cardiac, liver, or biliary diseases were excluded. The PV of each participant was evaluated and measured using a 3.5 MHz transducer and a standard liver sonography imaging protocol. Statistical analyses were performed using descriptive statistics, chi-square test, independent t-test, and Pearson correlations. Statistical significance was set at P < .05.
Results:
The mean age of the participants was 38 ± 16 years (range = 15–86 years). The mean PV diameter and BMI were 9.6 ± 2 mm (range = 4.9–16 mm) and 26.22 ± 8.5 (range = 15.2–39.7), respectively. The mean PV diameter of the participants who did and did not smoke was 10.5 ± 2.3 mm and 9.25 ± 1.8 mm, respectively. The PV diameter showed statistically significant associations with smoking status, age, and BMI (P = .01, .007, and .022, respectively).
Conclusion:
The findings of this study suggest that the PV diameter may increase with smoking, age, and BMI; however, no correlation was observed between the PV diameter and sex.
The portal vein (PV) and hepatic artery provide blood supply to the liver, and approximately 75% of the hepatic blood supply is derived from the PV. Portal vein is formed at the junction of the superior mesenteric vein with the splenic vein behind the neck of the pancreas at the level of the second lumbar vertebra. 1 The maximum diagnostic upper limit for the diameter of the PV is 13 mm.2,3 Geleto et al. 4 proposed that the average PV diameter and the normal pressure range from 7 to 15 mm and 5 to 10 mmHg, respectively.
Occlusion of the extrahepatic portal and splenic veins can cause complications related to portal hypertension. 5 Smoking is a risk factor for nonalcoholic fatty liver disease, which is one of the causes of hypertension.6,7 Smoking is a major public health concern that affects the hemodynamics of blood circulation. 8 Few studies have evaluated the effect of smoking on the diameter of the PV. Ahmed et al. 9 reported that smoking can cause dilatation of PV in patients with chronic liver disease. Chand and Jaradi 10 reported that the PV diameter shows significant correlations with age, height, and weight in children. Aqeel et al. 11 reported that the PV diameter shows direct correlations with weight and body mass index (BMI) in female participants; however, none of the body factors showed any correlations with the PV diameter in the male participants.
Sonography is a noninvasive, nonionizing, and accessible diagnostic tool that has been used for the detection and monitoring of patients with numerous clinical conditions, such as portal hypertension. 12 Sonography is an invaluable diagnostic tool that has been used to identify portal hypertension-related conditions, such as liver cirrhosis, ascites, splenomegaly, and dilation of the portal or hepatic veins. 13
Portal vein is the main channel of portal circulation, and its dilatation may result in portal hypertension. Therefore, this study aimed to determine whether increased PV diameter shows an association with the independent variables of smoking, age, sex, and BMI. The PV diameters of patients who did and did not smoke obtained via sonography were compared. Moreover, the study findings were correlated with the findings of previous studies, especially those pertaining to smoking, as only a few studies have been published on this issue. The primary objective of this study was to determine which of the following variables affect and increase the PV diameter: smoking, age, sex, and BMI.
Materials and Methods
This cross-sectional, descriptive study was conducted in Madinah, Saudi Arabia (KSA). This study was approved by the Research and Ethics Committee of the College of Applied Medical Sciences, Taibah University, KSA. The study data were anonymized to ensure confidentiality of the information provided by the participants.
Data were collected from 113 participants (age range = 15–86 years) who underwent PV diameter measurement using sonography at the Taibah University sonography training lab and the secondary care unit (Department of Radiology) in Hospital B between December 2022 and February 2023. Sonography was performed using MyLab40 (Esaote, Genova, Italy) and Affiniti 70 (Philips Medical, Andover, MA, USA) ultrasound equipment systems and 3.5 MHz transducers.
The participants were selected via convenience sampling. Asymptomatic students and patients with abdominal pain were included in this study. The patients had been referred to Hospital B for abdominal sonography as part of their secondary care. The exclusion criteria were as follows: patients with known cardiac disease and participants with sonographic findings of hepatomegaly, splenomegaly, hepatobiliary diseases, and dilated hepatic or splenic veins.
A structured data sheet was used to record the study data and variables such as sex, age, smoking status and duration, weight, height, and PV diameter. The BMI was calculated using the following formula: BMI = weight (kg)/height (m2).
The participants underwent sonographic examination in the supine or decubitus position. A 3.5 MHz curvilinear transducer was used to examine the liver. An acoustic couplant was applied over the right upper quadrant of the abdomen, and the transducer was placed in the transverse and longitudinal scanning planes to evaluate the main branch of the PV during quiet respiration. The PV diameter was measured from the inner-to-inner wall of the vessel (excluding the wall thickness) on high-quality images. The measurement site was the area before the bifurcation of the main PV, located within the right lobe of the liver (Figure 1). The normal upper limit of the PV diameter was 13 mm. The measurements were acquired in accordance with other published evidence in the literature.2,3

The method used to measure the diameter of the portal vein branch on the sonographic view of the liver. Note the use of electronic calipers to measure the distance between the inner-to-inner wall of the vessel.
An expert radiologist and a sonologist with more than 5 years of experience performed the sonographic examinations.
Statistical Analysis
Data were analyzed using Microsoft Excel (2021) and the Statistical Package for the Social Sciences (SPSS) program Version 26 (IBM, Armonk, New York, USA). A normality test was used to ensure the normal distribution of the study data, and the histogram indicated a normal distribution. Categorical and continuous variables are presented as percentages, frequencies, and descriptive statistics. The chi-square test was used to investigate the association between the PV diameter and sex. A set of Pearson’s correlations was used to determine the association between the PV diameter and age, as well as to investigate the association between the PV diameter and BMI. An independent t-test was used to determine the statistical association between PV diameter and smoking status. Statistical significance was set at P < .05.
Results
The study cohort comprised 113 participants with a mean age of 38 ± 16 years (range = 15–86 years). The mean PV diameter and BMI were 9.6 ± 2 mm (range = 4.9–16 mm) and 26.22 ± 8.5 (range = 15.2–39.7), respectively (Table 1). The majority of the study participants were males (61.9%).
Descriptive Statistics Based on Age, PV diameter, and BMI (N = 113).
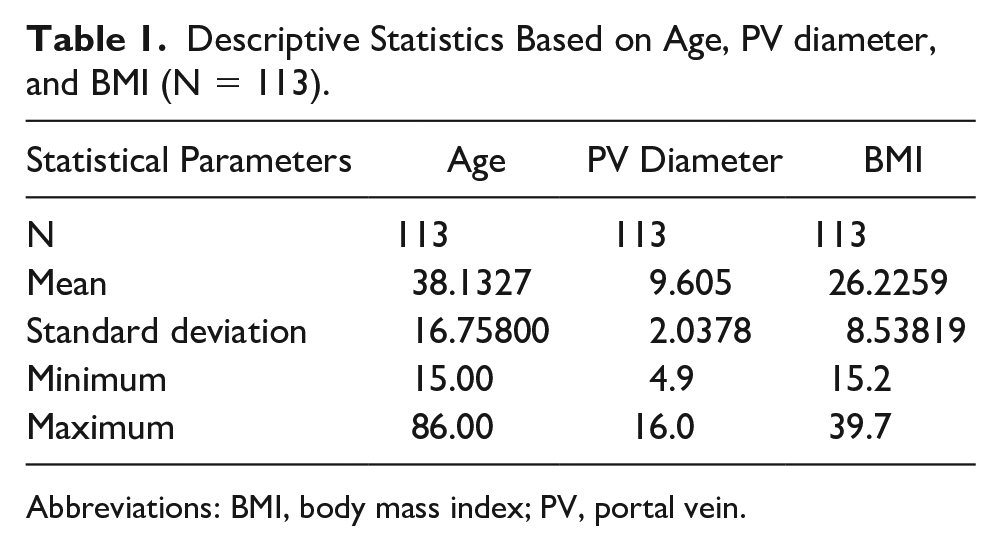
Abbreviations: BMI, body mass index; PV, portal vein.
Table 2 summarizes the results of the comparison between the participants who did and did not smoke in terms of mean age, portal vein (PV), and BMI. The proportion of participants who did and did not smoke was 27.4% (out of 113) and 72.6%, respectively. The mean age of the participants who did and did not smoke was 35 ± 14 years and 39 ± 17 years, respectively. The mean PV diameter of the participants who smoked was 10.5 ± 2.3 mm, which is higher than the mean PV diameter of the participants who did not smoke (9.25 ± 1.8 mm). The mean BMI of the participants who did and did not smoke was 24.2 ± 5.9 and 26.98 ± 9.25, respectively.
Descriptive Statistics and Comparison Between Patients Who Did and Did not Smoke (N = 113).
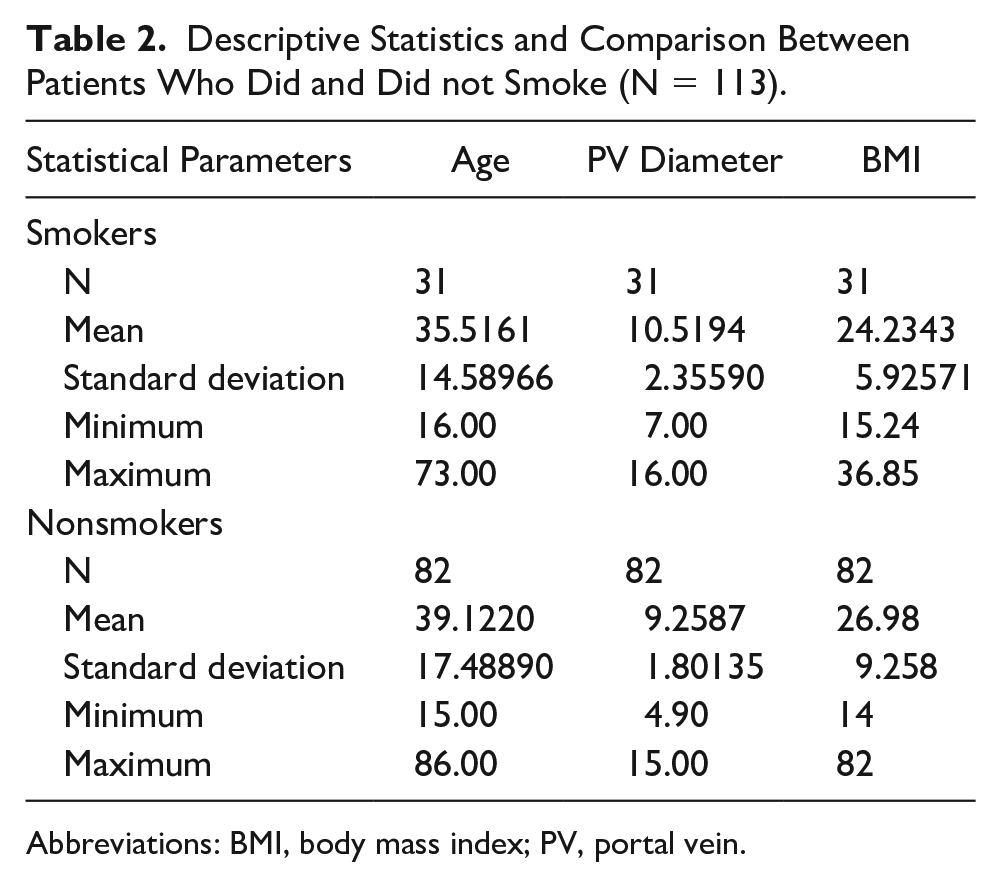
Abbreviations: BMI, body mass index; PV, portal vein.
Table 3 and Figure 2 present the statistical association between smoking status and the increase in PV diameter. Table 3 summarizes the results of the independent t-test. The mean PV diameter of the participants who smoked was higher than that of those who did not (t = 2.696, P = .01). The boxplot in Figure 2 confirms that the PV diameter of participants who smoked was higher than that of patients who did not.
Results of the Independent t-Test for a Statistical Association Between Smoking and the Portal Vein (PV) Diameter.

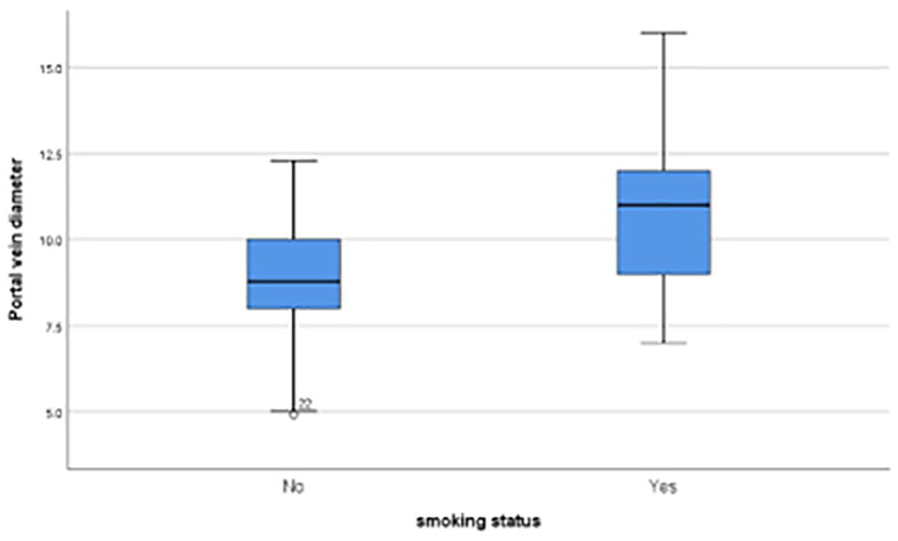
Boxplot displaying the participants’ data on smoking and the diameter of the portal vein.
Table 4 presents the results of the statistical analysis of the association between the PV diameter and age. A significant correlation was observed between the PV diameter and age (P = .01).
Statistical Correlation Between the PV Diameter and Age.
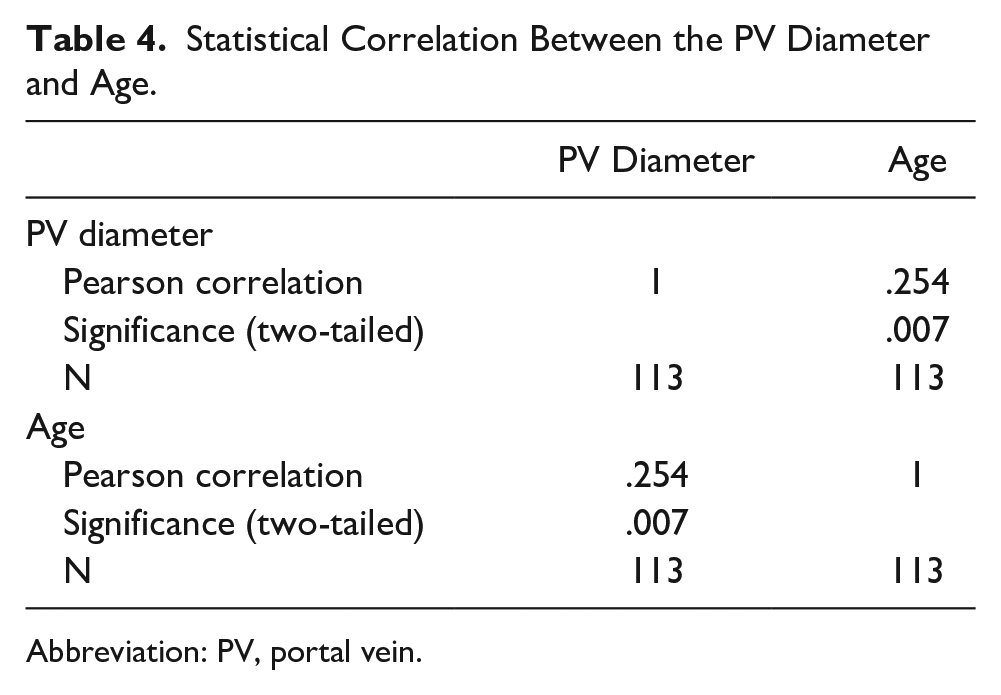
Abbreviation: PV, portal vein.
Table 5 summarizes the results of the statistical analysis of the association between the PV diameter and BMI. A significant positive correlation was observed between the PV diameter and BMI (Pearson correlation = 1.0, P =.02).
Statistical Correlation Between the PV Diameter and BMI.
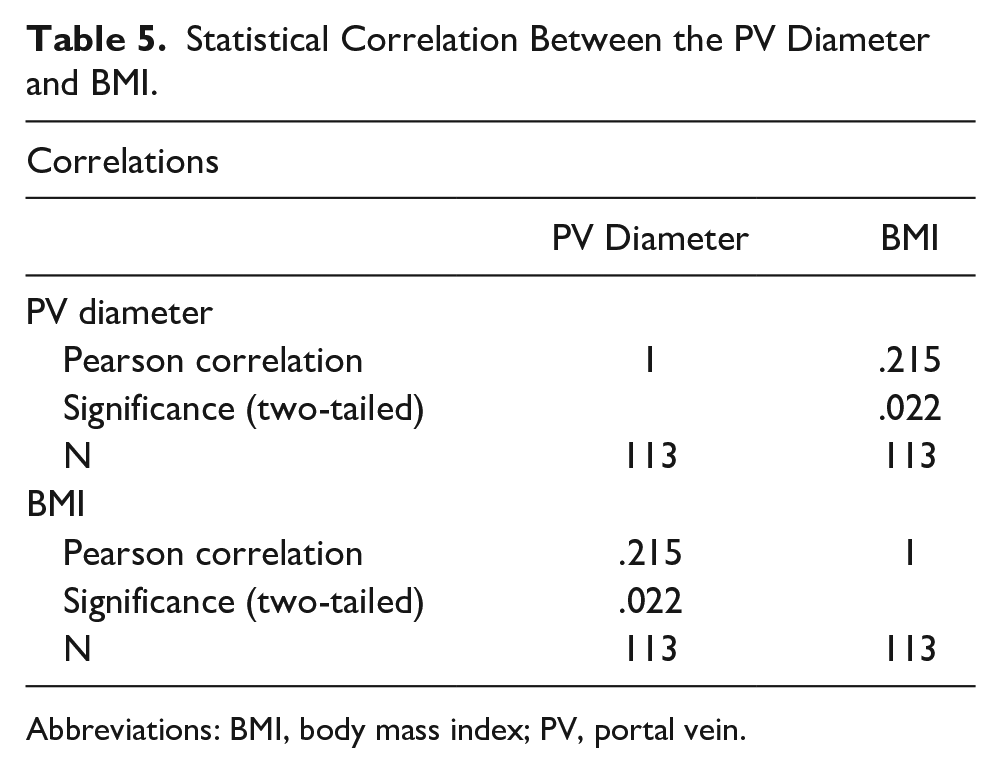
Abbreviations: BMI, body mass index; PV, portal vein.
Table 6 and Figure 3 present the results of the statistical analysis of the association between PV diameter and duration of smoking. A statistically significant correlation was observed (Pearson = 1.0, P < .05). However, the scatter plot in Figure 3 indicates a weak positive statistical association between the PV diameter and duration of smoking.
Statistical Correlation Between the PV Diameter and Duration of Smoking.
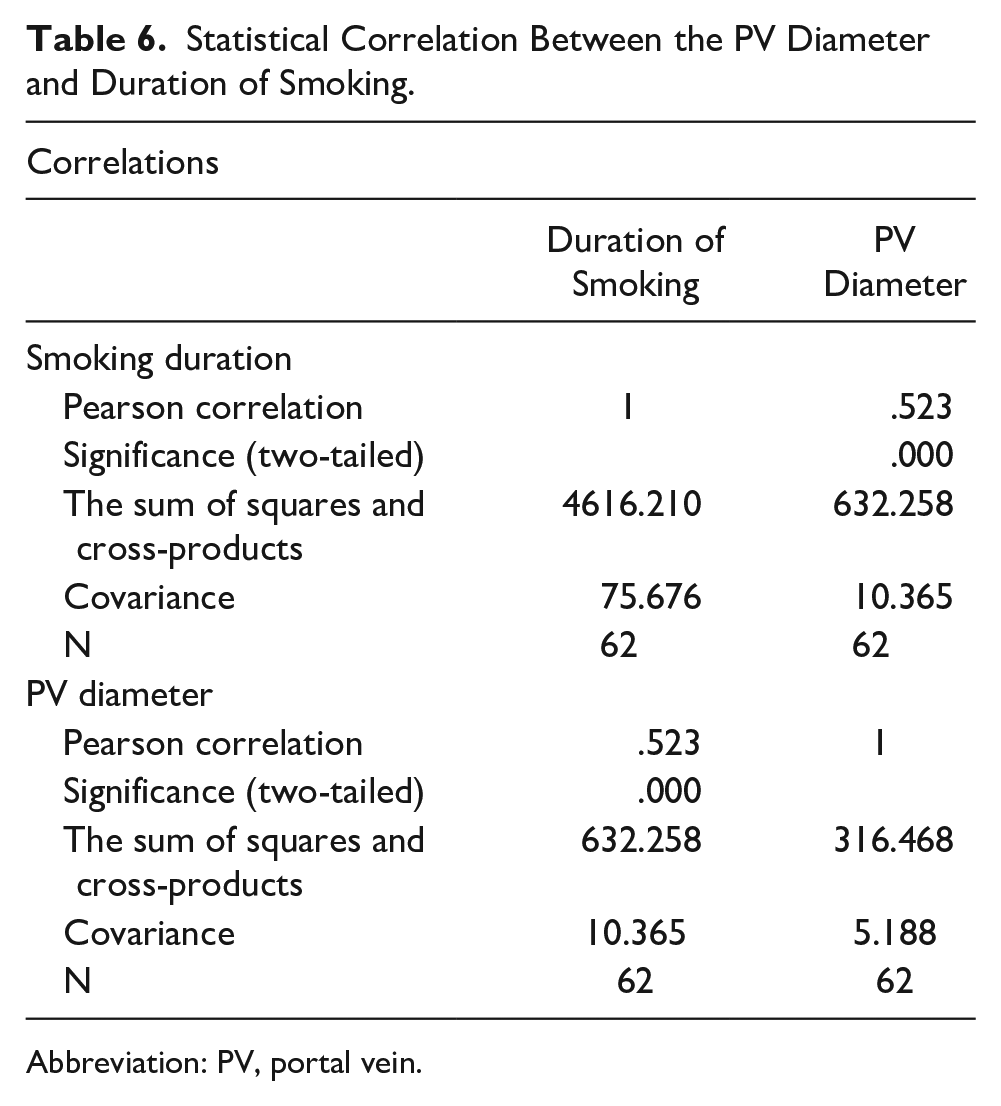
Abbreviation: PV, portal vein.
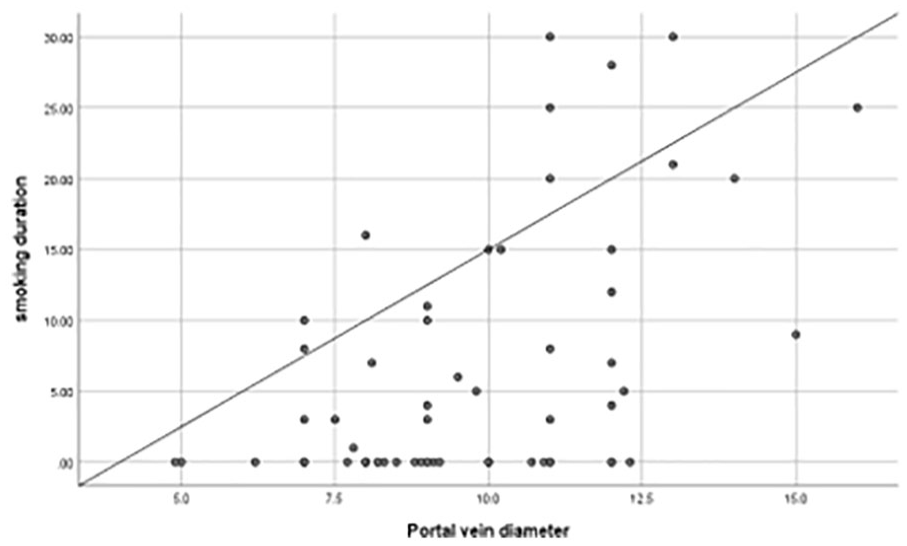
Scattered-plot depicting the association between the duration of smoking and the diameter of the portal vein (PV).
Table 7 summarizes the results of the chi-square test for the statistical analysis of the association between PV diameter and sex. No statistically significant association was observed between PV diameter and sex (P = .439).
The Results of the Chi-Square Test for Statistical Association Between the Portal Vein (PV) Diameter and Sex.
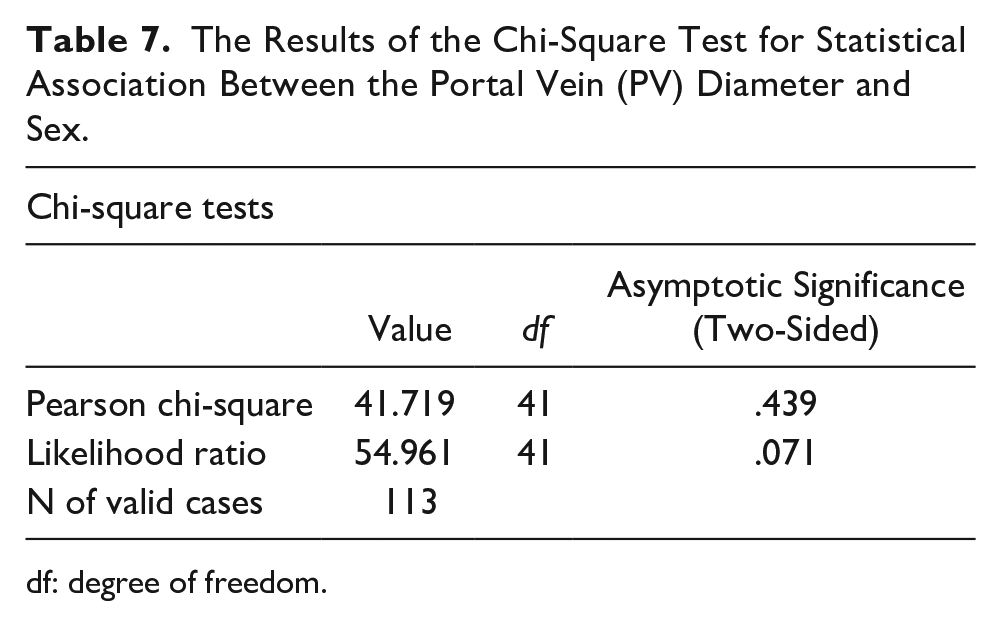
df: degree of freedom.
Discussion
This study aimed to evaluate the association of smoking, age, sex, and BMI with the PV diameter and compare the findings of participants who did and did not smoke.
The mean PV diameter was 9.60 ± 2.03 mm (Table 1), which is consistent with the findings of the studies by Albagir et al. 1 and Luntsi et al., 12 which reported mean PV diameters of 9.60 ± 1.41 mm and 10.40 ± 1.22 mm, respectively. Stamm et al. 14 used a different guideline to measure the mean PV diameter and reported a mean PV diameter of 15.5 ± 1.9 mm, which is significantly higher than the accepted upper limit.
This study revealed a strong significant association between smoking status and the PV diameter as the PV diameter increases. The data indicated that the mean PV diameter of the participants who did and did not smoke was 10.51 ± 2.35 mm and 9.25 ± 1.80 mm, respectively (Table 2). Moreover, the independent t-test revealed a strong association between smoking and an increase in the PV diameter (P = .01; Table 3). The boxplot (Figure 2) confirmed these findings. Thus, it can be concluded that the PV diameter increased more in participants who smoke than in participants who do not. A selective search of the literature did not yield published data comparing the PV diameter of participants who did and did not smoke. Rapaccini et al. 15 evaluated the acute effects of cigarette smoking on portal blood flow in men using Doppler and reported that the mean portal blood flow velocity, volume, and PV diameter increased significantly after the inhalation of the first cigarette. 15
This study revealed a statistically significant association between age and PV diameter (Table 4), consistent with the findings of the studies by Geleto et al., 4 Chand and Jaradi., 10 and Rapaccini et al., 15 which showed a statistically significant relationship between age and the PV diameter. In contrast, Albagir et al. 1 reported no statistically significant association between age and PV diameter. This difference in results may be attributed to the nature of their study, which included only young participants aged 20–25 years old. 1 Ahmed et al. 9 reported that PV dilatation increases with age and is more common in middle-aged individuals.
This study revealed a strong, statistically significant correlation between BMI and the PV diameter (P = .022; Table 5), which is consistent with the findings of the studies by Chand and Jaradi 10 and Luntsi et al., 12 which revealed a positive correlation between BMI and the PV diameter. 1 Aqeel et al. 11 concluded that BMI is statistically correlated with the PV diameter in female participants.
This study revealed no statistically significant association between the PV diameter and sex (P > .05) (Table 7). This finding is in contrast with those of the studies by Akanni et al., 2 Geleto et al., 4 and Rapaccini et al., 15 which showed a statistically significant association between sex and the PV diameter. Aqeel et al. 11 proposed that the association was only present between female sex and PV diameter.
Limitations
A major limitation of this study is its research design, which has limitations in terms of internal and external validity. The convenience sampling of participants and small sample size should also be considered as limitations. The study used an inclusion criterion of an unremarkable abdominal liver sonogram; however, this was not confirmed using other diagnostic tools. The asymptomatic participants could have had an undiagnosed cardiac disease, given that no echocardiographic study had been completed. Lastly, some variations in the PV diameter measurements may have occurred as the measurements were acquired by two investigators.
Conclusion
The findings of this study suggest that an increased PV diameter shows statistically significant associations with smoking, age, and BMI. No statistically significant association was observed between sex and the PV diameter. Smoking and an increased BMI may be associated with portal hypertension. Smoking and BMI are variables affecting the PV diameter that can be controlled; thus, public awareness and regulations may aid in reducing the negative health impact of these variables. Future studies with larger sample sizes and a random selection of participants must be conducted. In addition, the study participants should be recruited using more stringent inclusion criteria to ensure that the influence of cardiac and hepatic diseases is not present. Spreading awareness regarding smoking cessation and BMI control should be an essential part of public health programs.
Footnotes
Correction (March 2024):
This article has been updated from initial onlinefirst publication to correct the abbreviation for portal vein (PV) on page 3.
Ethics Approval
Ethical approval for this study was obtained from the Research and Ethics Committee of the College of Applied Medical Sciences, Taibah University, KSA (Approval Number/ID: 2023).
Informed Consent
Informed consent was not sought for this study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to this study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Key Takeaways
Smoking and an increased BMI may be potential risk factors for portal hypertension. Smoking cessation and BMI reduction may play an important role in the treatment of portal hypertension. Therefore, smoking cessation and BMI reduction should be considered in the treatment and management of vascular diseases.