
Abstract
Objective:
The prevalence of fatty liver disease is increasing among children. The aim of this study was to investigate a possible association between clinical and laboratory findings with the degree of fatty liver deposition, in pediatric patients.
Materials and Methods:
This study enrolled 323 pediatric patients with suspected fatty liver disease, who underwent a liver sonogram. The amount of fatty infiltration, within the liver, was assessed. The clinical data include age and body mass index (BMI), which were collected from their medical records.
Results:
The liver sonogram revealed fatty infiltration in 212 (66%) of the patients. Of those patients, 120 (38%) displayed mild infiltration, 65 (20%) exhibited moderate infiltration, and 27 (8%) demonstrated severe infiltration. Patients with severe fatty infiltration had significantly higher levels of alanine aminotransferase (ALT). The different levels of aspartate aminotransferase (AST), among patients, with varied degrees of fatty infiltration, were not statistically significant.
Conclusion:
A liver sonogram can be utilized to assess liver damage and inflammation, in pediatric patients, with fatty liver disease. Sonographers should prioritize evaluating the liver size, hepatic vasculature, and liver parenchyma for signs of fatty infiltration. Monitoring ALT levels appears to be crucial in managing pediatric patients, with nonalcoholic fatty liver disease (NAFLD).
The incidence of fatty liver disease in children is increasing, with rates reaching up to 10% in the United States. 1 This condition entails the buildup of fat in the liver, resulting in inflammation and damage. Initially, children with fatty liver disease may not exhibit noticeable symptoms; however, over time, they may develop fatigue, abdominal pain, and jaundice.1 –4 Fatty liver disease is linked to obesity, insulin resistance, and metabolic syndrome. If left untreated, severe liver damage may occur, including cirrhosis and liver failure.2,5 –10
Liver sonography and elastography are valuable diagnostic and surveillance tools to assess pediatric fatty liver disease.1,12 –15 These noninvasive and painless imaging techniques allow for the identification of fat deposition in the liver, assessment of disease severity, and tracking liver architectural changes over time.
Unlike other imaging methods such as computed tomography (CT), sonography does not employ ionizing radiation, making it safer for children.11,15 Moreover, it is widely available in most health care facilities and is more economical than alternative diagnostic imaging techniques.
However, liver sonography does have certain technical limitations. While it is useful for diagnosing and monitoring fatty liver disease in children, it may not be capable of distinguishing between specific types of liver diseases, such as nonalcoholic fatty liver disease (NAFLD). Nonalcoholic fatty liver disease is a milder form of liver disease, with the fat accumulation usually confined to the liver, and nonalcoholic steatohepatitis (NASH), which is a more serious form of liver disease. Nonalcoholic steatohepatitis is associated with the inflammation and scarring, often causing more extensive damage to the liver and having a distinct prognoses and treatment approaches. Thus, additional diagnostic tests such as magnetic resonance imaging (MRI) may be necessary to accurately identify the specific type of liver disease and determine the appropriate treatment plan. In addition, sonographic results can vary depending on the skill of the sonographer and the quality of the equipment. 16
Despite these limitations, liver sonography remains a valuable diagnostic tool in managing pediatric patients with fatty liver disease. Ongoing research may lead to technical advancements in sonographic imaging, which could provide more precise and reliable information for diagnosis and monitoring of this condition. In this study, the objective was to investigate the relationship between clinical and laboratory findings and the extent of fatty liver deposition in pediatric patients, based on suspected fatty liver disease.
Materials and Methods
Demographics
In this retrospective cohort study, a total of 323 pediatric patient cases, with suspected fatty liver disease, were selected. These patients had undergone liver sonography at a tertiary care hospital in Iran between January 2018 and December 2022. This study was approved based on an ethical review by the hospital’s Institutional Review Board. Informed consents were obtained from the parents or guardians of all participating patients.
The patient case selection criteria included pediatric patients, aged 2 to 18 years, who exhibited clinical suspicion of fatty liver disease. This was denoted by their elevated liver enzymes; abnormal liver function tests; or a history of obesity, insulin resistance, or metabolic syndrome. Exclusion criteria involved patients with a documented history of liver disease, viral hepatitis, or other chronic medical conditions affecting the liver.
Clinical data, including age, gender, body mass index (BMI), laboratory findings, and medical history, were gathered from medical records. Body mass index was further categorized based on a previous study and was assigned as follows: 17
18.5 to 24.9: normal;
25 to 29.9: overweight;
30 to 39.9: obese;
40 or higher: morbidly obese.
Sonographic Protocol
All sonographic examinations were conducted and interpreted by two radiologists with 9 years of experience in conducting abdominal sonography. The radiologists were also unaware of the patient’s clinical information. A WS80A (Samsung Medison Co., Ltd., Korea) ultrasound equipment system was used, with a curvilinear transducer (2.5–3.5 MHz), to examine the patients. The evaluation of the liver involved assessing its size, echogenicity, and the presence of fatty infiltration. The extent of fatty infiltration was classified as mild, moderate, or severe based on the liver’s echogenicity in comparison with the adjacent right kidney (see Figures 1–4).
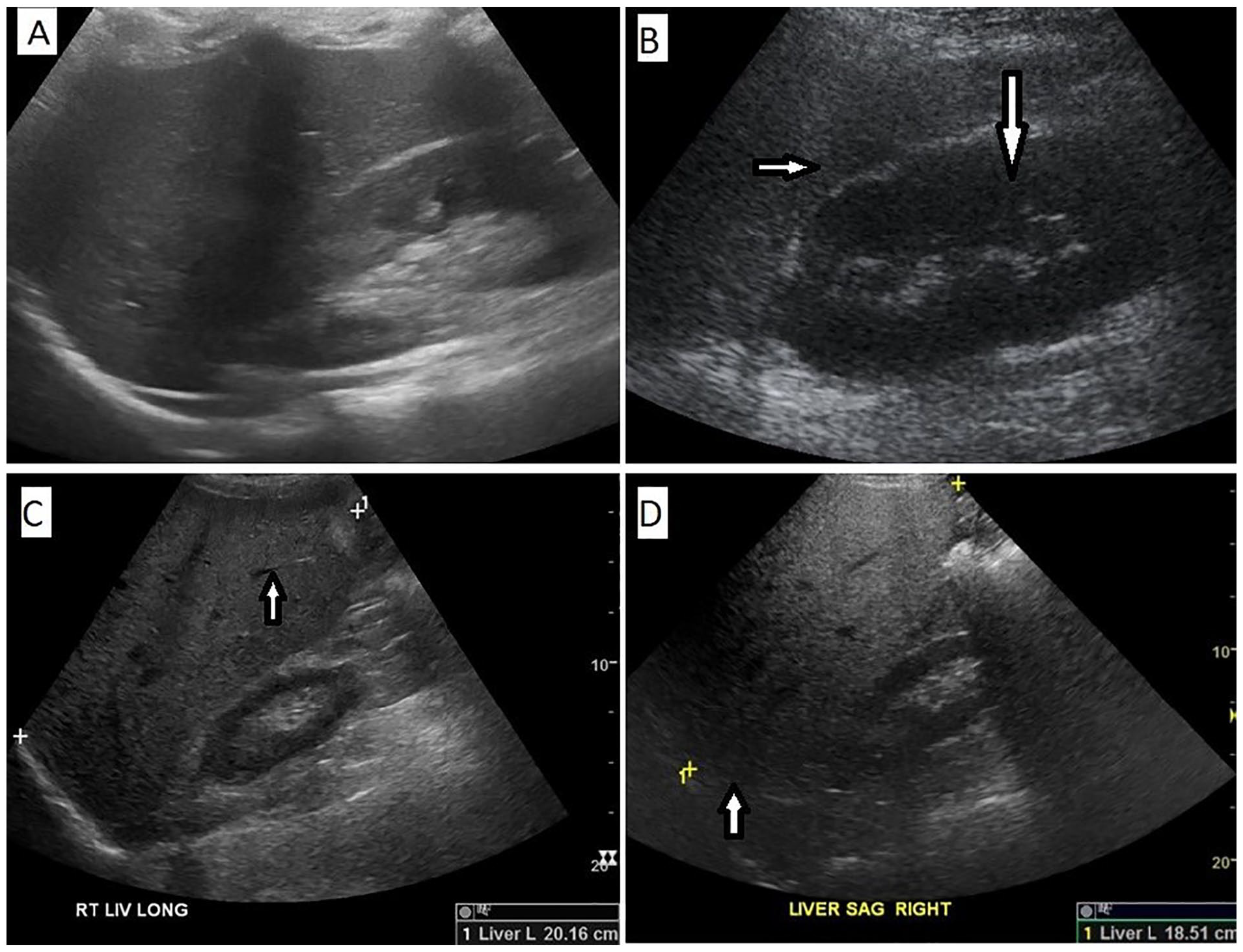
The sonographic grading of hepatic steatosis is illustrated: (A) An example of a normal liver. (B) An example of mild steatosis, which is demonstrated as increased liver echogenicity (see white short arrow) compared with the renal cortex (see white long arrow). (C) An example of moderate steatosis, which is shown as deceased conspicuity of hepatic vasculature (see white arrows). (D) An example of severe steatosis that is exhibited as decreased ability to visualize the diaphragm (see white long arrow) and deeper liver parenchyma (see white short arrow).
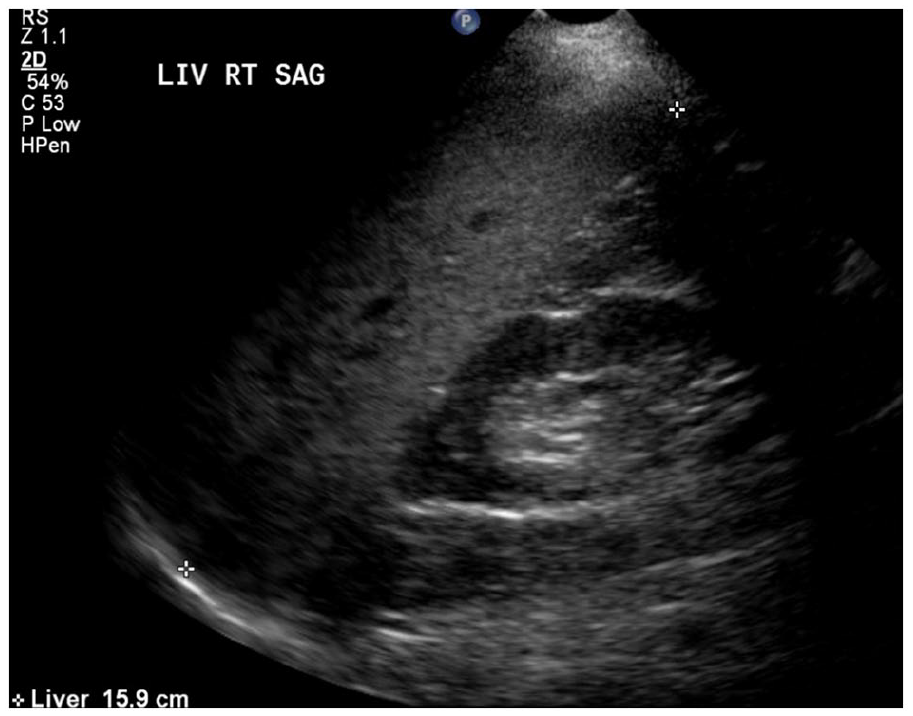
The liver sonogram of a 17-year-old obese male patient, which revealed a large liver measuring 159.0 cm and exhibited increased echogenicity consistent with moderate steatosis, as well as hepatomegaly.
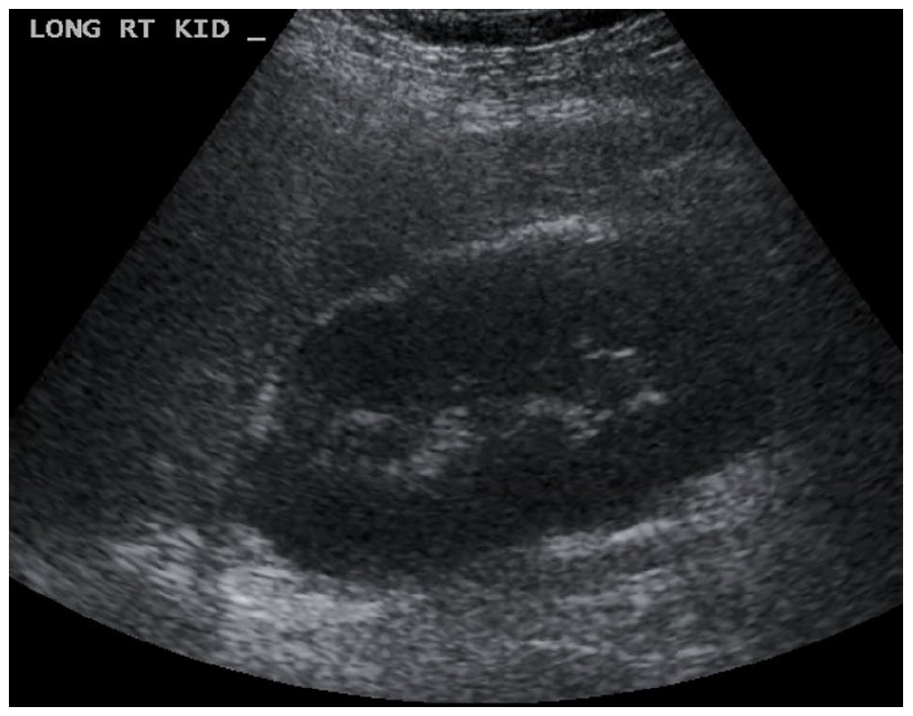
The liver sonogram of a 7-year-old obese female patient that demonstrated increased liver echogenicity when compared with the renal cortex and is consistent with mild steatosis.
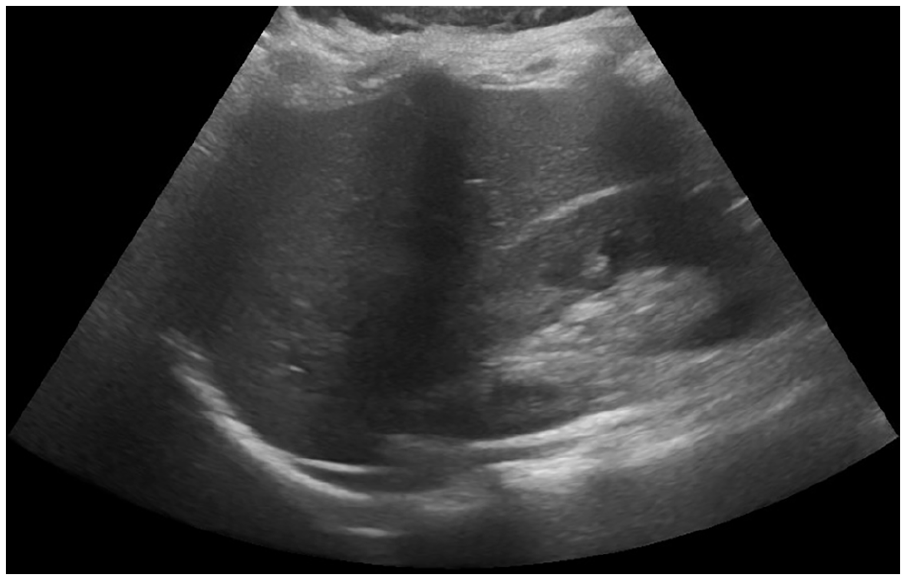
The liver sonogram of a 5-year-old female patient, with high BMI level, demonstrated a normal sonographic liver appearance.
The system for grading the sonographic level of hepatic steatosis was categorized as follows:
Mild steatosis: Increased liver echogenicity compared with the renal cortex;
Moderate steatosis: Increased liver echogenicity compared with the renal cortex along with deceased conspicuity of hepatic vasculature;
Severe steatosis: Increased liver echogenicity compared with the renal cortex along with decreased ability to visualize the diaphragm and deeper liver parenchyma.
Statistical Analysis
The clinical data analyzed using SPSS (SPSS Inc., IBM, Chicago, IL) statistical software, version 24, were used. Descriptive statistics were employed to analyze the data, and the findings were reported in terms of frequencies, percentages, and mean values. Clinical variables were measured for strength of association using analysis of variance (ANOVA), and a P value was set at .05, a priori.
Results
The study included 323 pediatric patients, of whom 181 (56%) were male and 142 (44%) were female. The mean age of the patients was 10.5 ± 3.8 years, and the mean BMI was 28.1 ± 4.5 kg/m2. The most common presenting symptom was abdominal pain (67%), followed by fatigue (33%) and jaundice (11%) (see Table 1).
The Study Cohort’s Characteristics Which Were Based on a Medical Chart Review.
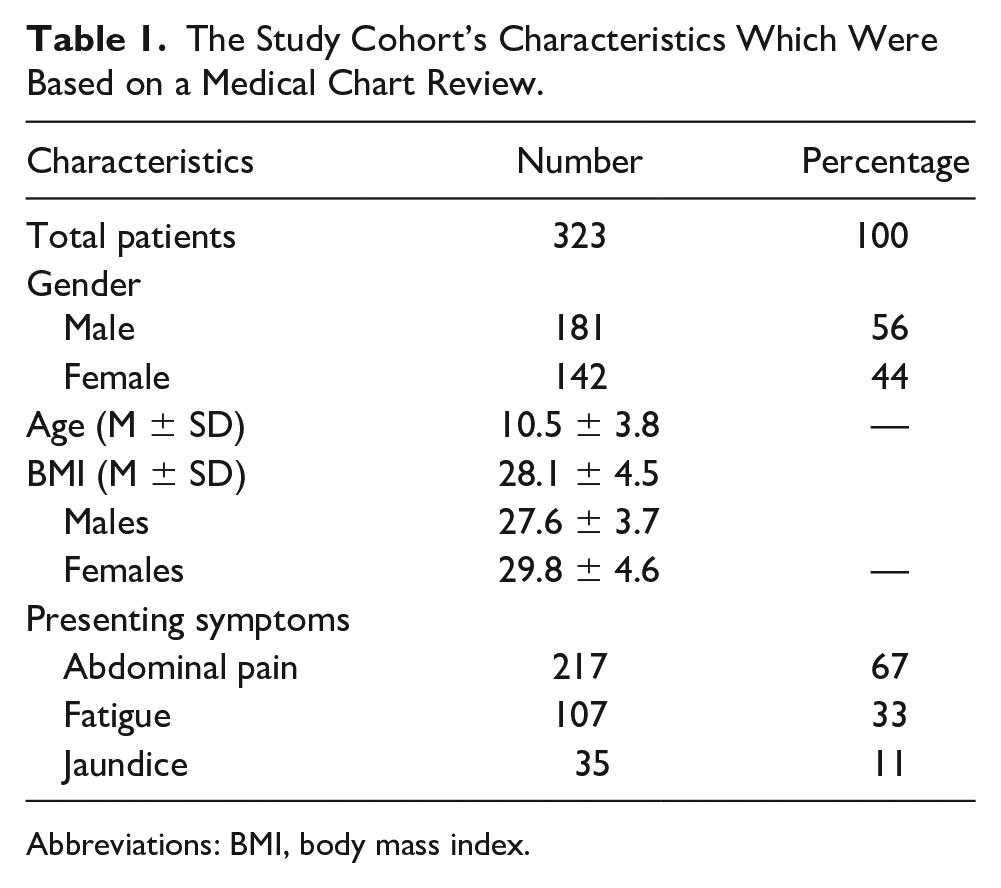
Abbreviations: BMI, body mass index.
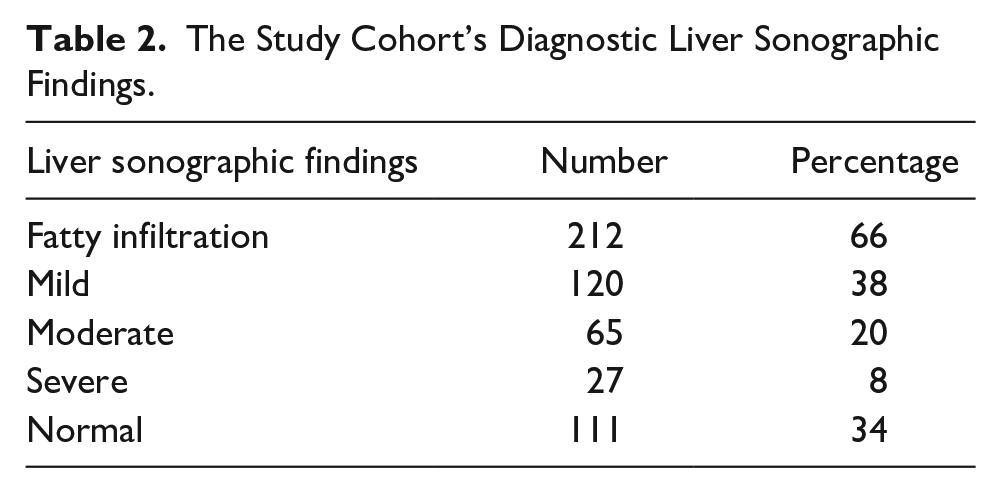
The liver sonogram revealed fatty infiltration in 212 (66%) patients, with 120 (38%) having mild, 65 (20%) having moderate, and 27 (8%) having severe fatty infiltration. The remaining 111 (34%) patients had a normal liver sonographic finding (see Table 2).
The Study Cohort’s Diagnostic Liver Sonographic Findings.
Furthermore, based on these findings, patients with severe fatty infiltration had higher levels of alanine aminotransferase (ALT) compared with patients with mild and moderate fatty infiltration, which was statistically significant (P = .005). Conversely, the different levels of aspartate aminotransferase (AST) among patients with varying degrees of fatty infiltration did not reach statistical significance (P > .05). Patients with moderate to severe fatty infiltration also had significantly higher levels of fasting glucose and insulin resistance (P < .05). The degree of fatty infiltration was significantly associated with high BMI levels, in the way that patients with moderate and severe fatty infiltration had higher levels of BMI compared with those with mild fatty infiltration, 29.7 ± 3.62 and 31.2 ± 3.9 versus 26.9 ± 3.1, respectively (P = .001) (see Table 3).
The Correlations Between the Degree of Liver Fatty Infiltration and Associated Clinical Parameters, in This Pediatric Cohort.
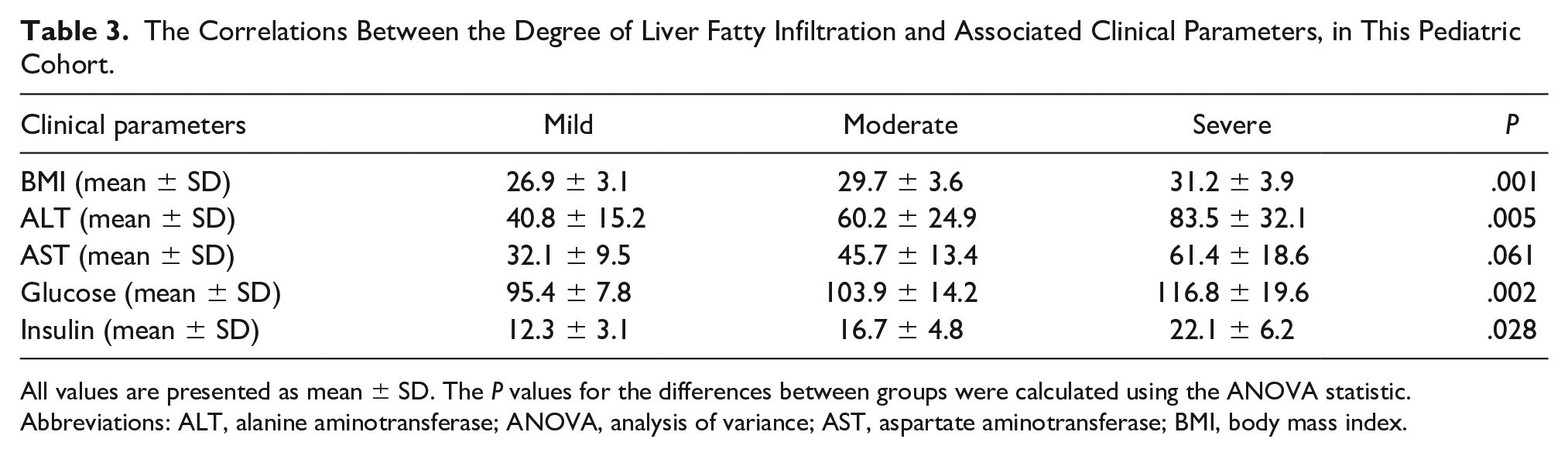
All values are presented as mean ± SD. The P values for the differences between groups were calculated using the ANOVA statistic.
Abbreviations: ALT, alanine aminotransferase; ANOVA, analysis of variance; AST, aspartate aminotransferase; BMI, body mass index.
Of the 111 patients with a normal liver sonogram, 39 (35%) had elevated liver enzymes, suggesting the presence of NAFLD despite the absence of fatty infiltration on their sonogram.
Discussion
The role of diagnostic imaging in various diseases has been well documented.18 –28 The objective of this study was to assess the role of liver sonography in the surveillance of pediatric patients with fatty liver. These findings revealed that most of the pediatric patients suspected of having fatty liver exhibited evidence of fatty infiltration on their liver sonogram. The prevalence of fatty infiltration in this study was determined to be 77%, which is higher than the reported prevalence in certain previous studies. For example, Sahota et al. reported a prevalence of 12.3%, while Shapiro et al. reported a prevalence of 26%. This disparity in prevalence may be attributed to several factors, including the high BMI observed in this study cohort and the additional variations in the characteristics of other study cohorts, across varied studies.10,12 Furthermore, this study findings revealed a significant association between the degree of fatty infiltration and BMI, which is consistent with prior research conducted by Elizabeth et al. 13 and Mohamed et al. 14 These studies have previously demonstrated a clear connection between obesity and fatty liver. It is worth noting that the similarity in patient protocols across these studies may contribute to the observed correlation. This study findings underscore the significance of lifestyle modifications and weight loss in the management of pediatric patients with fatty liver. Furthermore, the study revealed a noteworthy association between the extent of fatty infiltration and liver enzyme levels, particularly alanine transaminase (ALT). This finding agreed with previous research that has documented the correlation between fatty liver and liver enzyme levels. 15 In addition, a significant proportion of patients with normal liver sonographic findings displayed elevated liver enzyme levels, indicating the presence of NAFLD despite the absence of fatty infiltration on ultrasound examination. This highlights the significance of measuring liver enzyme levels in the follow-up of pediatric patients suspected of having NAFLD, even in the absence of fatty infiltration on their sonogram.
Several previous studies investigating the prevalence and risk factors of fatty liver disease in pediatric populations using sonography have reported diagnostic findings consistent with the current study. For example, a study conducted by D’Hondt et al. in China reported a prevalence of 53.7% in children aged 6 to 16 years. 29 Similarly, a study by Schwimmer et al. in the United States found that overweight and obese children had a higher rate of developing fatty liver disease (38%) compared with those with a normal BMI. 4 The significant association observed between the degree of fatty infiltration and liver enzyme levels, particularly ALT, aligns with previous studies. For instance, a study by Feldstein et al. found that children with fatty liver disease had higher levels of liver enzymes compared with those without the disease. 30 Overall, the results of this study, in conjunction with prior investigations, highlight the importance of early detection and monitoring of fatty liver disease in pediatric patients to prevent the progression to more advanced stages of liver disease. They also emphasize the role of liver sonography as a valuable tool in the diagnosis and monitoring of fatty liver disease among pediatric patients.
Limitations
The major limitation of this study was based on the research design and its threats to internal and external validity. The results from this large cohort cannot be generalized to the population. In addition, it is worth mentioning that other studies, such as those conducted by Pacifico et al. and Valerio et al. in Italy, have reported different prevalence rates of fatty liver disease in pediatric populations.31,32 These variations could be attributed to differences in study participants, such as BMI and the prevalence of obesity. Nevertheless, these study findings need to be replicated to confirm the results provided.
Conclusion
The findings of this study may suggest that the degree of fatty infiltration, detected on a liver sonogram, could serve as a diagnostic indicator of the severity of liver damage and inflammation, in pediatric patients suspected of fatty liver disease. When conducting a pediatric liver sonogram, sonographers should prioritize key areas such as liver size and position, hepatic vasculature, and liver parenchyma to identify any indications of increased liver echo pattern, which may suggest the presence of fatty liver. By assessing these factors, sonographers could contribute to accurately diagnosing and managing liver conditions, in pediatric patients. The results also highlight the importance of monitoring ALT levels in the clinical management of pediatric patients with NAFLD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved based on an ethical review by the hospital’s Institutional Review Board (IR.BMU.REC.9619).
Informed Consent
Informed consents were obtained from the parents or guardians of all participating patients.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because animals were not used in the study.