
Abstract
Objective:
The intima-media thickness (IMT) of the common carotid artery (CCA) can indicate cardiovascular and cerebrovascular disease risk, which could aid in early disease identification and prevention. This study was designed to correlate carotid artery IMT with age, obesity, diabetes, and hypertension using sonography.
Materials and Methods:
This cross-sectional cohort study included 300 individuals of all ages selected through convenient sampling at a university clinic in Lahore from November 2022 to February 2023. An Xario XG ultrasound equipment system (Toshiba, Tokyo, Japan) and a 7.5- to 10-MHz linear transducer was used to examine the patients.
Results:
The CCA-IMT was evaluated in 300 individuals (mean age 36.83 years). Significant statistical differences were observed between hypertensive/non-hypertensive and diabetic/non-diabetic individuals (P < .05). CCA-IMT was positively correlated with age and higher in obese/overweight individuals.
Conclusion:
This large cohort study found a significant difference in CCA-IMT between hypertensive/diabetic and normal individuals. CCA-IMT was positively correlated with age and body mass index.
Keywords
The common carotid artery intima-media thickness (CCA-IMT) refers to the measurement of the thickness of the innermost layer (intima) and the middle layer (media) of the carotid artery wall. The carotid arteries are located in the neck and provides a major blood supply to the brain and neck. 1 IMT is typically measured using sonography, and it can be used as a diagnostic indicator of atherosclerosis, or the buildup of fatty deposits in the lining of the artery, which elevates the risk of heart attack and stroke. A thicker IMT measurement indicates a greater likelihood of atherosclerosis and an increased risk of cardiovascular disease.2,3
Hypertension, diabetes, aging, and obesity have negative consequences for a healthy artery. 4 Hypertension is a major contributor to the risk of cerebrovascular and cardiovascular disorders. 5 Hypertension has also been shown to be positively correlated with increased intima IMT. 6 The thickening of the arterial walls can result in a decrease in the elasticity of the artery, which can contribute to the development of atherosclerosis. Atherosclerosis may indicate a correlation between diabetes and increased IMT, suggesting a potential direct cause-and-effect relationship. 7 Diabetes also has a significant impact on the CCA-IMT that can cause damage to the inner lining of the artery, known as endothelial dysfunction. 8 This can lead to inflammation resulting in increased CCA-IMT and the buildup of plaque in the artery walls. 9 CCA-IMT tends to increase with age. 10 In fact, age is one of the most important factors associated with CCA-IMT, and it has been estimated that CCA-IMT increases by approximately 0.007 mm, per year of age. 11 Overall, the age-related increase in CCA-IMT is a reflection of the cumulative effects of atherosclerotic risk factors over time. 12 Obesity is also a major risk factor for the development of carotid artery disease 13 and can have a significant impact on CCA-IMT. This may be due to the fact that obesity is often accompanied by other health problems such as hypertension, high cholesterol levels, and insulin resistance, which can all contribute to the development of atherosclerosis. 14
Carotid sonography is a real-time diagnostic screening tool that is commonly used by radiologists, to evaluate at-risk patients. It is generally accessible, inexpensive, quick, secure, and non-invasive. The CCA, the area of bifurcation, as well as the internal and external carotid branches are all evaluated as a part of an early detection method and surveillance tool. 15 On the grayscale sonographic image, the far vessel wall’s outer border and luminal border of the intima are measured to assess the CCA-IMT thickness. 16 CCA-IMT is the double-line pattern visualized on a grayscale sonogram and is formed by two parallel echogenic lines representing the junction of the vessel lumen with the intima and media-adventitia interface 17 as shown in Figures 1 and 2. Instead of looking at the lumen, CCA-IMT enables imaging of the artery wall, which is where the atherosclerotic disease is likely to occur. 18 Typically, the normal thickness of the CCA-IMT is under 0.9 mm. 19
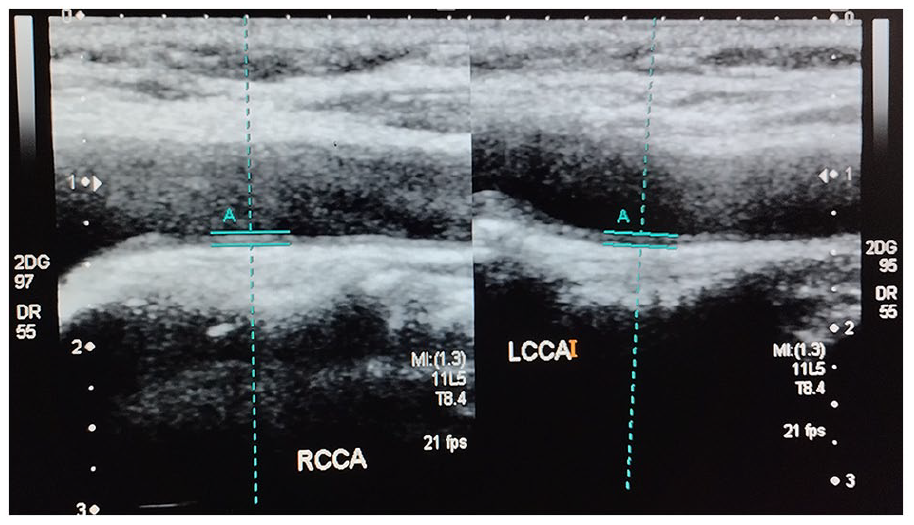
This dual sonogram demonstrates how the intima-media thickness of the common carotid artery was measured in an obese 50-year-old hypertensive female, with a body mass index (BMI) of 30.1. LCCA, Left Common Carotid Artery Intima Media Thickness; RCCA, Right Common Carotid Artery Intima Media Thickness; TCCA, Total Common Carotid Artery Intima Media Thickness; GD, Grey Scale Dynamic Range; DR, Dynamic Range.
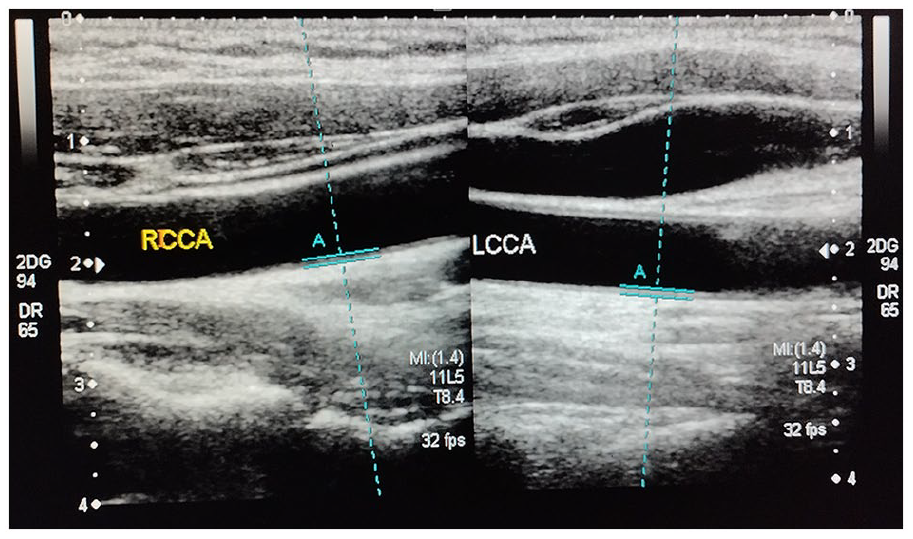
This dual sonogram shows how the intima-media thickness of the common carotid artery was measured in a 23-year-old female, with a body mass index (BMI) of 20.3. LCCA, Left Common Carotid Artery Intima Media Thickness; RCCA, Right Common Carotid Artery Intima Media Thickness; TCCA, Total Common Carotid Artery Intima Media Thickness; GD, Grey Scale Dynamic Range; DR, Dynamic Range
The research question and purpose of the study was to investigate the sonographic association between CCA-IMT and age, obesity, and hypertension. By analyzing the correlation between CCA-IMT and these factors, the study aimed to understand the potential impact of age, obesity, and hypertension on carotid artery health and identify potential risk factors associated with atherosclerosis development. This research effort was designed to contribute valuable insights into the early detection and management of atherosclerosis and related cardiovascular diseases. Therefore, the objective was to correlate CCA-IMT with age, obesity, diabetes, and hypertension using sonography.
Materials and Methods
A cross-sectional, cohort study was performed to determine the sonographic association of CCA-IMT with age, obesity, diabetes, and hypertension. This research was reviewed and approved by the University of Lahore’s Research Ethics Committee (REC-UOL-103-05-2023). The study consented 300 individuals, who were examined for CCA-IMT on both the right and left sides. In this study, the sonographic IMT measurements were performed using a standardized imaging procedure. The sampling electrocardiogram was gated, which ensured that the images were frozen at the same point of the cardiac cycle and minimize variability, due to cardiac motion artifacts. Multiple measurements of CCA-IMT were taken for each patient, and these measurements were then averaged to improve accuracy and reliability. The IMT of the CCA was measured at a site 1.0 cm proximal to the carotid bulb while the patient was laying supine. Obese, non-obese, or overweight males and females of all ages were included, as well as hypertensive, diabetic, and normal individuals. Patients whose body mass index (BMI) was more than 25 kg/m2 were considered as overweight, while patients with a BMI more than 30 kg/m2 were considered obese. 20 Patients with only a single risk factor were included, as part of the study. Patients with any underlying carotid pathologies such as carotid endarterectomy, stenting, or comorbidity were excluded. Pregnant women were also excluded. During the sonographic examination, patients were positioned supine on an examination couch, with their neck extended. The head was rotated 45° away from the side of the carotid artery being examined, to ensure accurate measurements of CCA-IMT. To clarify the methods employed in producing repeated results, the measurements were performed manually by trained health care professionals. The sonographic measurements were taken during both systole and diastole to gather comprehensive data. The duration of data collection was 4 months, from November 2022 till February 2023, and data were collected from a university ultrasound clinic in Lahore. An Xario XG ultrasound equipment system (Toshiba, Tokyo, Japan) and a 7.5- to 10-MHz linear transducer was used to examine the patients.
Data Analysis
Data analytics were performed using SPSS (IBM, SPSS Inc., Chicago, IL) version 26 software. A correlational analysis was planned to explore the associations between CCA-IMT, age, and obesity. In addition, an analysis of variance (ANOVA), post hoc analysis, and t-statistics were selected to assess the statistical significance of the relationships between these variables. The P value was set at .05, a priori.
Results
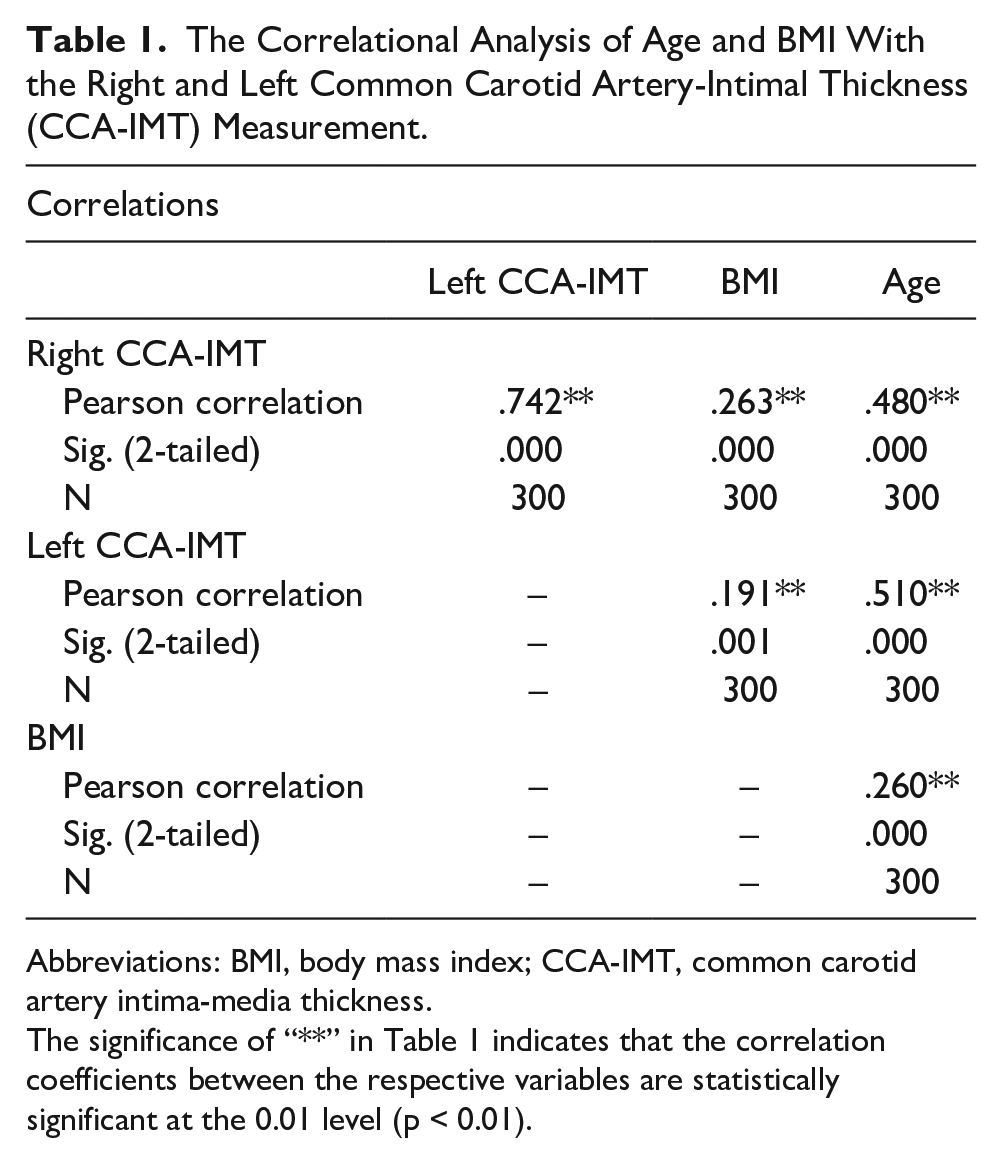
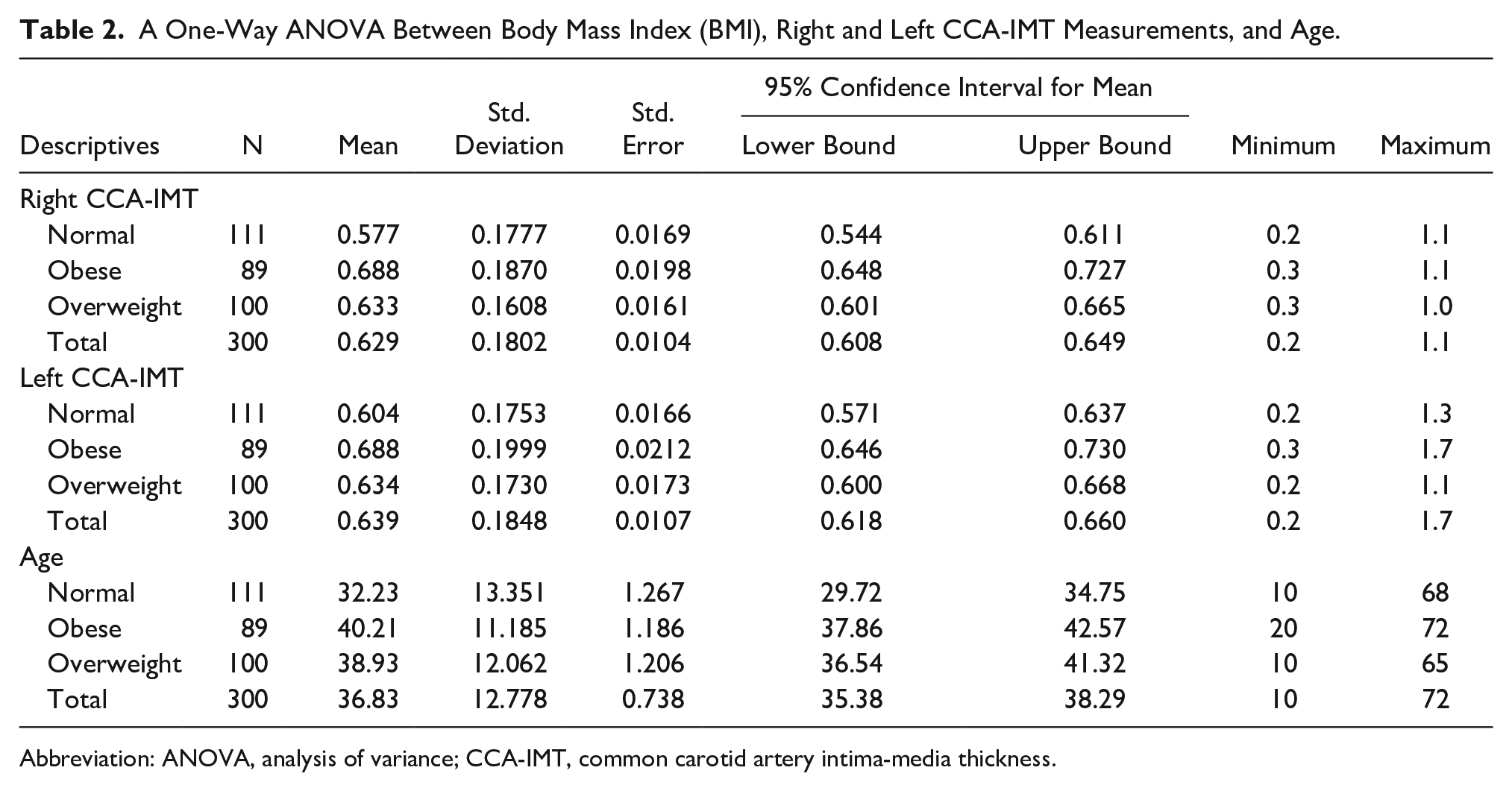
The descriptive data based on the 300 consented individuals were 262 females and 38 males, for a total sample size of 87.3% and 12.7%, respectively. In this cohort, 124 patients (41.3%) were hypertensive, which comprised 109 females and 15 males. There were 47 patients who were diabetic, including 43 females and 4 males. The cohort’s mean age was 36.83 years. Based on the 300 participants, there were 111 patients that were deemed of normal weight, 89 were obese, and 100 patients were overweight. Figures 1 and 2 demonstrate how the IMT of the CCA was measured. Correlations between CCA-IMT, age, and BMI are summarized in Table 1. A statistically significant correlation was observed between age and right CCA-IMT (P = .000), age and left CCA-IMT (P = .000), BMI and right CCA-IMT (P = .000), and BMI and left CCA-IMT (P = .001). The mean and standard deviation (SD) measurements of right and left CCA-IMT for normal, obese, and overweight individuals are listed in Table 2. For normal, obese, and overweight groups, the total mean and SD of the right CCA-IMT was 0.62 ± 0.18 mm, and the total mean and SD of the left CCA-IMT was 0.63 ± 0.18 mm.
The Correlational Analysis of Age and BMI With the Right and Left Common Carotid Artery-Intimal Thickness (CCA-IMT) Measurement.
Abbreviations: BMI, body mass index; CCA-IMT, common carotid artery intima-media thickness.
The significance of “**” in Table 1 indicates that the correlation coefficients between the respective variables are statistically significant at the 0.01 level (p < 0.01).
A One-Way ANOVA Between Body Mass Index (BMI), Right and Left CCA-IMT Measurements, and Age.
Abbreviation: ANOVA, analysis of variance; CCA-IMT, common carotid artery intima-media thickness.
Figures 3 and 4 depict the mean of right and left CCA-IMT in the normal, obese, and overweight groups as 0.57 mm, 0.68 mm, and 0.63 mm and as 0.60 mm, 0.68 mm, and 0.63 mm, respectively. In addition, Figure 5 provides the mean age for the normal, obese, and overweight patient groups as 32.23 years, 40.21 years, and 38.93 years, respectively.
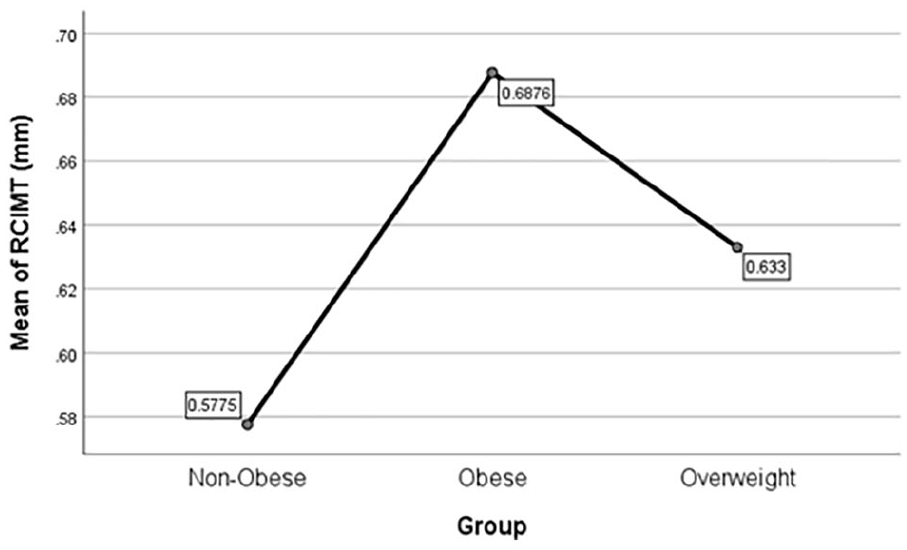
A graph of the mean right common carotid artery-intimal thickness (CCA-IMT) within the obese, normal, and overweight patient groups. RCIMT; Right common carotid artery intima media thickness.
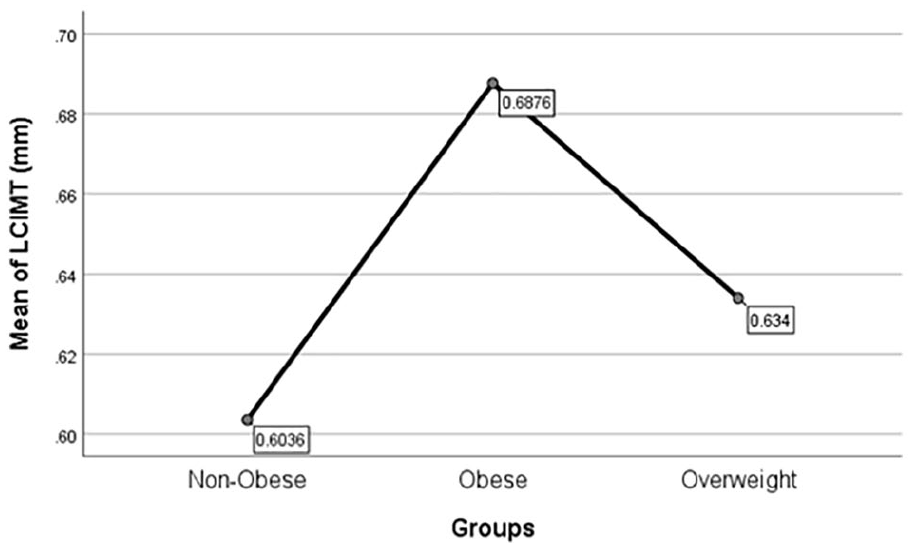
A graph of the mean left common carotid artery-intimal thickness (CCA-IMT), within obese, normal, and overweight patient groups. LICMT; Left common carotid artery intima media thickness.
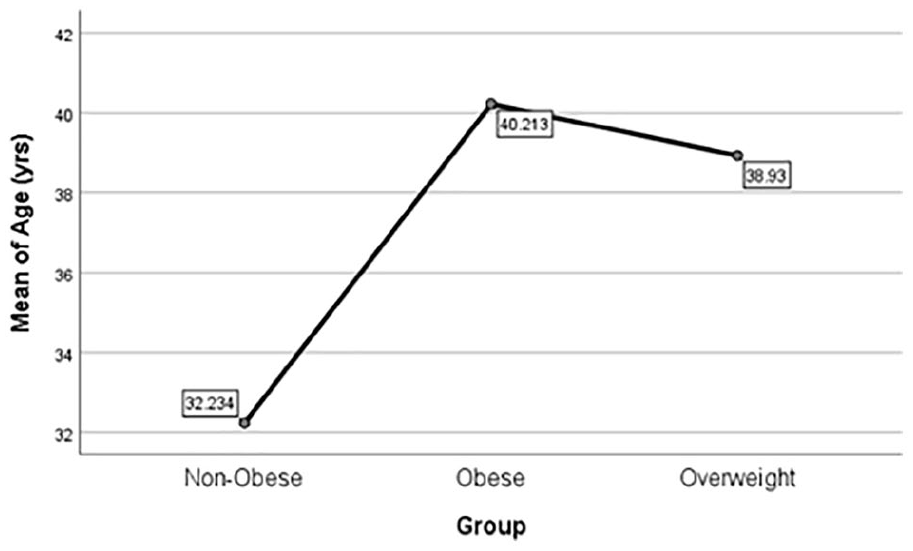
A graph of the mean ages within the obese, normal, and overweight patient groups.
Tables 3 and 4 display the mean and SD, as well as the mean difference of right and left CCA-IMT for the obese, normal, and overweight groups. An ANOVA was run between BMI, right and left CCA-IMT, and age, and it revealed that the mean and SD of right and left CCA-IMT of the three groups were significantly different. The P values for the differences among means was P = .000 and P = .005. The mean and SD for age in all three groups was also significantly different (P = .000). A post hoc analysis between BMI, right and left CCA-IMT, and age indicated that the right CCA-IMT mean was statistically significant between the obese, normal, and overweight groups. The left CCA-IMT mean was significant between the obese and normal groups, and the obese and overweight groups, but not significant between the normal and overweight groups. The age mean difference between the obese and normal groups and that between the overweight and normal groups were significant. However, in the obese and overweight groups, the age mean difference was not statistically significant.
A One-Way ANOVA Between Body Mass Index, Right and Left CCA-IMT, and Age, Within the Patient Cohort.
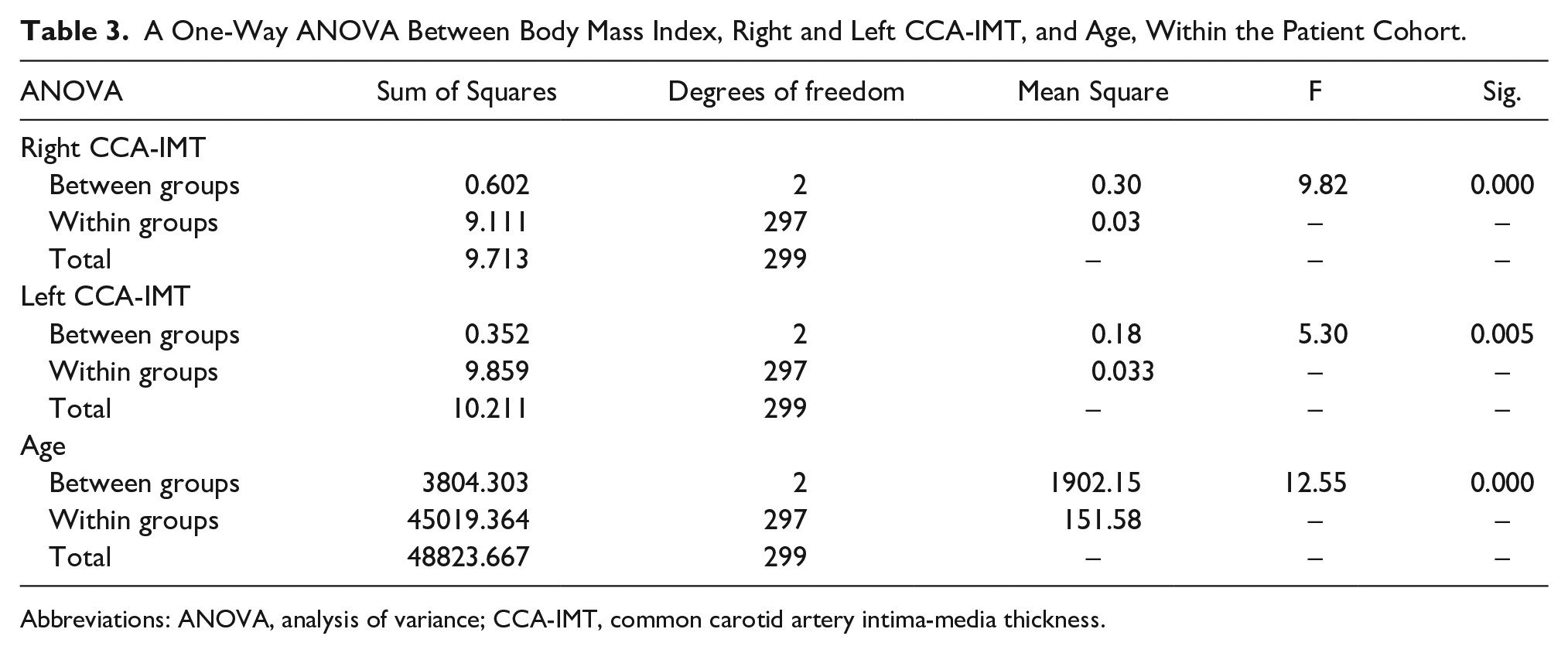
Abbreviations: ANOVA, analysis of variance; CCA-IMT, common carotid artery intima-media thickness.
The Post-Hoc Analysis Between Body Mass Index (BMI), Right and Left CCA-IMT Measurements, and Age.
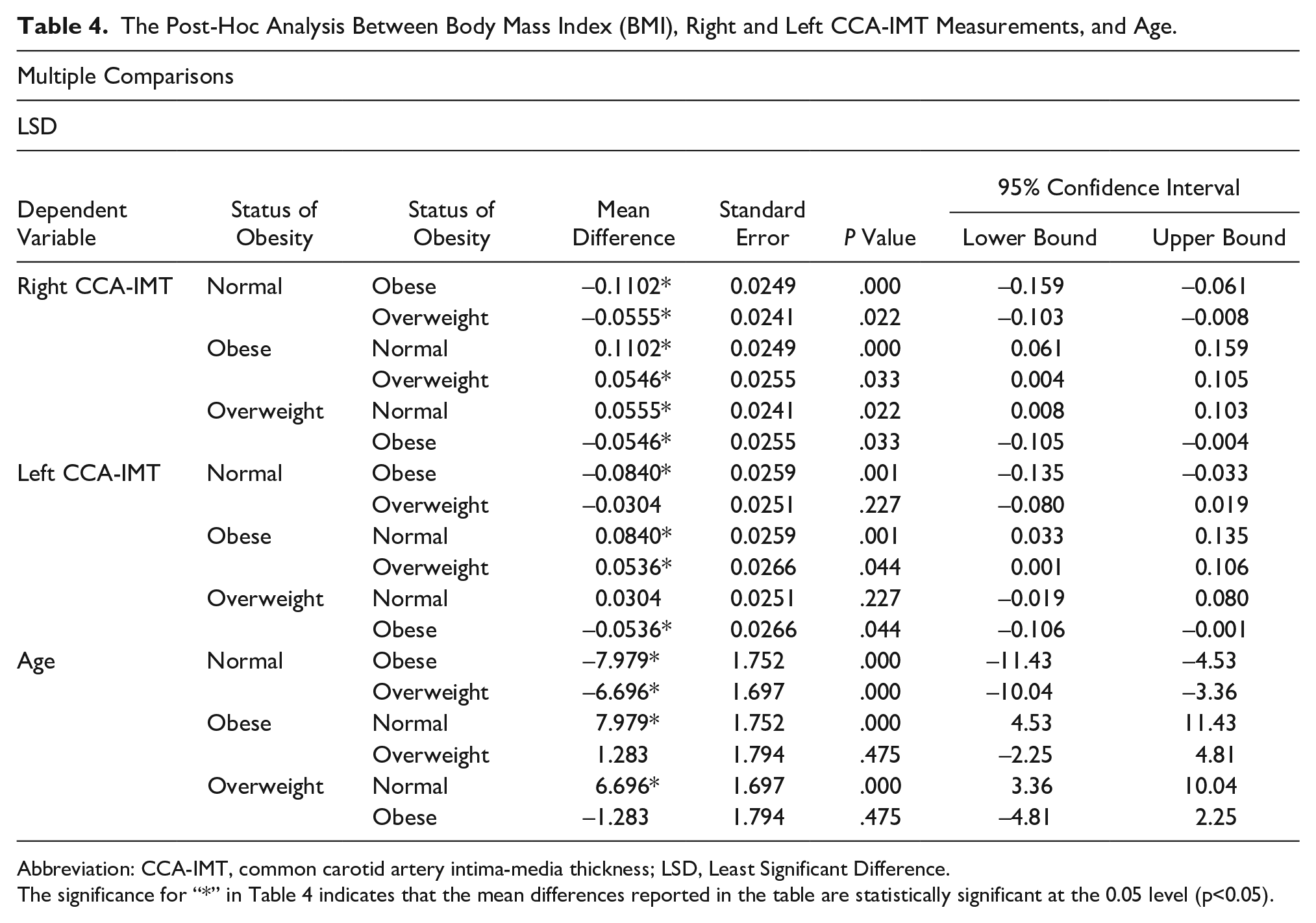
Abbreviation: CCA-IMT, common carotid artery intima-media thickness; LSD, Least Significant Difference.
The significance for “*” in Table 4 indicates that the mean differences reported in the table are statistically significant at the 0.05 level (p<0.05).
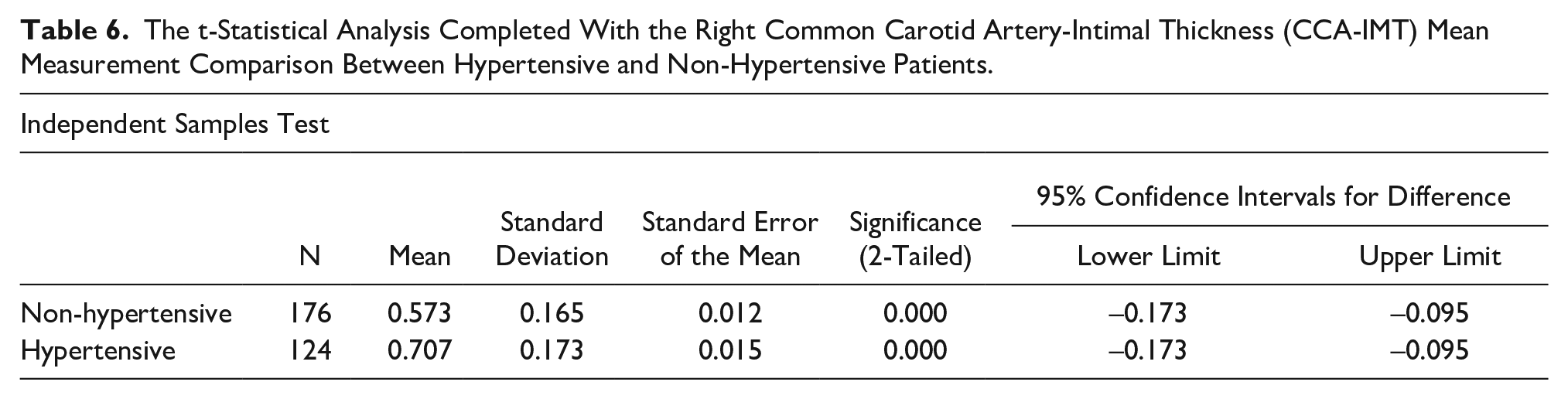
Table 5 presents the mean and SD, for the right and left CCA-IMT, in hypertensive and non-hypertensive individuals. The measured values were 0.70 ± 0.17 mm and 0.57 ± 0.16 mm for the right CCA-IMT and 0.71 ± 0.19 mm and 0.58 ± 0.15 mm for the left CCA-IMT, respectively. The overall mean and SD, for both hypertensive and non-hypertensive patients, was 0.62 ± 0.18 mm for the right CCA-IMT and 0.63 ± 0.18 mm, for the left CCA-IMT. The t test results for the right and left CCA-IMT mean comparison between hypertensive and non-hypertensive individuals showed a significant difference (P = .000) as shown in Tables 6 and 7.
The Mean Measurement of the Right and left Common Carotid Artery-Intimal Thickness (CCA-IMT) Measurements, in Hypertensive and Non-Hypertensive Patients.
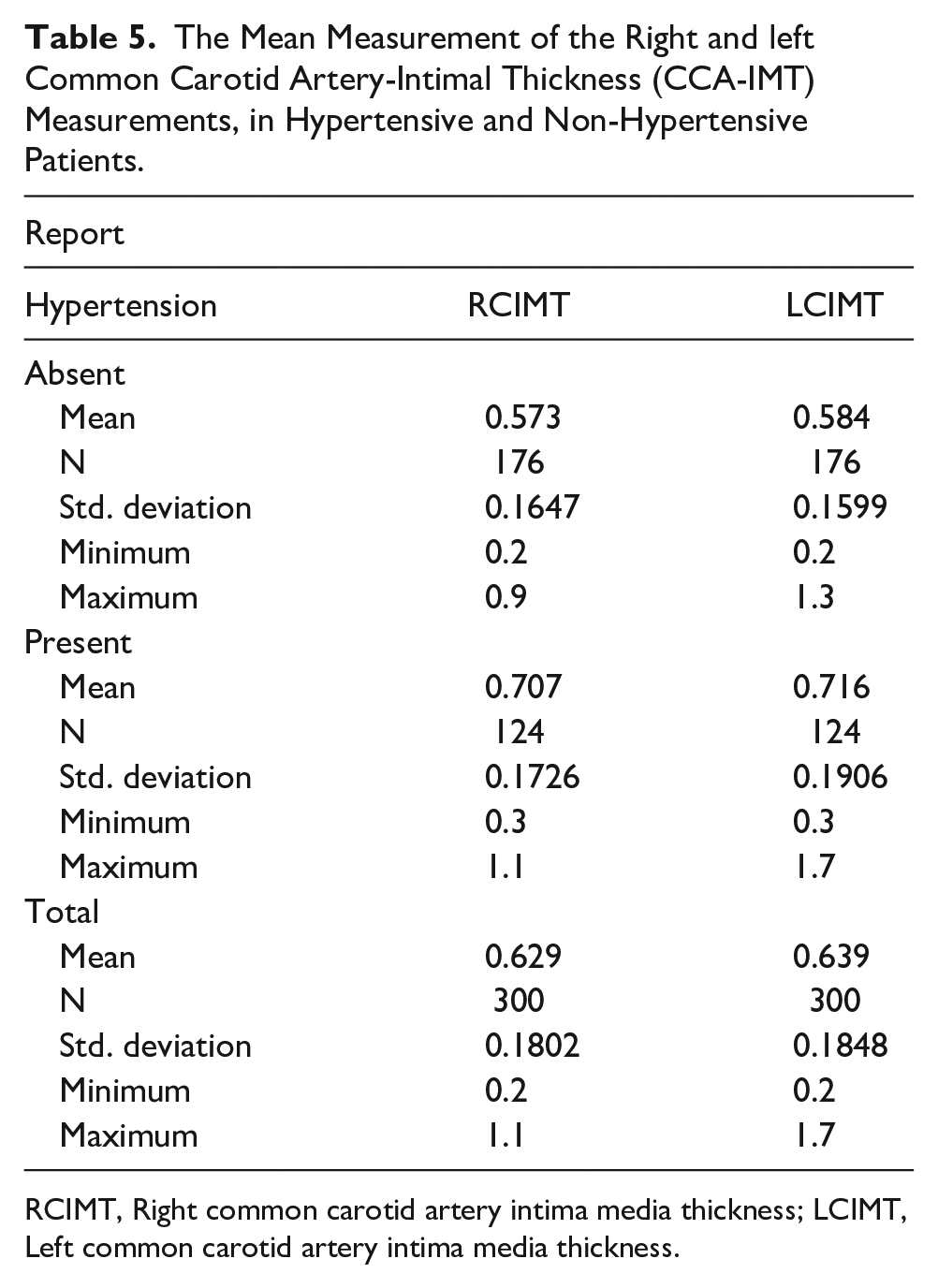
RCIMT, Right common carotid artery intima media thickness; LCIMT, Left common carotid artery intima media thickness.
The t-Statistical Analysis Completed With the Right Common Carotid Artery-Intimal Thickness (CCA-IMT) Mean Measurement Comparison Between Hypertensive and Non-Hypertensive Patients.
The t-Statistical Analysis Completed With the Left Common Carotid Artery-Intimal Thickness (CCA-IMT) Mean Measurement Comparison Between Hypertensive and Non-Hypertensive Patients.
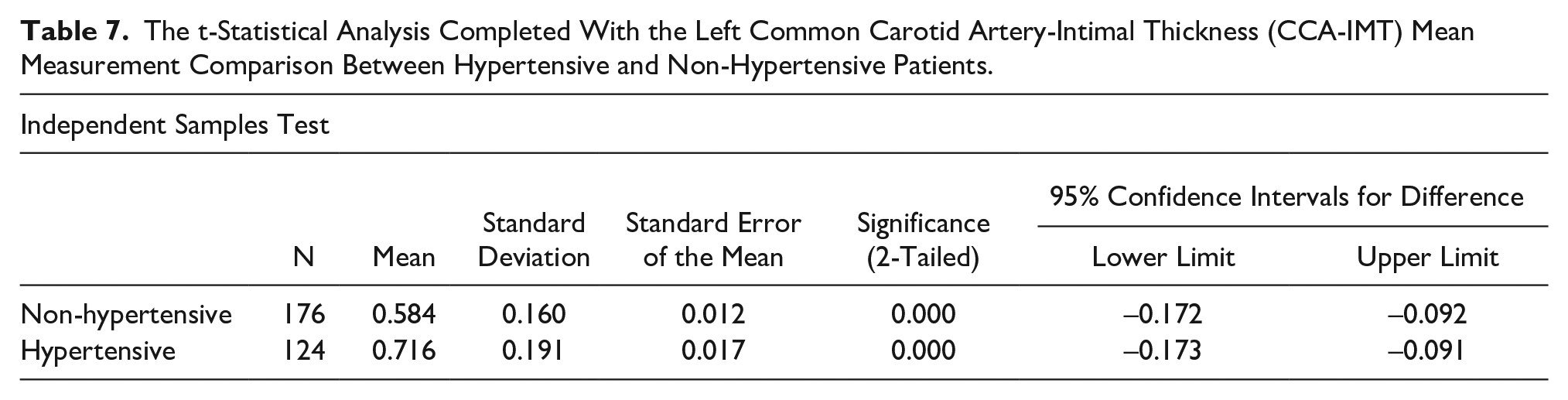
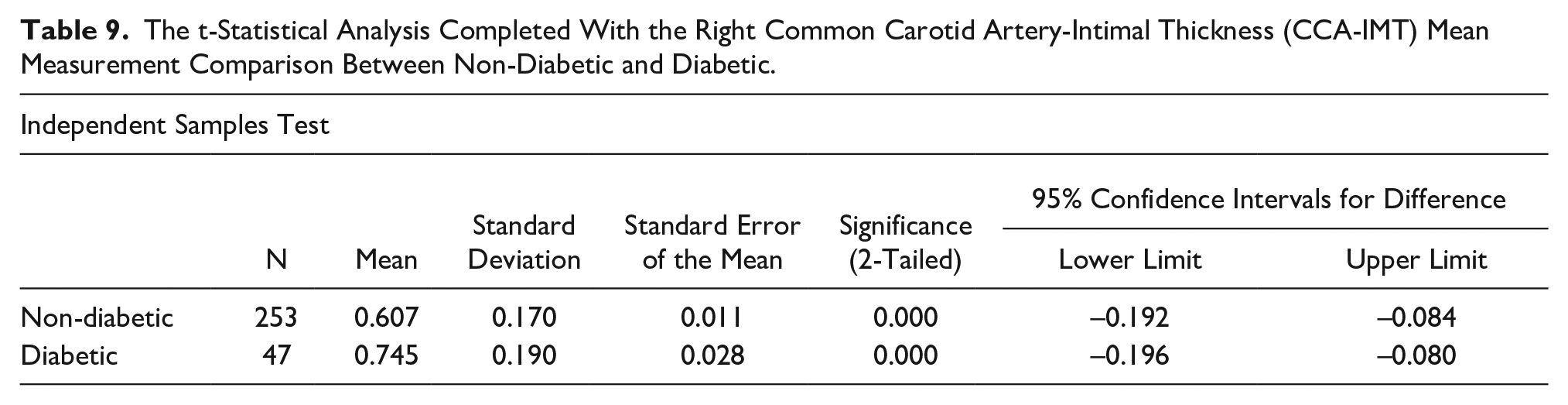
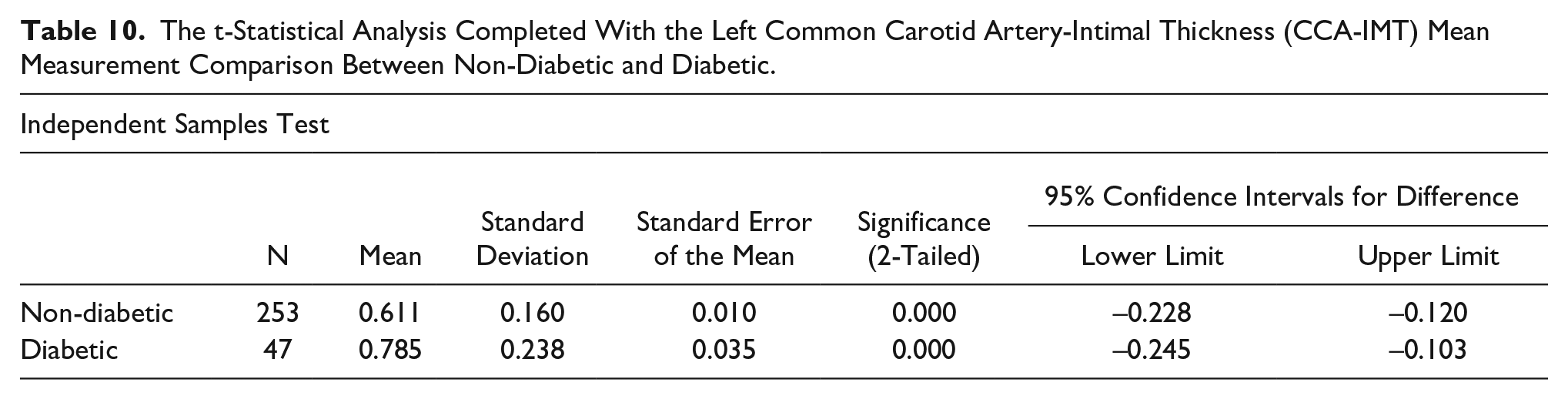
Table 8 provides the mean and SD for the right CCA-IMT, in the non-diabetic and diabetic patients, as 0.60 ± 0.17 mm and 0.74 ± 0.18 mm, respectively. For the left CCA-IMT, the mean and SD for non-diabetic and diabetic individuals were 0.6 ± 0.15 mm and 0.78 ± 0.23 mm, respectively. The overall mean and SD, for both non-diabetic and diabetic patients, were 0.62 ± 0.18 mm for right CCA-IMT and 0.63 ± 0.18 mm for left CCA-IMT, respectively. The t test confirmed that the right CIMT mean for both non-diabetic and diabetic patients was significantly different (P = .000) as shown in Tables 9 and 10.
The Mean Measurement of the Right and Left CCA-IMT Measurements, in Diabetic and Non-Diabetic Patients.
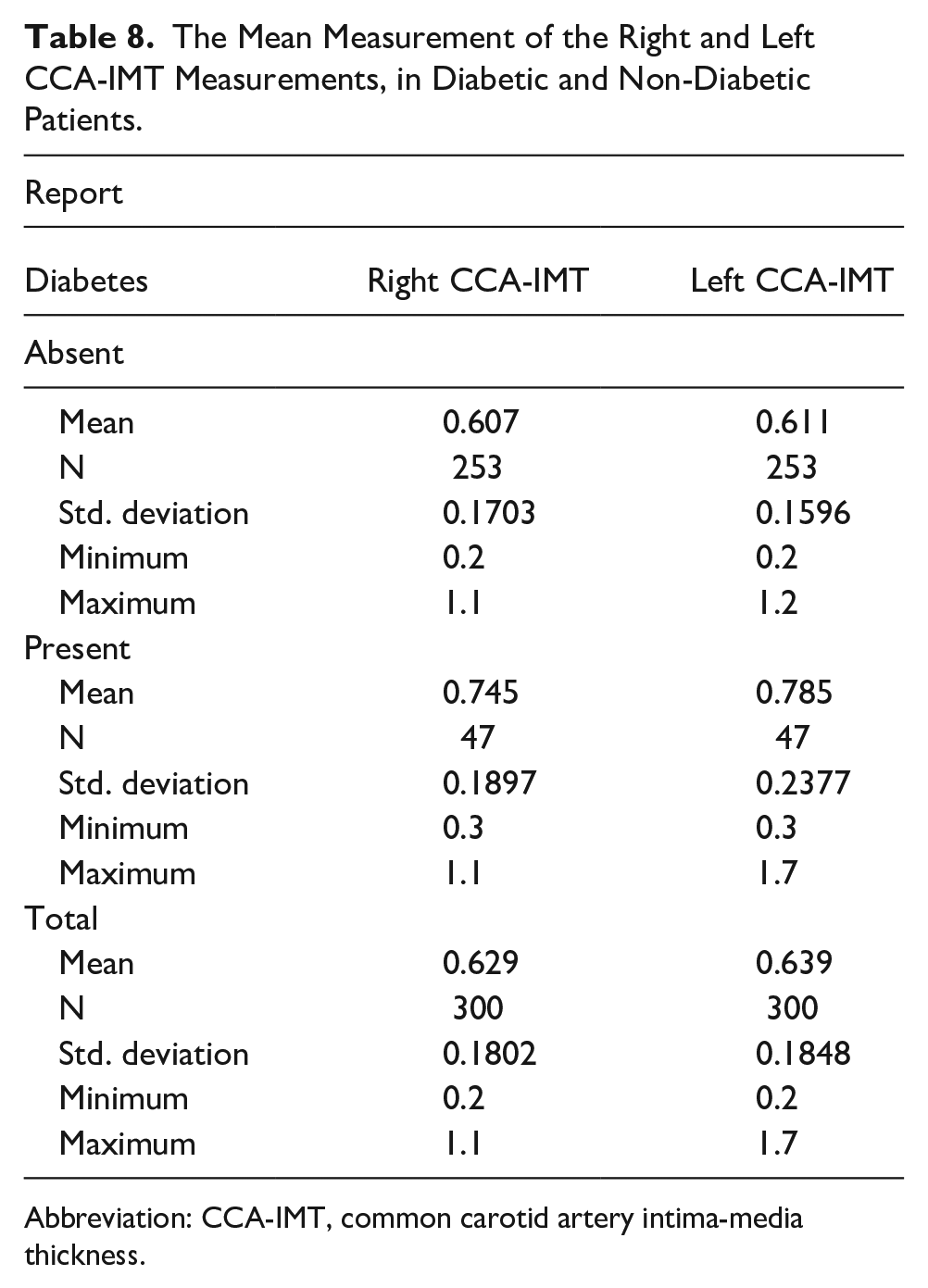
Abbreviation: CCA-IMT, common carotid artery intima-media thickness.
The t-Statistical Analysis Completed With the Right Common Carotid Artery-Intimal Thickness (CCA-IMT) Mean Measurement Comparison Between Non-Diabetic and Diabetic.
The t-Statistical Analysis Completed With the Left Common Carotid Artery-Intimal Thickness (CCA-IMT) Mean Measurement Comparison Between Non-Diabetic and Diabetic.
Overall, the results indicated significant associations between CCA-IMT, age, BMI, hypertension, and diabetes, supporting the relevance of these factors in the context of atherosclerosis and cardiovascular health.
Discussion
The current study found a robust association of increasing age (P = .000) and BMI (P = .000 and P = .001) with bilateral CCA-IMT. The study also revealed a significant difference between the right and left CCA-IMT means of hypertensive and non-hypertensive individuals (P = .000) and between diabetic and non-diabetic individuals (P = .000). Many studies have found a meaningful connection between IMT and cardiovascular risk factors. In a study by Sharma et al., 21 they discovered statistically significant changes in IMT between normotensive and hypertensive subjects.
In a study conducted by Jourdan et al., 22 they found that the CCA-IMT showed a slight increase with age and exhibited a normal distribution among their youngest subjects. However, in the peri- and post-pubertal age groups, the distribution of CCA-IMT was positively skewed (P < .001). In addition, it was observed that CCA-IMT had a stronger correlation with height than with age. 22
Raju et al. 23 conducted a study in which they found that, when compared to controls (0.54 ± 0.09 mm), the hypertension patients’ mean CCA-IMT was substantially greater (0.82 ± 0.32 mm); however, there was no significant variability in BMI. The present study also found a thicker IMT in hypertensive patients than normal patients but also showed a significant correlation of BMI with right and left CCA-IMT (P = .000 and P = .001).
While Shams et al. 21 reported that their findings did not reveal any significant difference in IMT between hypertensive and non-hypertensive patients, the current study demonstrated a significant difference in IMT between hypertensive and non-hypertensive individuals.
In a study conducted by Pujia et al., 24 they were able to determine if those patients with non-insulin-dependent diabetic mellitus (NIDDM), known to have a high risk of atherosclerosis, had a larger CCA-IMT. Comparing NIDDM patients to control participants, it was shown that they had greater IMT, higher levels of triglycerides, and lower concentrations of high-density lipoprotein (HDL) cholesterol. 24 In both groups, IMT had a negative connection with HDL cholesterol and a positive relationship with age and high blood pressure. 24
According to the study results provided by Luo, among patients between the ages of 35 and 65 years, the left CCA-IMT exhibited a significant increase in thickness compared to the right (P = .01–.05), and the difference was significant (P = .001) as both CIMTs increased in size with age. 25
Sajja et al. 26 found that children who were overweight or obese had a greater mean CCA-IMT than the children with normal BMI (0.5 ± 0.1 mm vs. 0.34 ± 0.05 mm). In the current study, a significant correlation was observed between BMI and the right CCA-IMT (P = .000) and between BMI and the left CCA-IMT (P = .001). In the Sajja study, age and gender had no effect on the mean intimal medial thickness. 26 In contrast, the current study showed a significant correlation between age and CCA-IMT (P = .000).
Ibinaiye et al. 27 conducted research to determine how the CCA-IMT and the blood pressure, age, and BMI of hypertensive, within adult patients, were related. Their study concluded that age and blood pressure were positively linked with carotid artery intima-media thickness, while BMI revealed a negative connection. 27 But in the current study, it is shown that a positive correlation existed between age and hypertension, as well as with BMI.
A study by Garcia et al. 28 revealed that IMT positively correlated with BMI score and was higher in children who were overweight or obese, showing increased likelihood of heart disease in that cohort. The current study also revealed a strong correlation between CCA-IMT and BMI.
According to Freitas et al., 29 CCA-IMT was strongly linked with age, especially after the age of 64 years. For the hypertensive patients, the current study also revealed a statistically significant positive connection between age and CCA-IMT.21,30
Limitations
The major limitation to this study was the research design and the convenient sample of patients. The threats to internal and external validity are such that generalizations cannot be made. An added limitation was the limited time for the data collection. It was also a single-center study, which could be expanded for a larger and more diverse sample. Another limitation was the participants’ lack of awareness regarding the importance of a carotid sonogram and some individuals feeling uncomfortable or hesitant to expose their necks during the procedure.
Conclusion
This large cohort study revealed significant findings regarding the association of CCA-IMT with hypertension, diabetes, age, and BMI. The results demonstrated a statistically significant difference in CCA-IMT between hypertensive (P < .05) and diabetic (P < .05) patients when compared to normal individuals. Moreover, a significant positive correlation was observed between CCA-IMT and age (P = .000) as well as BMI (P = .000). These study results may suggest that CCA-IMT could serve as a valuable diagnostic marker for assessing the impact of hypertension and diabetes on vascular health and aging-related changes. These study results should be replicated to provide further clinical evidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the University of Lahore’s Research Ethics Committee (REC-UOL-103-05-2023).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used.
Trial Registration
Not applicable.