
Abstract
Objective:
The aim of this study was to investigate the relationship between sonographic vascularity and echogenicity of the thyroid lobes, compared with a participant’s body mass index (BMI).
Materials and Methods:
A total of 3722 participations, with varied BMI, were included in the study. For all the participants, the thyroid-stimulating hormone (TSH) was measured, as well as thyroid volume, sonographic echogenicity, and vascularity were recorded. A multiple regression analysis was performed to assess the relationship between the sonographic vascularity and echogenicity, of thyroid lobes, compared with the participants’ BMI.
Results:
The serum TSH values were significantly higher in patients with a BMI > 25 kg/m². The sonographic vascularity and volume of thyroid lobes were positively correlated the participants’ BMI (P < .005). Sonographic heterogenicity of the left thyroid lobe, right thyroid lobe, and the isthmus were positively associated with BMI (P < .005). However, the hyper/hypoechogenicity did not demonstrate any significant correlation with BMI (P > .005).
Conclusion:
Based on the findings of this study, it was concluded that thyroid volumes may have a significant positive relationship with BMI. In overweight participants (i.e., BMI more than 25), thyroid echogenicity was more heterogeneous and their thyroid lobes were more hypovascular.
The prevalence of obesity has increased during the last decades, worldwide1,2 and obesity has been tripled from 3.2% to 10.8% in men and doubled in women from 6.4% to 14.9% between 1975 and 2016. 3 In developing countries like Iran, the burden of obesity increases in line with comorbid diseases. 4 Excess body weight is a predisposing factor for several diseases including diabetes, hypertension, cardiovascular disease, cancers, and all-cause mortality. 5 Obesity as defined by body mass index (BMI) has a protective effect on health and reduces all-cause mortality. 6
BMI may have influence on thyroid function tests. 7 The thyroid gland plays a main role in the control of energy metabolism by thyroid hormone actions.8,9 Several cross-sectional studies have shown a significant positive association between BMI and serum thyrotropin (thyroid-stimulating hormone, TSH).10-12 Obesity had many effects on the hypothalamic–pituitary–thyroid axis. Therefore, an intriguing cycle between obesity and thyroid could be hypothesized.8,9
Thyroid sonography is a valuable tool for diagnosing structural thyroid diseases and determining thyroid volumes and also is able to characterize the echographic structure of thyroid tissue. 13 This study was performed as a large cohort on volunteer employees within a medical science university, to determine if a relationship exists between thyroid volume and the BMI. Likewise, a secondary concern was whether there was a relationship between the sonographic vascularity and echogenicity of thyroid lobes and BMI. It was paramount to find out whether sonographic vascularity and echogenicity, of the thyroid parenchyma, and thyroid volume varied between participants. While performing sonography, some of the subjects showed sonographic hypoechogenecity or hypovascularity within the thyroid lobes, without other abnormal findings indicating a reasonable cause such as Hashimoto thyroiditis, subacute thyroiditis, and so on. It has been mentioned in the literature that hypoechogenecity of thyroid lobes may be seen in morbidly obesity patients. 14
Materials and Methods
Setting and Participants
This study sample was derived from the Persian organizational cohort study in Mashhad (POCM), which is an ongoing cohort investigation of risk factors for non-communicable diseases (e.g., cardiovascular events). The POCM includes extensive information on baseline status and regular check-up of 12000 employees (aged 30–70 years) in different organizations in Mashhad, northeast of Iran. Detailed national protocol has been published 15 The informed consent was obtained from participants prior to the baseline assessment. The study protocol was in accordance with the principles outlined in the Helsinki declaration. This study was approved by the national and regional ethics committee (IR.MUMS.REC.1395.526; January 2017).
Study Measurements and Clinical Assessments
All of the laboratories values, in POCM, including serum TSH measurements were performed after 10–12 hours fasting in the morning (BT1500 auto analyzer, Biotechnical Instruments, Rome, Italy).
The thyroid sonogram was performed by three expert examiners, by means of the same ultrasound equipment system (Affiniti 50, Philips), with a linear-array transducer (7–12.5 MHz). The patients were instructed to lay in a supine position with their neck hyperextended. The size of the thyroid lobes, as well as the isthmus, were measured in centimeters at maximum diameter, on the basis of a longitudinal, antero-posterior, and transverse planes. The volume of the thyroid, as has been assessed by measuring the three largest perpendicular diameters. Total thyroid volume was determined by adding up the volume of isthmus to left and right lobes. Echogenicity of the thyroid was categorized as homogenous and heterogeneous. Hypo-echogenicity was defined as thyroid echogenicity less than echogenicity of strap muscles. 16 The vascularity of the thyroid lobes was assessed with color Doppler (CD). Hypervascularity was defined as the thyroid tissue demonstrating more than three vessels with CD and vascularity of the lobe, more than what was expected as usual for a normal thyroid gland, as our expert ultrasonographer’s point of view. Hypovascularity was defined when the vascularity of thyroid parenchyma was comparatively lower than a strap muscle’s vascularity.
The body composition test was performed using the InBody 770 body analyzer (InBody Corporation, Seoul, South Korea). This machine sends a weak alternative current (50–1000 kHz) and determines the mass of different body tissues by measuring the reflected current. It also calculates the BMI: (BMI formula) kg/m2 is a person’s weight in kilograms and m2 is height in meters squared. A BMI of 25.0 or more is considered overweight, compared with a healthy BMI range of 18.5–24.9. The participants were required to stand motionless keeping the standard position (e.g., standing barefoot on the footplates while holding hand electrodes with straight arms and no touches in the armpits area). The height was measured to the nearest one decimal point in centimeters, while the participant was shoeless and had light underclothes. Participants who were pregnant or had an implanted pacemaker were excluded from the body analysis.
Statistical Analysis
Statistical analyses were performed using the R studio (version 3.5.3, R Core Team, 2019). Descriptive data are presented as the number of observations and percent (for qualitative variables) or as the mean, standard deviation (+SD), and 95% confidence interval (95% CI) for quantitative variables. Comparisons of categorical variables was conducted using a chi-square test. The analyses of continuous variables were completed using an independent-samples t-test and Mann–Whitney U test. Univariate and multivariate logistic regression analysis were used to estimate the impact of BMI > 25 kg/m² on the sonographic vascularity and echogenicity of thyroid in patients. A stepwise method of multivariate logistic regression analysis (with P < .05 as an entrance criterion and P > .1 as a removal criterion) was conducted. Age and serum TSH level were used as confounding factors.
Results
The comparison of demographic, clinical, and pathological features, in this cohort, was made with the categories of normal weight (BMI<25 kg/m²) and overweight +obese people (BMI ≥ 25 kg/m²) (see Table 1). The sample cohort consisted of 3722 participants including 1738 (46.7%) males and 1984 (53.3%) females, with a mean age of 46.16 ± 9.50 years. Within this cohort, 1171 participants had a normal weight (BMI<25 kg/m²) and 2551 participants were either overweight or obese (BMI ≥ 25 kg/m²). The mean age was significantly lower in the group with BMI <25 kg/m² than in the group with BMI ≥ 25 kg/m² (P = .005). A serum TSH was significantly higher in patients with BMI > 25 kg/m² than in patients in the BMI < 25 kg/m² group (P < .05 for both) and differences in the levels of TSH, between the two groups were statistically significant (P < .05 for both). The sonographic vascularity and volume of the thyroid lobes were positively correlated with amount of BMI (P < .005). The sonographic heterogenicity within the left lobe, right lobe, and the isthmus of thyroid were positively associated with amount of BMI (P < .005). Interestingly, the sonographic hyperechogenicity and hypoechogenicity did not demonstrate a significant correlation with BMI (P > .005). The univariate and multivariate logistic regression analysis of BMI is provided (see Table 2). Overweight and obese participants had a significantly higher rate of increased sonographic vascularity in the right thyroid lobe of thyroid compared with participants with a normal weight. The statistical analysis indicated that a BMI ≥ 25 kg/m² was not significantly associated with abnormal sonographic echogenicity (P > .05).
The Demographic and Clinical Characteristics of the Total Group of Participants, As Well As the Two Subgroups, Based on BMI Group. The Data Is Presented as the Number of Observations (Percent) or the Mean With Standard Deviations (+SD).
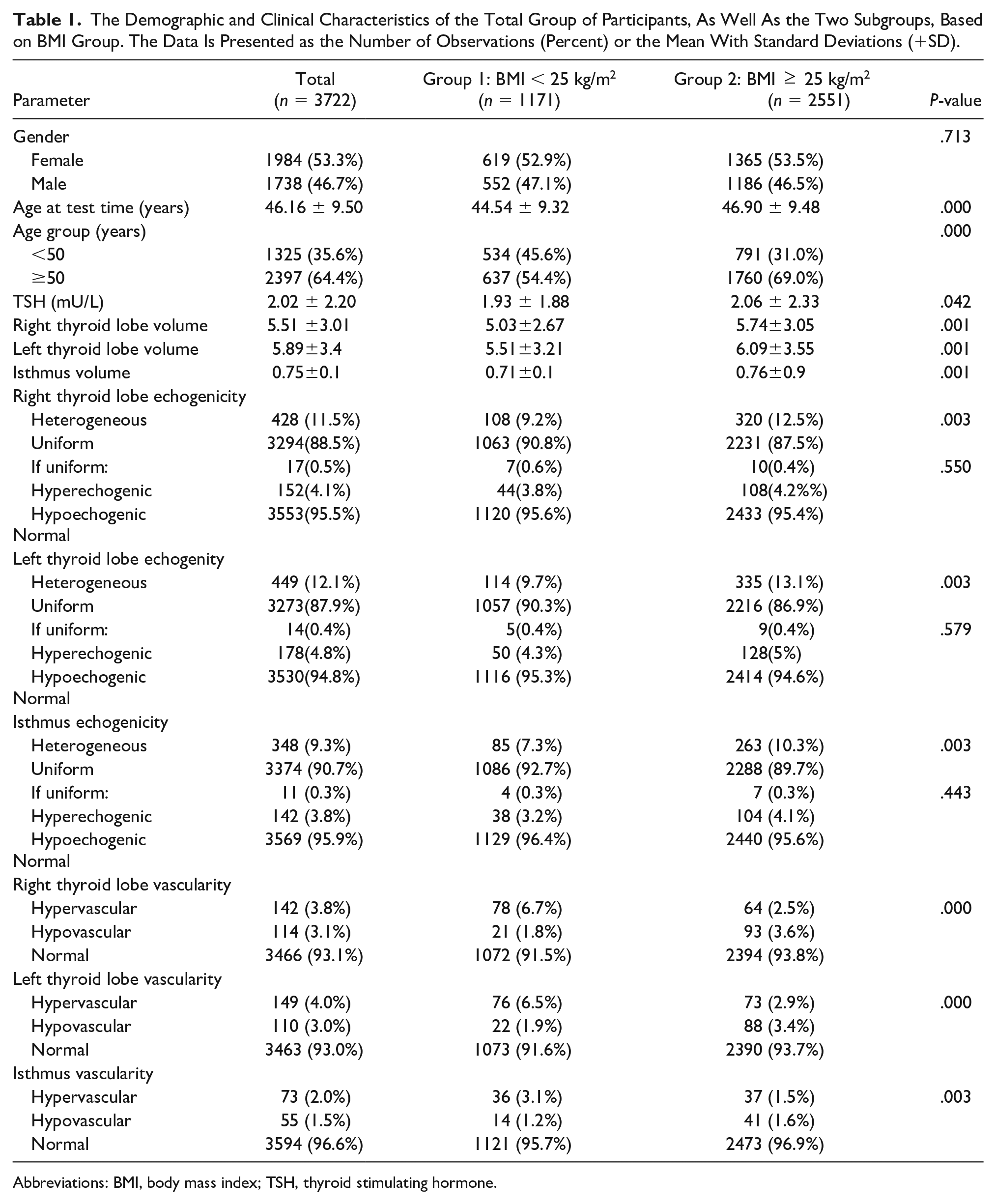
Abbreviations: BMI, body mass index; TSH, thyroid stimulating hormone.
The Univariate and Multivariate Logistic Regression Analysis of Participants Who Had a BMI > 25 and Their Thyroid Imaging Outcomes.
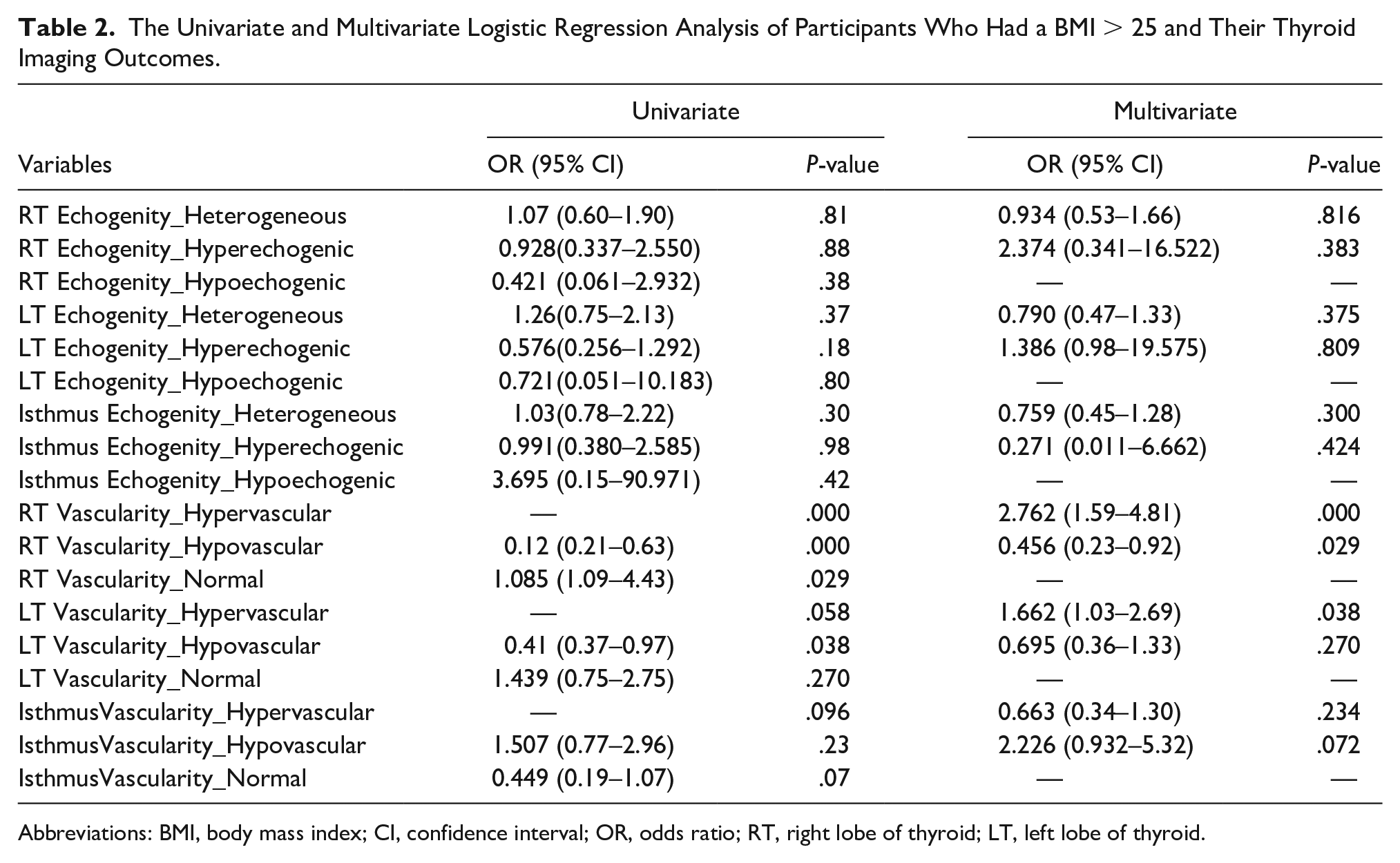
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; RT, right lobe of thyroid; LT, left lobe of thyroid.
Discussion
Sonography is a valuable diagnostic tool in the evaluation of the thyroid gland. It is possible to detect some abnormalities in the thyroid’s glandular structure, such as detecting nodules, hypo- or hyperechogenicity of the thyroid tissue, sonographic vascularity of within the lobes, and calculate the thyroid volumes, by utilizing sonography.13,17
Vascular assessment of thyroid parenchyma was based on the Doppler assessment. In this study, the patient’s thyroid vascularity was evaluated and there was a significantly positive correlation between the graded vascularity of the right thyroid lobe with BMI (P < .005). Vita et al found that thyroid vascularization correlated directly with thyroid volume and that a larger thyroid tended to be more vascular. 13 In another study, Ramazan et al showed a positive correlation between thyroid volume and body weight, compared with BMI and body fat percentage. 18 In that study, they showed that after 6 months of treatment of obesity, volume of thyroid decreased only in women who lost more than 10% body weight. 18
There are other reports that have shown correlation between increasing thyroid volume and increasing BMI.17-20 This study was in concordance with the results of the previous research provided. It would appear that sonographic heterogeneity, of the thyroid gland, is a nonspecific finding and it can be seen in conditions that diffusely affect the thyroid gland, such as Graves’ disease and Hashimoto thyroiditis.
In this study, a BMI > 25 was not significantly associated with sonographic hypoechogenicity of the thyroid. However, there was a positive correlation between the sonographic heterogeneity and echogenicity of the thyroid compared with BMI. As is evident from literature data, obese patients are more likely to have a hypoechoic appearance of the thyroid, when examined with sonography. Capturing a hypoechoic image of the thyroid, with sonography, is considered a diagnostic indicator of autoimmune thyroiditis. According to this study, it can be concluded that the hypoechogenecity of these participants’ thyroid tissue was more frequently seen by those who were deemed to be obese or overweight but not necessarily indicating Hashimoto thyroiditis. This was proven due to the relatively significant number of participants with thyroid hypoechogenecity, lacking other characteristic ultrasonographic features of Hashimoto thyroiditis, in this study.
Rotondi et al showed that a sonographically hypoechogenic thyroid, without negative antithyroid antibodies, was observed in 1.9% of nonobese patients, compared with 64.8% of obese individuals. 14 This may strongly indicate that hypoechogenicity of thyroid parenchyma, utilizing sonography, among obese patients has other causes, beyond autoimmunity. One explanation may be metabolic inflammation of thyroid gland. Otherwise, adipose tissue releasing cytokines may lead to vasodilation and more permeable blood vessels in thyroid 21 Another explanation that has been suggested is the accumulation of adipose tissue in thyroid gland. 21
In this study, serum TSH was significantly higher in patients with BMI > 25 kg/m2 than in patients with BMI < 25 kg/m2. This finding is consistent with other numerous prior studies that have reported higher blood levels of TSH in obese patients. García-Solís et al have explained in detail that they believe that a central resistance to locally produced FT3 results in increase of TSH level in obese individuals and this represents as an adaptive process to increase basal energy expenditure. 22 In another study, Betry et al showed that leptin levels correlate with TSH positively. So, another explanation of high levels of TSH in obese patients may be the effect of high concentration of leptin in them. 23
Limitations
There were several limitations to this study and the main was the cohort being purposively drawn from the larger study. The threats to internal and external validity make these results only applicable to this cohort. An added challenge was that this study lacked information regarding complete thyroid function tests (TFT) and anti-thyroid antibody concentrations in these participants, especially antithyroperoxidase antibody. Future studies should consider that these imaging results were generated by three expert sonographers, and it would be limit variability to have a single sonographer to achieve precision and reproducibility of the methods.
Conclusion
This study was a retrospective epidemiologic investigation, performed on a large cohort of participants. It was noted that a recorded BMI of more than 25 was frequently associated with older participants. In addition, it was found that in participants with a BMI more than 25, their sonographic thyroid echogenicity was more heterogenous and the right thyroid lobe was more hypervascularized, compared with leaner participants. The measured thyroid volumes had a significantly positive relationship with BMI. Likewise, the sonographic hypoechogenicity of thyroid lobes was frequently noted in obese and overweight participant, which does not necessarily indicate Hashimoto thyroiditis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.