
Abstract
Objective:
Work-related musculoskeletal disorders (WRMSDs) are injuries developed through repetitive use or strain. These may lead to an early career-ending injury. Work-related burnout has also been documented among sonographers, but the potential relationship between WRMSDs and burnout has not been well studied.
Material and Methods:
A 43-question survey was sent to sonographers and included questions regarding work culture, presence of WRMSDs, early career-ending injury, and occupational burnout. The Oldenburg Burnout Inventory was used to determine gauge occupational burnout.
Results:
Of 127 respondents, 64% (n = 81) reported a WRMSD and 76% (n = 96) self-reported occupational burnout. The total burnout score was 3.3 points higher among those reporting a WRMSD, compared with those not reporting. (P = .0077).
Conclusion:
Work-related musculoskeletal disorders and occupational burnout were associated conditions among this group of sonographers. Hospital and clinic administrators should listen to employees to identify potential occupational burnout or a WRMSD, prior to either condition resulting in an exit from the profession.
Keywords
Work-related musculoskeletal disorders (WRMSDs) are injuries caused in the workplace and develop over time by repetitive use or strain. 1 The condition was first reported among sonographers in 1985 2 and subsequent studies have since been conducted.3 –5 These injuries may begin with minimal pain being noted during work but progresses and lasts beyond the end of the workday.3,6 The problem affects sonographer health, job satisfaction, and, in some cases, the injury necessitates an earlier than planned exit from the profession. 3
Pike et al 3 conducted the first comprehensive study of the prevalence of WRMSD and reported that 81% of sonographers were working in pain. Of those working in pain, 20% of them were injured to the point of leaving the profession. 3 In a follow-up study with a different cohort of respondents, Evans et al 4 reported that 90% of sonographers were scanning in pain, which was a 9% increase in prevalence. Notably, in this survey, 54.5% of respondents received education on how to adjust equipment and use ergonomic principles when conducting sonography. 4 In the 2023 report by Roll et al, 5 they noted that, among a sample of 3592 respondents, 98.2% had reported musculoskeletal pain, while working, within the past year. Between 44% and 61.6% of the respondents indicated the pain interfered with daily activities and there were 86% of this cohort of sonographers who also experienced discomfort related to their occupational work. 5
To prevent WRMSDs, the profession’s response has centered around increasing education, encouraging manufacturers to redesign ultrasound equipment systems to include ergonomic features, encouraging sonographers to take responsibility for maintaining good ergonomics during the workday, and emphasizing sonographers’ personal responsibility for maintaining good personal fitness and health. To facilitate these initiatives, it requires that manufacturers create ergonomic equipment and that administrators provide the education, as well as the equipment. However, the primary responsibility is on the sonographer to prevent WRMSDs through use of the equipment, applying the education, and maintaining good personal health and fitness.
Evans et al 4 reported in 2009 that manufacturers had implemented ergonomic designs and features into ultrasound equipment systems; therefore, the Commission on Accreditation of Allied Health Education Programs required, in 2011, that educational programs may be designed to teach the importance and practice of ergonomics to students. The instruction was to include proper personal fitness, support tools, equipment, and patient positioning. 7 The impact of this educational programming is questionable as Scholl and Salisbury 8 noted that, within sonography education programs, students and recently graduated sonographers may not be following these ergonomic recommendations.
The recommended guidelines and educational programs promoting personal physical fitness are widely available.9,10 Research on the implementation by sonographers has focused on stretching, yoga, biofeedback, and mindfulness as ways to prevent WRMSDS.11 –14 To date, these interventions have shown modest results; however, owing to the use of small sample sizes, lack of a control group, and minimal long-term results, it is difficult to determine the effectiveness of these interventions.11 –14 Interventions that rely on the participants to maintain these personal changes have generally shown that participants either cannot or will not continue implementing change, regardless of their early sucesses.15 –19
Sommerich 20 described a new paradigm to study how sonographers could address the risk of WRMSDs. She proposed a sociotechnial systems approach in which the entire work system, including the sonographers, should be working toward a solution to improve worker safety. 20 To study the entire work system with this approach, every perspective is considered, including the psychosocial factors contributing to WRMSDs. Overall sonographer health, sonographer well-being, and workplace culture, such as autonomy at work, workload, and administrative support, are also considered components of the system. 20 This approach provides an alternative view of the risk of injury and, in this model, the sonographer does not bear the primary responsibility for prevention, but rather it is shared by all stakeholders in the work system. 20
The prevalence of sonographers working in pain has not decreased over a 25-year period regardless of advances in ergonomic equipment design, education, and available prevention programs. Education, personal responsibility, and fitness as prevention techniques do not appear sustainable. It may be time for the profession to explore the psychosocial aspects of workplace culture that may be contributing to WRMSDs and find new interventions to prevent them.
Occupational burnout is described as work-related stress or exhaustion that can develop into a debilitating psychological state causing emotional exhaustion, depersonalization, and an overall decreased sense of achievement. 21 Staff shortages, compassion fatigue, work conditions, long work days, low job satisfaction, and lack of employee appreciation are all factors that contribute to occupational burnout. 22 Burnout has an adverse effect on interpersonal skills between the sonographer and attending physician, patient care quality, and examination errors, which can lead to litigaton. 23
The research indicates that medical imaging professionals experience high levels of occupational burnout. 24 In particular, the prevalence of burnout in sonographers 25 has been reported as high as 92%. Factors that contribute to burnout among sonographers include the following: the operator dependence of sonography, overtime and on-call work, scheduling pressures, the need to stay current with technology, and being prone to WRMSDs. 24 The issues of workplace culture that may be an important factor that impacts WRMSDs and burnout simultaneously include insufficient time allocated for examinations, examinations with high cognitive demands, lack of control over the schedule, increasing documentation expectations, and an inability to take breaks during the day.24,25 Pike et al 3 suggested that a stressful work culture can contribute to physical exhaustion, pain, and injury, and affect mental well-being. Harrison and Harris 26 further suggested that the psychosocial factors of work contribute to WRMSDs due to exhaustion and fatigue.
Since both occupational burnout and WRMSDs may affect a sonographer’s ability to perform daily tasks, finding solutions to manage burnout and WRMSDs among sonographers is critical to minimize the number of workers who are injured and leave the profession. The occupational burnout rate among sonographers, and the associative relationship between WRMSDs has been proposed, but not established. The goal of this study was to determine whether there are associations between WRMSD, occupational burnout, and sonographers taking an early exit from their career. The knowledge gained from this work may assist administrators and sonographers with methods to improve sonographer’s well-being, reduce the risk of WRMSDs, and prevent an early exit from the career.
Materials and Methods
The project was reviewed by the host institution’s institutional review board (IRB) and was granted exempt status. A closed, anonymous survey consisting of 43 questions, regarding demographics, work culture, presence of WRMSDs, occupational burnout, and an early exit from the career exit, was created with the Qualtrics XM online survey software. The survey was pilot tested among a subset of university faculty to review for question errors such as grammar and question flow. The survey was e-mailed to 505 diagnostic medical sonographers who are affiliates of a southwestern diagnostic medical sonography program who serve as clinical instructors for the program and were registered in the education program’s clinical database management system. The survey link was available for 20 days from October 2022 to November 2022. Three reminders were sent after the first week, the second week, and the weekend before the survey closed.
The IRB required a screening question to verify that the respondents were at least 18 years of age. Questions 1 through 5 asked work demographic questions, including years of practice, most scanned specialty, typical numbers of patients a day, hours worked a week, and call hours worked per week. Questions 6 through 15 were related to scanning in pain, how it affects job satisfaction, and early retirement from the field. Questions 16 through 19 were related to work-related burnout. Question 20 asked the sonographer how much longer the participant planned to work as a sonographer. Questions 21 through 36 included the Oldenburg Burnout Inventory (OLBI) items, and Questions 37 through 43 were personal and health-related demographics (see supplemental material for the full survey).
Frequencies and percentages of sonographers working in pain, reporting occupational burnout, and OLBI scores were analyzed and compared with previous studies. The OLBI scores were analyzed for normality assumptions among sonographers who reported working in pain and those who did not. A student t test was used to compare OLBI scores among sonographers who reported working in pain and those who did not.
A multivariate linear model was constructed to determine whether demographic and workplace variables influence the relationship between working in pain and OLBI scores. A second multivariate model was used to analyze variable associations with the question regarding how many years a sonographer plans to continue working in the occupation. Both multivariate linear models controlled for age since increased age has been associated with levels of occupational burnout and influences their remaining working years. All statistical tests assumed a 5% chance of a Type I error. For the analysis, SAS 9.4 (Carey, NC, USA) was used. Sonographers with higher pain levels were hypothesized to have higher OLBI scores (see Table 1, which outlines the statistical approach).
A Description of the Statistical Approach Used in This Survey Research.
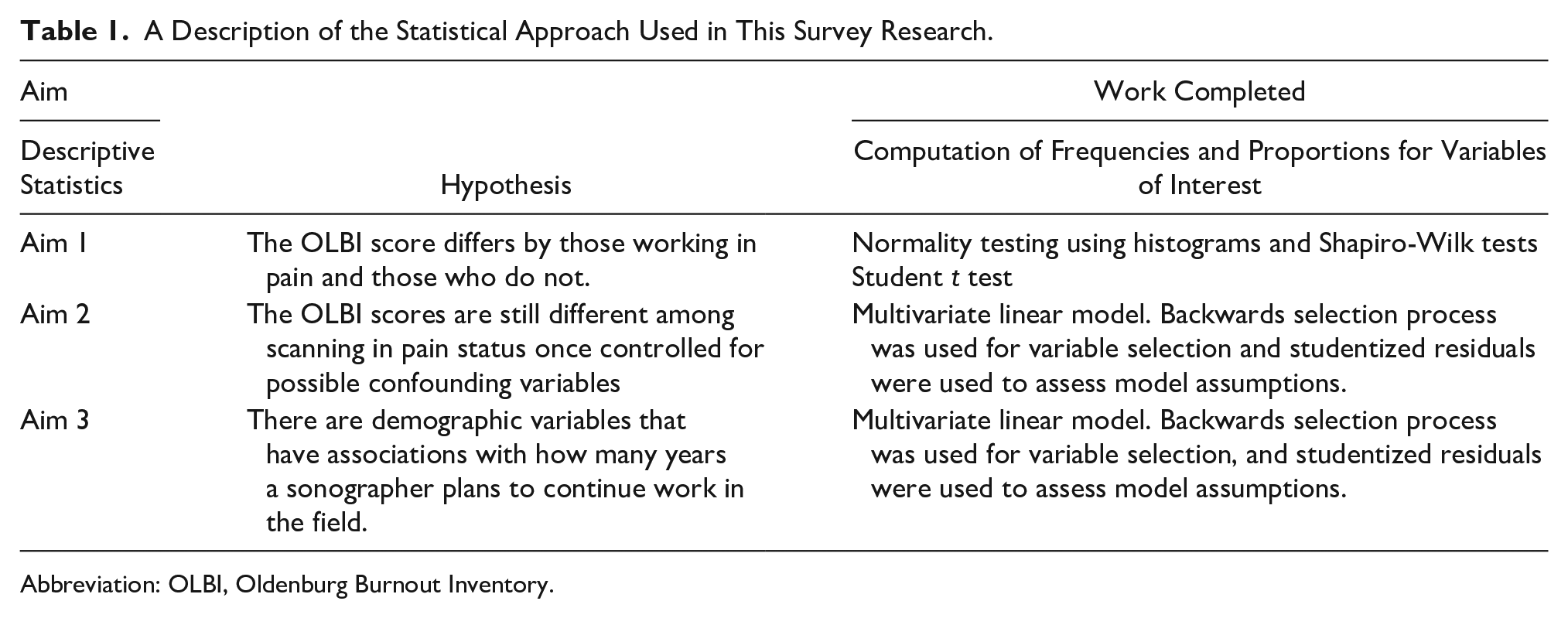
Abbreviation: OLBI, Oldenburg Burnout Inventory.
Results
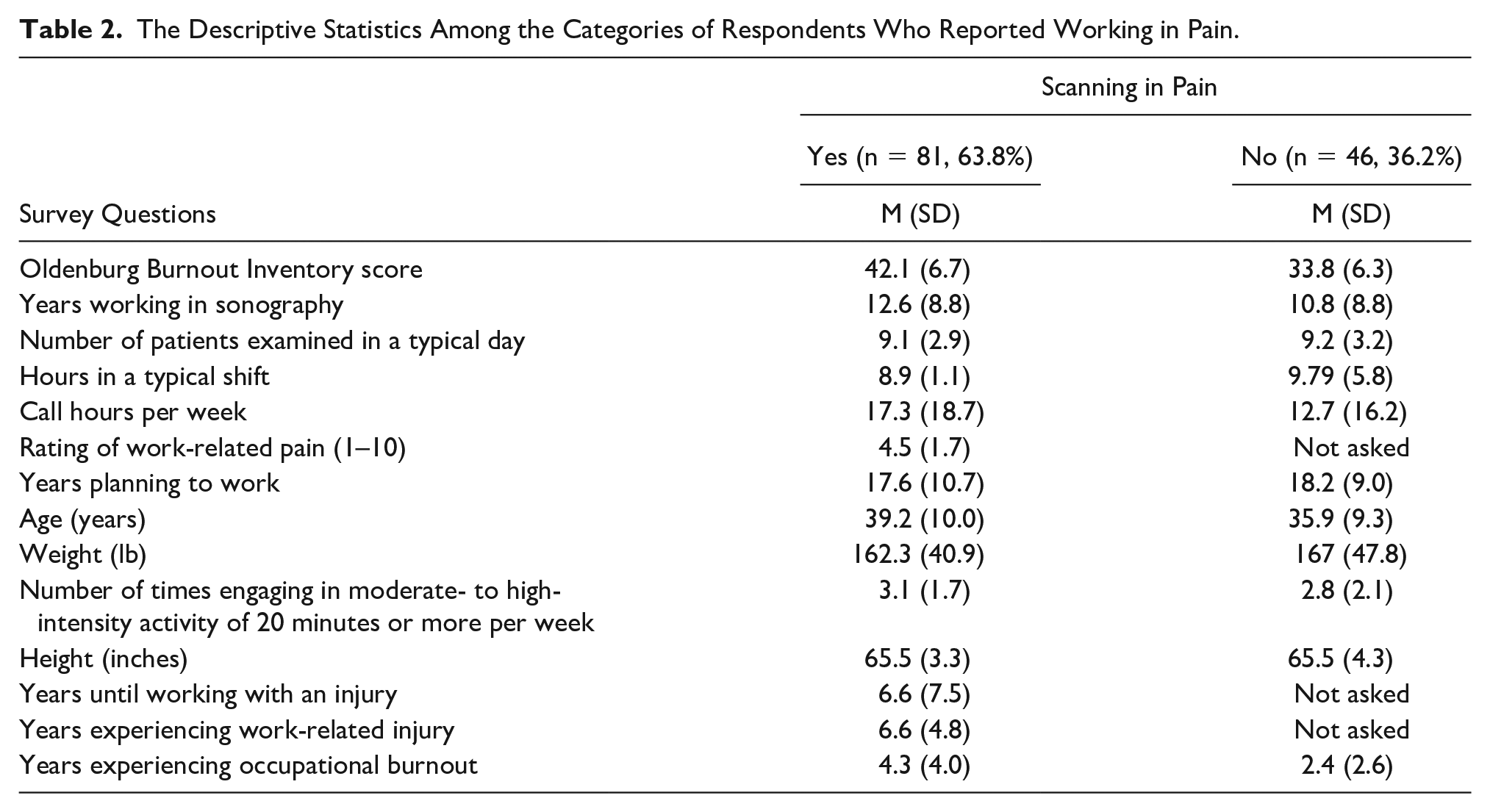
A total of 127 completed responses were recorded out of 505 survey recipients, for a 25% response rate. Descriptive statistics strata were computed for all variables in the data set (see Table 2). Sixty-four percent (n = 81) of sonographers reported working in pain, and 75% (n = 96) self-reported occupational burnout. The total OLBI score was 3.3 points (95% CI, 0.9–5.7) higher among those reporting working in pain compared with those who did not report working in pain (P = .0077; see Figure 1). The total OLBI score was 9 points (95% CI, 7–11) higher among respondents with self-reported occupational burnout compared with those respondents who did not self-reported burnout (see Figure 2).
The Descriptive Statistics Among the Categories of Respondents Who Reported Working in Pain.
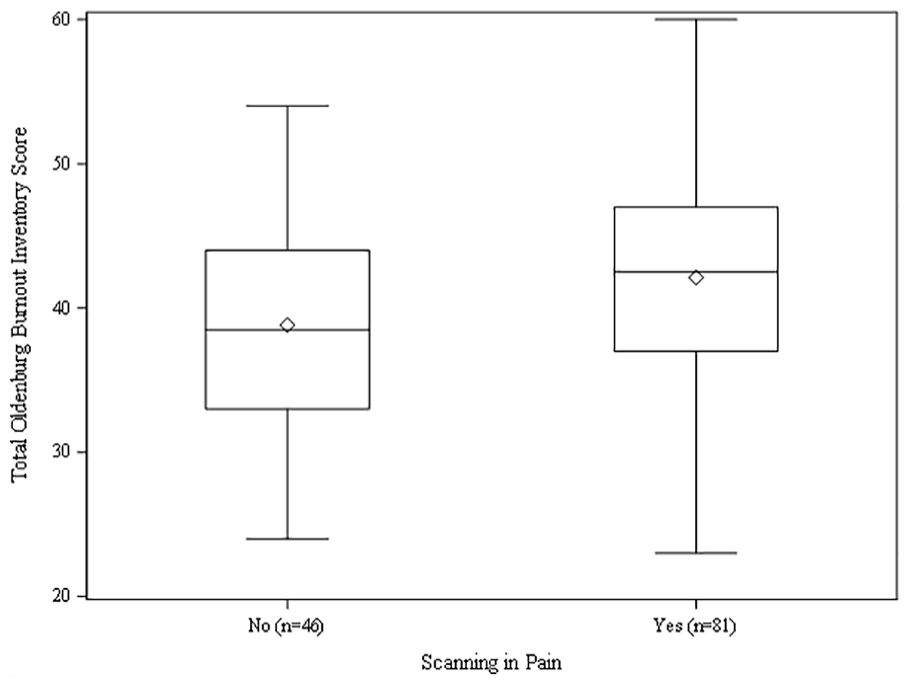
A box plot of the data related to the total Oldenburg Burnout Inventory scores compared with participants indicating whether they were working in pain.
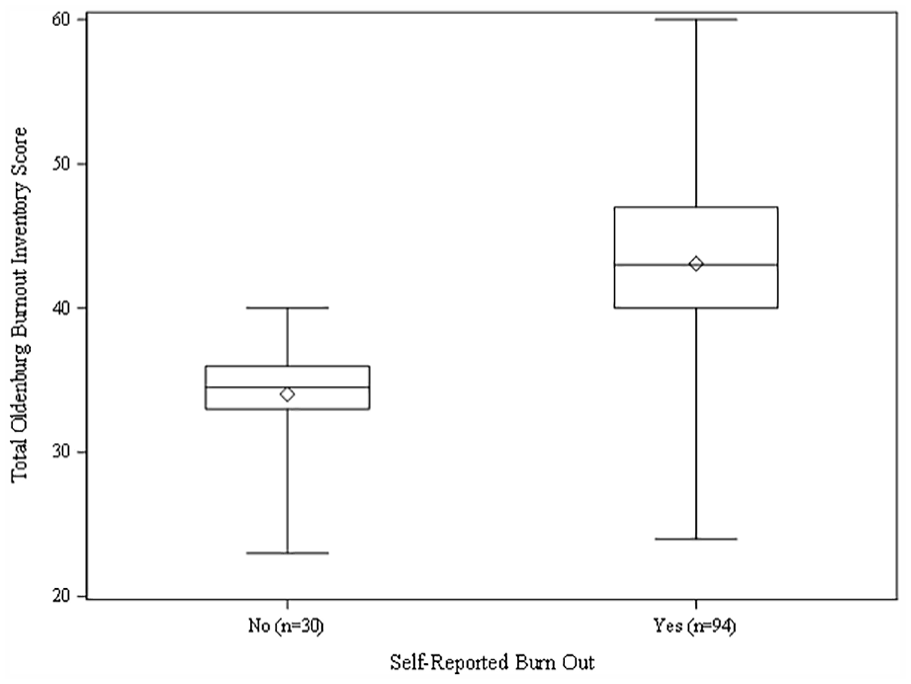
A box plot of the data related to the total Oldenburg Burnout Inventory scores compared with participants indicating whether they were experiencing occupational burnout.
The first multivariate analysis compared the influence of variables on working in pain and the total OLBI scores. Variables with nonsignificant P values eliminated from the multivariate analysis included the following: years working in sonography, the number of hours worked during a typical shift, the number of call hours per week, weight, height, self-rating of pain level, the number of years until the pain began, the number of years working with the pain, and the number of years experiencing self-perceived work-related burnout. The model was adjusted for the number of patients seen in a typical day, age, number of years the individual planned to remain in sonography, and the number of moderate- to high-intensity activities performed per week. After this adjustment, self-reported pain with conducting sonography was associated with a 3.2 (95% CI, 1.0–5.4) higher occupational burnout score (P = .0041), and respondents with more days per week participating in moderate- to high-intensity exercise of 20 minutes or more per week had higher OLBI scores (P = .0025; Table 3). A second multivariate model analyzed variable associations of how many years a sonographer plans to continue working in the field, and two significant variables were found: age (P = .0003) and total OLBI score (P =< .0001). After adjusting for these two variables, working in pain was not associated with a sonographer’s expectation to remain in the field (P = .2187).
The Total OLBI-Adjusted Multivariate Model Results.
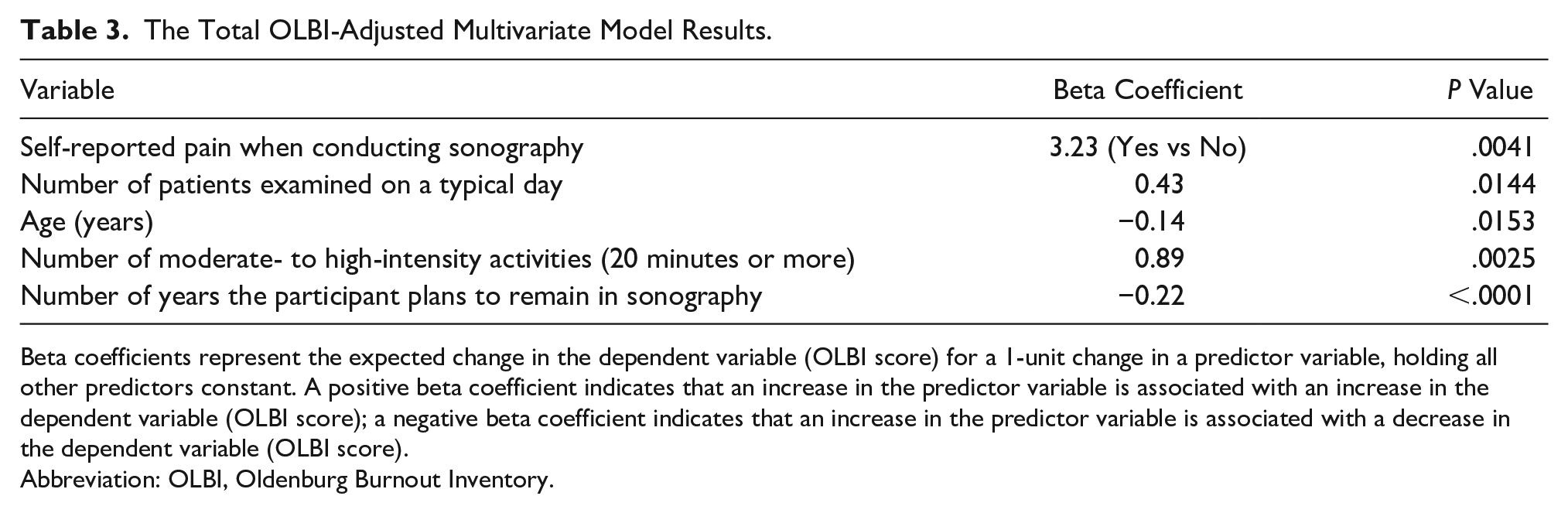
Beta coefficients represent the expected change in the dependent variable (OLBI score) for a 1-unit change in a predictor variable, holding all other predictors constant. A positive beta coefficient indicates that an increase in the predictor variable is associated with an increase in the dependent variable (OLBI score); a negative beta coefficient indicates that an increase in the predictor variable is associated with a decrease in the dependent variable (OLBI score).
Abbreviation: OLBI, Oldenburg Burnout Inventory.
Descriptively, respondents who were not working in pain reported a mean of 10.8 years in the profession and expected to remain in the profession for 18.2 years on average, whereas respondents in pain reported working an average of 12.6 years in the occupation and planned to work 17.6 years in the profession. When asked about whether working in pain had changed their future perspective, 80% of those who were in pain also reported that their future perspective had changed. Participants were asked to comment on variables, besides pain that impacted how they felt about their future in the profession. Comments fell into categories predominantly related to work-place culture, as follows: increasing workload, lack of raise in pay, patient attitude toward sonographers, absence of advanced opportunities in sonography, lack of engagement with physicians, and increasing number of difficult studies due to patients with a high body mass index.
Discussion
Sonographers are at high risk of WRMSDs.3 –6 These injuries can be devastating to a sonographer’s health and well-being, job satisfaction, and career longevity. 3 Despite education and ergonomic equipment availability, the prevalence of risk of WRMSDs among sonographers has not declined. This research supports Sommerich’s proposal that the key to prevention may lie in evaluating the problem with a systems approach. 20 Underscoring contributing factors, besides personal responsibility, could help sonographers reduce the primary burden of WRMSD prevention.
Compared with the studies by Pike et al, 3 Evans et al, 4 and Roll et al, 5 this research demonstrated a lower prevalence of WRMSDs among sonographers with 64% (n = 81) compared with 81%, 3 90%, 4 and 86%, 5 respectively. The participants in this study were younger compared with those in the studies by Pike et al 3 and Evans et al 4 and these participants were geographically concentrated in the southwestern region of the United States. The survey was only sent to sonographers in two urban areas, within one southwestern state, and they had to be registered in the host sonography educational program’s clinical affiliate database. This cohort of sonographers may be different compared with sonographers from other areas of the country, which may not be immediately apparent. The study had a 25% response rate, which was lower than in the studies by Pike et al, 3 Evans et al, 4 and Roll et al. 5 The response rate may further hamper the results and emphasize that these results are unique to just this cohort.
The OLBI measured levels of occupational burnout, and this inventory has demonstrated acceptable reliability and validity in previous studies. 27 The inventory focuses on two core dimensions of burnout: disengagement and exhaustion from work, using positively and negatively formulated items. There are 16 items in the inventory, 28 for a total possible score ranging from 16 to 64. The model developers considered occupational burnout on a continuum and did not include cutoff scores or categories of burnout, but suggested that the higher the score, the higher the level of burnout. 28
The percentage of sonographers self-reporting occupational burnout in this study is lower than the rate reported in the studies by Singh et al 24 and Skelton et al. 25 In this study, the total OLBI score was statistically higher among sonographers reporting a WRMSD, when compared with those who did not report an injury; however, 75% of sonographers self-reported occupational burnout. This finding indicates that there may be an association between developing a WRMSD and occupational burnout, but it does not provide a time line of when these conditions developed. Thus, a causal relationship between these two variables is not established. Furthermore, the OLBI score was the most related variable to indicate an early exit from the career (P < .001) rather than WRMSDs. This finding may demonstrate that occupational burnout should be considered when considering the risk and occurrence of WRMSDs.
A surprise result was noted in this study that the more days of moderate- to high-intensity activities (20 minutes or more), performed in a week, the higher the total OLBI score (P = .0025). This finding is concerning, since physical fitness and well-being are essential tenets of WRMSD prevention. Exercise is often advised for stress relief and improving mental health. While this study is not designed to explore this relationship, it suggests at least two possibilities: the respondents were experiencing occupational burn out and chose exercise to improve their mental well-being and/or health, or they found it stressful to maintain exercise on top of a busy schedule. Other alternative explanations may exist to explain these results. A critique of the question is that moderate- to high-intensity activity was not defined in this survey tool. This question represented a variation in the questions asked on the National Health and Nutrition Examination Survey which has two questions, one for moderate activity and one for vigorous activity performed in a week. 29 There may have been wide variability in how respondents defined moderate- to high-intensity activities, which may have influenced the finding in ways not detected in the analysis.
Limitations
The major limitation to this study was the research design, which has threats to internal and external validity. Another weakness in this research is the lack of definition of general health for the respondents. Some respondents may have believed it included mental health while others may have only responded with regard to physical health. The effect on the responses is unknown; however, the comparisons made in this study did not include a reference to mental health, so any confusion from the respondents for this question may not have impacted the analysis. Self-selection bias may also be present in this survey. Respondents who were in pain or reported burnout may have been more willing to take the survey due to identifying with the topic. The percentage of respondents who reported working in pain was less than that reported in the studies by Evans et al 4 and Roll et al, 5 and if participants who were uninjured had taken the survey, it may have further reduced the number working in pain. Finally, this research was conducted during the postpandemic period. Hence, it is likely that the stress that health care workers experienced during the pandemic affected the OLBI scores in this research. Longitudinal research could be conducted on burnout to determine whether the rates remain steady or decline to prepandemic levels in the future.
Future research can explore the temporal relationship between WRMSDs and occupational burnout; whether a WRMSD contributes to occupational burnout and vice versa. In addition, researchers can refine the question regarding moderate- to high-intensity activities per week to determine whether that relationship truly exists. More research is needed on whether working in pain or occupational burnout is related to a sonographer’s decision to leave the profession early. Exploration of burnout as a contributing factor may provide additional insights to the WRMSD epidemic. Findings in this research suggest that exploring psychosocial factors of work and work culture may offer new insights to potential causes and solutions that move beyond the initial approach of education, engineering, and personal responsibility.
Conclusion
Sonographers have a high risk of WRMSDs, and the number of sonographers working in pain continues to increase despite increased education and awareness. Along with WRMSDs, sonographers are impacted by occupational burnout. This research demonstrated that, in this cohort, WRMSDs and occupational burnout were associated conditions. Knowing that this relationship may exist in other work groups may allow hospital and clinic administrators to be proactive when evidence of occupational burnout or WRMSDs is noted. This awareness could provide an opportunity to create departmental solutions that address pain reduction, occupational burnout, and avoid an early exit from the occupation. Reducing the number of career-ending incidents will greatly contribute to solving sonographer shortages as well as reducing the risk of WRMSDs and occupational burnout among the staff who continue working in the clinical department.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231211325 – Supplemental material for Exploring the Relationship Between Sonographers’ Work-Related Musculoskeletal Disorders and Occupational Burnout
Supplemental material, sj-docx-1-jdm-10.1177_87564793231211325 for Exploring the Relationship Between Sonographers’ Work-Related Musculoskeletal Disorders and Occupational Burnout by Jennifer E. Bagley, Danielle Amos and Jonathan D. Baldwin in Journal of Diagnostic Medical Sonography
Footnotes
Ethics Approval
Ethical approval for this study was waived by the host institution’s institutional review board (IRB) because the study did not collect PHI or other identifying information and involved no more than minimal risk to participants.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.